

Abstract
OBJECTIVE: In a cardiothoracic and vascular intensive care unit, to compare nasal high-flow (NHF) oxygen therapy and standard high-flow face mask (HFFM) oxygen therapy in patients with mild to moderate hypoxemic respiratory failure.
METHODS: In a prospective randomized comparative study, 60 patients with mild to moderate hypoxemic respiratory failure were randomized to receive NHF or HFFM. We analyzed the success of allocated therapy, noninvasive ventilation rate, and oxygenation.
RESULTS: Significantly more NHF patients succeeded with their allocated therapy (P = .006). The rate of noninvasive ventilation in the NHF group was 3/29 (10%), compared with 8/27 (30%) in the HFFM group (P = .10). The NHF patients also had significantly fewer desaturations (P = .009).
CONCLUSIONS: NHF oxygen therapy may be more effective than HFFM in treating mild to moderate hypoxemic respiratory failure.
Introduction
High-flow oxygen therapy is a routine treatment for hypoxemic respiratory failure in extubated, self-ventilating patients in the intensive care unit (ICU). This therapy is traditionally delivered via a face mask rather than nasal cannula, because of the flow limits of traditional nasal cannula (4–6 L/min)1,2 and the tendency for patients in respiratory distress to breathe through their mouths. Optiflow (Fisher & Paykel Healthcare, Auckland, New Zealand) is a new nasal high-flow (NHF) oxygen system that allows the delivery of up to 60 L/min of heated and humidified, blended air and oxygen via wide-bore nasal cannula. The system conditions the inspired gas to 37°C and 44 mg H2O/L, which is considered thermodynamically neutral to the airway,3 preserving the function of the ciliated mucosa.4 Recent work described complications associated with unhumidified high-flow face mask (HFFM) oxygen therapy, which include discomfort and airway drying.5
Following the introduction of NHF oxygen therapy into our ICU, we found that patients tolerated NHF well, that NHF obviated NIV in some cases, and that NHF patients remained well oxygenated, even with open-mouth breathing. Work by Wettstein and colleagues supports those observations and suggests that the mouth may act as an anatomical reservoir for oxygen in some cases.6 We also believed that NHF has facilitated early ICU discharge, because it can be managed effectively in the postoperative ward. We hypothesized that NHF would also improve the success of oxygen therapy and improve oxygenation.
Studies in healthy volunteers showed that NHF can deliver an accurate FIO27,8 and generate positive nasopharyngeal pressure, which increases with increased gas flow.7,9 This positive and linear relationship between flow and pressure was further substantiated in a cardiothoracic ICU population.10,11
The objective of this clinical study was to evaluate whether NHF would be better tolerated and with fewer treatment failures than HFFM in patients with mild to moderate hypoxemia.
Methods
We conducted a prospective randomized comparative study in our 24-bed cardiothoracic and vascular ICU. Our regional ethics committee approved this study. Funding for the study was provided by Fisher & Paykel: they supplied the Optiflow circuits used in this study, and they paid for the statistical analysis. All 3 authors designed the study and were responsible for data collection, analysis, and writing the paper. The authors consulted employees of Fisher & Pakel Healthcare regarding study design and data analysis.
Sixty patients with mild to moderate hypoxemic respiratory failure (Table 1) were enrolled. Patients requiring imminent mechanical ventilation and patients under orders not to receive mechanical ventilation were excluded. Randomization was with a random-numbers table in spreadsheet software (Excel, Microsoft, Redmond, Washington). Patients were randomized in blocks of 4, to ensure even distribution of sample size between the 2 study arms. Allocation concealment was maintained with opaque, sealed envelopes.
Definition of Mild to Moderate Hypoxemic Respiratory Failure
We recorded demographic data, Acute Physiology and Chronic Health Evaluation II score, Sequential Organ Failure Assessment score, arterial blood gas values, SpO2, respiratory rate, and heart rate at baseline, 30 min, 1 hour, 2 hours, and 4 hours after randomization, and then as per unit protocol.
Participants were randomly allocated to receive humidified high-flow oxygen via either NHF (Optiflow, with MR880 humidifier, RT241 heated delivery tube, RT033 large/RT034 small, wide-bore nasal cannula, Fisher & Paykel Healthcare, Auckland, New Zealand) (Fig. 1) or HFFM (standard face mask, MR850 humidifier, RT308 heated delivery tube and air entrainer, Fisher & Paykel Healthcare, Auckland, New Zealand) with an aerosol mask (Hudson RCI, TFX Medical, High Wycombe, United Kingdom) (Fig. 2). The NHF group commenced therapy at an initial flow of 35 L/min. Flow and FIO2 were titrated to an arterial oxygen saturation (SpO2 or arterial saturation via blood gas analysis [SaO2]) of ≥ 95%. The HFFM group received humidified oxygen at 31°C and 32 mg H2O/L, also titrated to an SpO2 or SaO2 ≥ 95%.
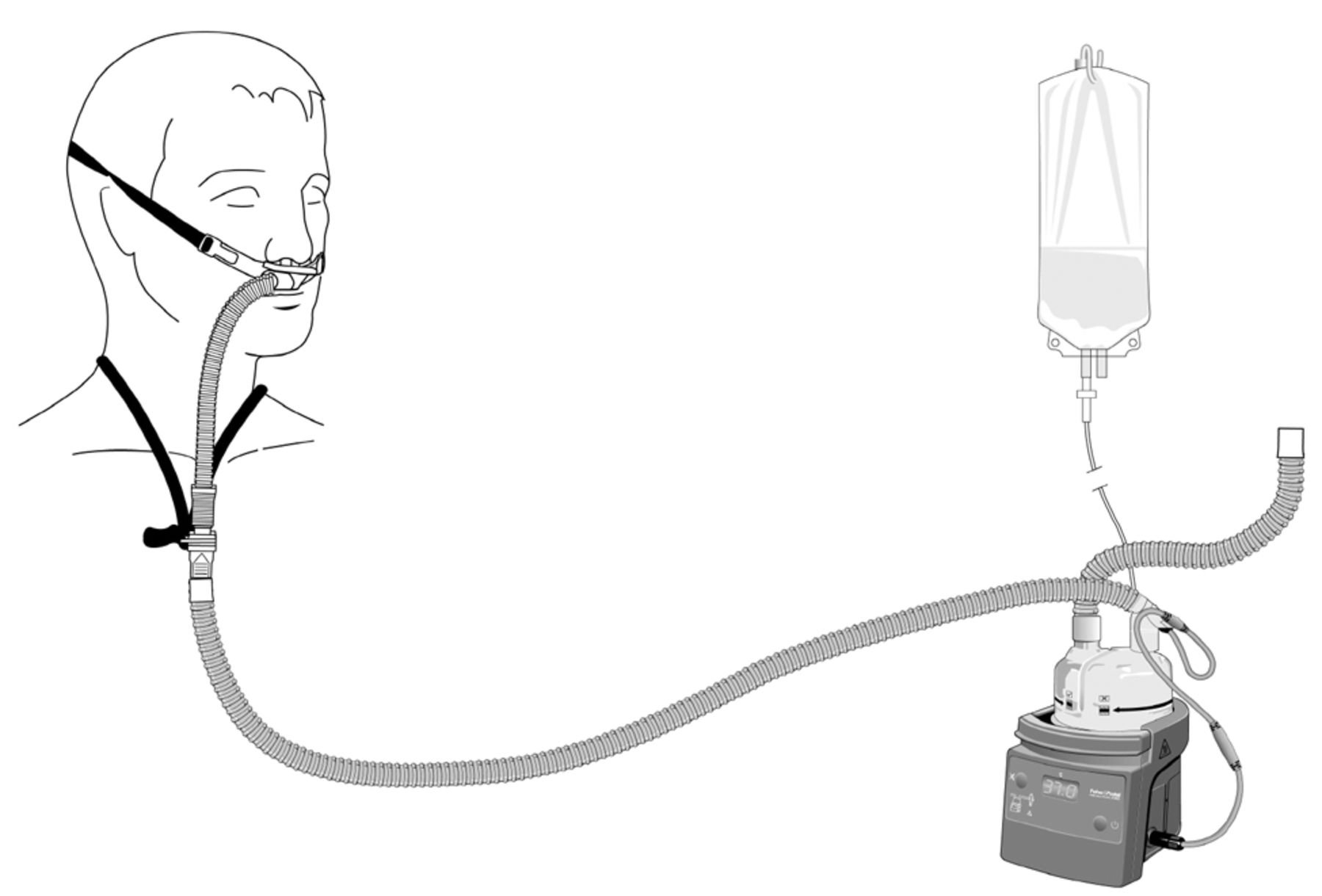
Optiflow high-flow nasal oxygen system.

Standard high-flow face-mask oxygen system.
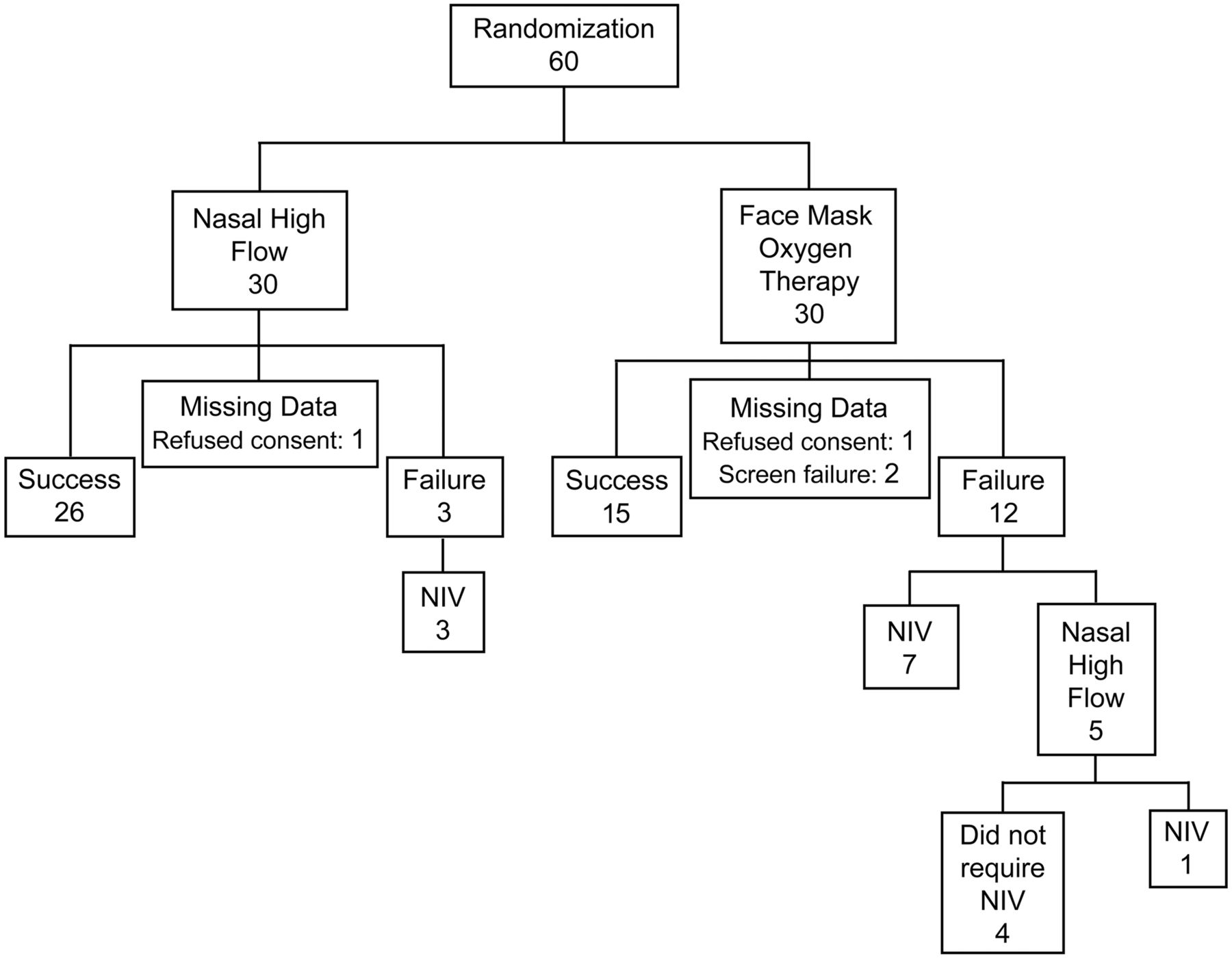
We calculated NIV rate, PaO2/FIO2, SpO2, and stay. Continuous SpO2 data and instances of desaturation (SpO2 < 93% for more than 5 s) were collected with the BedMasterEx software (version 2.02, Excel Medical Electronics, Jupiter, Florida). We graphed the saturation data and highlighted the desaturation episodes. All episodes were identified by time point and cross referenced to screen shots of the SpO2 trace. Episodes were discounted if the SpO2 trace indicated signal interference or signal loss. Allocated therapy was considered successful if the patients were maintained on or weaned from their assigned oxygen therapy within 24 hours of enrollment. Failure of therapy was defined as worsening respiratory failure that required a change in the respiratory-support device within 24 hours of study enrollment. For example, patients on HFFM requiring more respiratory support would be deemed to have failed at the point they were escalated to NIV. Worsening respiratory failure was determined by the treating clinician, based on evidence of one or more of: increased dyspnea, respiratory fatigue, worsening gas exchange, or intolerance of allocated therapy. Patients who failed their allocated therapy were then treated at the discretion of the treating clinician (Fig. 3).
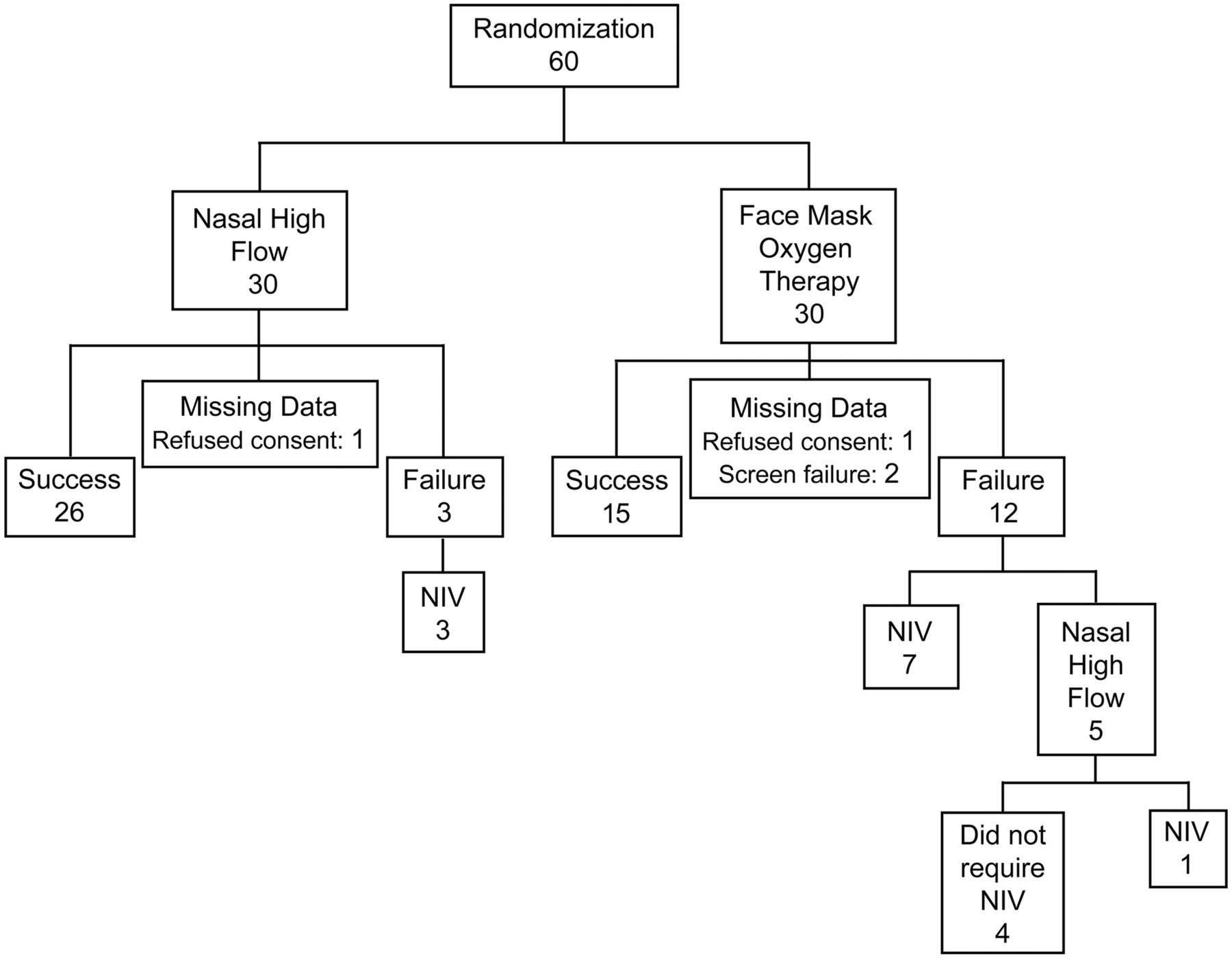
Consort diagram of patient flow through study.
Statistical analysis was carried out with statistics software (SAS 9.1, SAS Institute, Cary, North Carolina, and Excel, Microsoft, Redmond, Washington). PaO2/FIO2 was calculated for the 4-hour period by simple averaging, excluding baseline data because there was no evidence of time trend, and compared with analysis of covariance adjusted for baseline. Additional regression analysis of PaO2/FIO2 was also conducted to account for age, sex, diagnosis, Acute Physiology and Chronic Health Evaluation II score, and Sequential Organ Failure Assessment score. We used Fisher's exact test to compare differences in therapy success, number of patients who needed NIV, and number of patients with oxygen desaturations. Differences in desaturations rate were tested assuming Poisson data. We used analysis of variance to analyze treatment differences in time from randomization to ICU discharge and hospital stay, and the log rank statistic to analyze survival. P values ≤ .05 were considered statistically significant.
Results
Sixty patients were enrolled, and data from 56 were analyzed. Four patients (one from the NHF group, and 3 from the HFFM group) were excluded: 2 refused consent for all data collection, and 2 failed the screening (see Fig. 3). Baseline demographics were similar (Table 2).
Demographics and Baseline Measurements (n = 56)
More NHF patients (26/29) than HFFM patients (15/27) succeeded on their allocated therapy (P = .006). Of the 12 patients in the HFFM group who failed allocated therapy, 7 received NIV, and 5 were switched to NHF, one of whom subsequently required NIV. The 3 patients in the NHF group who failed allocated therapy were all treated with NIV, and none of them were switched to HFFM.
The rate of NIV in the NHF group was 3/29 (10%), compared with 8/27 (30%) in the HFFM group (P = .10) (see Fig. 3).
Where continuous saturation data were successfully recorded, the NHF group had significantly fewer desaturations (P = .009). Seventy-one percent (10/14) of the HFFM group had at least one desaturation, compared to 42% (8/19) of the NHF group (P = .16) (Table 3). Baseline SpO2 was similar.
Desaturation Data
We analyzed PaO2/FIO2 of patients who had complete data available for the first 4 hours (28 NHF, 22 HFFM). PaO2/FIO2 did not differ significantly between the groups (P = .08). However, an additional regression analysis with adjustment for other covariates showed a treatment effect in favor of NHF (P = .03).
Neither time from randomization to ICU discharge nor hospital stay differed significantly (P = .20 and P = .11, respectively, via analysis of variance; note that the survival analysis gave very similar results). Of the other measured variables (arterial blood gas values, respiratory rate, heart rate, and SpO2) only average pH over 4 hours showed an effect, and only when adjusted for the covariates described above (P = .04).
Discussion
There are many options for delivering oxygen therapy to patients with hypoxemic respiratory failure. Clinicians are tasked with selecting the most appropriate device to meet the individual patient's requirements. This study aids the clinician by adding to the limited body of evidence about high-flow oxygen devices used in the critical-care environment.
This study indicates that NHF may be more effective than HFFM for the treatment of mild to moderate hypoxemic respiratory failure. Prior to this study, Optiflow NHF had been available in our ICU for 6 months, during which time our clinicians reported an increase in the use of NHF and an associated reduction in need for NIV. This study was undertaken to quantitatively assess that trend.
We found a significant difference in therapy success between the NHF and HFFM groups. We believe that this is because patients tolerated NHF better. The limited available clinical literature identifies patient acceptability (comfort and tolerance) while maintaining oxygenation as key features of NHF that are likely to improve overall treatment effectiveness.12–16 Studies that compared face masks and nasal masks to nasopharyngeal oxygen delivery devices found that patients described the latter as more comfortable and more effective.13,17,18 Face mask may cause discomfort, induce claustrophobia, and impede oral intake and communication.19 Nasal mask requires patent nasal passages and mouth closure to minimize leak, and can cause pressure sores and tissue necrosis over the nasal bridge.20 Collectively, these problems may cause poor adherence to therapy17 and increased nursing time. In our ICU we heat and humidify oxygen delivered via HFFM. It is possible that the treatment effect would have been greater if the HFFM group had received oxygen that was not heated and humidified. Chanques et al found fewer dryness symptoms in patients using HFFM with a heated humidifier than in those using a bubble humidifier.5
NHF provides body-temperature-and-pressure-saturated gas (37°C, 44 mg H2O/L), which is important for patient comfort16 and improves mucociliary clearance.21 Long-term humidity therapy with NHF in patients with chronic respiratory disease improved lung function and reduced exacerbation days.22 Rea and colleagues proposed that these improved clinical outcomes may be the result of enhanced lung mucociliary clearance.22 Improved secretion clearance might also be a possible mechanism of action in the acute-care environment.
A difference in NIV rates between the 2 groups was found in this study; however, it should be recognized that this study was not powered adequately to detect this treatment effect. When designing this preliminary study, there were no data available to carry out a sample-size calculation. A sample size of 60 patients was deemed feasible and pragmatic for this study.
There is evidence that high gas flow directly into the nares generates positive airway pressure,9–11 which may improve gas exchange and reduce respiratory effort. Nasopharyngeal positive pressure may reduce nasopharyngeal resistance during inspiration and provide expiratory resistance, which appears to be transmitted down the airways, leading to improved lung volumes.23 Another possible explanation for clinical benefit is washout of anatomical dead space.15,24,25 High incoming gas flow may flush expired CO2-rich gas from the upper airways in exchange for oxygen-enriched gas available for the patient's next breath, simultaneously reducing rebreathing of CO2 and increasing the effective FIO2. Sim and colleagues assessed inspired FIO2 with NHF during simulated respiratory failure.8 The FIO2 achieved with 100% oxygen via NHF at 40 L/min was unaffected by simulated respiratory failure. This may well be explained by high incoming gas flow minimizing the variability of room-air entrainment as the respiratory pattern changes.
During the study period clinicians began to see NHF as a preferred option for patients with hypoxemic respiratory failure. This explains the 5 patients who were switched from their allocated HFFM to NHF during the course of the study. We presume that those patients would have been commenced on NIV had NHF not been available. However, in the context of this pragmatic study, the treating clinician was allowed to select any therapy if the randomized treatment failed. We deemed it unethical to withhold NHF if HFFM failed.
It was not practical to blind participants and staff to the allocated therapy—a problem inherent to many studies of medical devices and oxygen therapy systems. This problem was mitigated by randomization techniques and the groups being comparable at baseline. A limitation of this study was the absence of documented guidelines or protocols for escalating respiratory support therapy. When assessing respiratory function in the failing patient, staff reported using clinical judgment and indicators such as SpO2, respiratory rate, and work of breathing in preference to arterial blood gas measurements. Stated criteria for escalating therapy varied and included subjective decision making a large proportion of the time.
These were interesting and unexpected findings of this study and highlight the need for more informative study guidelines to minimize bias when performing research in the real world of intensive care medicine. Although a difference was found in the number of desaturation episodes between the 2 groups, a major limitation of this study was the availability of data for analysis. The limited amount of data available was directly attributable to problems with the software used to download data after hours when research staff were not in attendance. This has highlighted considerations for future studies that require continuous data from bedside monitoring systems. This represents a failure in the execution of the study methodology and highlights some of the challenges when conducting research in the real world. Because of the lack of detailed data available we were unable to complete a comprehensive analysis to determine the degree of desaturation and treatment required for each episode.
Despite the limitations of this study, NHF appears to be a promising new area of respiratory care that warrants further investigation in large, well designed clinical trials.
Conclusions
NHF has a growing place in the repertoire of respiratory therapies available in the intensive care environment. In this study NHF was more successful than HFFM in the treatment of mild to moderate hypoxemic respiratory failure. We hypothesize that the difference in NIV rate found in this study is attributable to positive pressure delivered by the Optiflow system. The results and lessons learned from this preliminary randomized controlled trial will inform the development of an appropriately powered study into the effect of NHF on respiratory therapy outcomes.
Footnotes
- Correspondence: Rachael L Parke, MHSc, Cardiothoracic and Vascular Intensive Care Unit, Auckland City Hospital, Private Bag 92024, Auckland 1010, New Zealand. E-mail: rparke{at}adhb.govt.nz.
-
The authors have disclosed a relationship with Fisher & Paykel, which provides funding to the Auckland District Health Board for the salary of the research nurse in the Cardiothoracic and Vascular Intensive Care Unit, Auckland City Hospital, Auckland, New Zealand.
-
Rachael L Parke MHSc presented a version of this paper at the 53rd International Respiratory Congress of the American Association for Respiratory Care, held December 1-4, 2007, in Orlando, Florida.
-
See the Related Editorial on Page 355
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}