

Abstract
A 45-year-old female was admitted to our ICU with severe ascites, and septic shock due to an obstructive ureteric stone. Despite an FIO2 of 1.0, high PEEP, and multiple recruitment maneuvers, it was challenging to obtain an SpO2 > 85% after the patient was turned. We inserted an esophageal balloon to determine whether the abdominal pressure was affecting lung compliance. PEEP was guided to a level of 32 cm H2O to achieve a transpulmonary pressure of 0 cm H2O. Within 6 hours there was significant oxygenation improvement: PaO2/FIO2 increased from 80 mm Hg to 244 mm Hg, and oxygenation index decreased from 35 to 18. At 48 hours, PaO2/FIO2 was 382 mm Hg and oxygenation index was 7. Paracentesis of approximately 5 L assisted with weaning. Subsequent PEEP changes were guided by transpulmonary pressure. She was weaned from mechanical ventilation within 10 days, with no adverse sequelae associated with very high PEEP.
- PEEP
- esophageal balloon
- transpulmonary pressure
- acute respiratory distress syndrome
- ARDS
- acute lung injury
- ALI
- ascites
Introduction
The current approach to mechanical ventilation of patients with acute lung injury or acute respiratory distress syndrome (ARDS) is to use low tidal volume (approximately 6 mL/kg predicted body weight) and to limit plateau pressure to ≤ 30 cm H2O.1 Another key ventilation setting for these patients is PEEP. Three large randomized controlled trials that compared low PEEP to high PEEP found no definitive difference in clinical outcomes such as mortality.2–4 Brower and colleagues2 and Meade and colleagues3 used PEEP settings determined from a chart that guided PEEP and FIO2 increase or decrease, based on the patient's oxygenation status. Mercat and colleagues set PEEP to reach a plateau pressure of 28–30 cm H2O.4 Even with arbitrary setting of high or low PEEP, a recent meta-analysis suggested a 4% mortality benefit from high PEEP alone with ARDS patients.5 Smaller studies have set PEEP according to lung mechanics and found improved and sustained oxygenation, but the studies were not large enough to identify an improvement in clinical outcomes.6–8 In a recent randomized controlled trial, patients were allocated to receive mechanical ventilation either according to the ARDS Network protocol or guided by pleural pressure measured with esophageal balloon manometry. Transpulmonary pressure (Ptp) was titrated for a target of ≥ 0 cm H2O. Oxygenation and lung compliance were greater in the esophageal-balloon group.9
A key limitation of mechanical ventilators is that they do not measure the Ptp or pleural pressure. Airway pressure alone cannot distinguish poor lung compliance from poor chest-wall compliance. High intra-abdominal pressure can severely impair chest wall mechanics.9,10 We used esophageal balloon manometry to estimate Ptp and guide optimal PEEP in a patient suspected of having decreased lung compliance due to intra-abdominal hypertension.
Case Report
A 45-year-old female with a normal body mass index (22.5 kg/m2) presented to the emergency room febrile, hypotensive, and complaining of left flank pain. She had a history of Crohn disease and ureteral reflux. She was taking no medications at home. A computed tomogram showed a 6–7-mm renal stone in the left pelvic uteric junction, with hydronephrosis and multiple calculi in the left kidney. She went to the operating room for a planned cystoscopy. The stone could not be removed, so a ureteric stent was placed, and she was sent to the intensive care unit (ICU) for septic shock management.
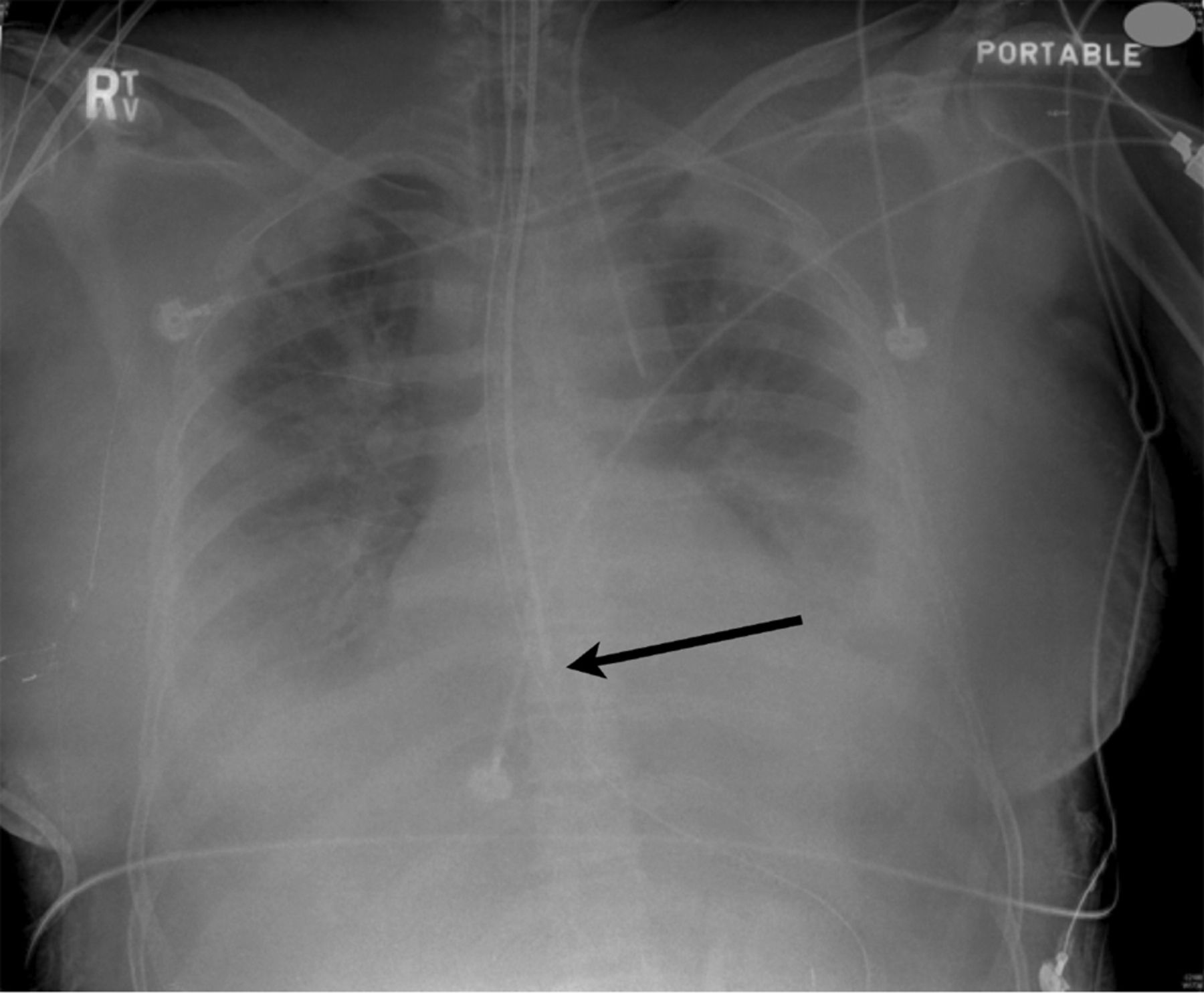
On admission to the ICU she had received 5,000 mL of crystalloid in the operating room, and continued to require fluid resuscitation and norepinephrine infusion for hypotension. Initial ventilation settings were pressure control (above PEEP) of 20 cm H2O to achieve a tidal volume of 6 mL/kg, respiratory rate 26 breaths/min, inspiratory time 1.0 s, PEEP 12 cm H2O, and FIO2 1.0. The initial arterial blood analysis showed pH 7.19, PaCO2 29 mm Hg, PaO2 123 mm Hg, HCO3 10 mEq/L (indicating metabolic acidosis), SaO2 97%, PaO2/FIO2 123 mm Hg, and oxygenation index 17. The initial chest radiograph showed severe interstitial and air-space pulmonary edema (Fig. 1). Her abdomen was firm and her bladder pressure was 29 mm Hg.

Radiograph immediately after insertion of the esophageal balloon (arrow).
During her initial 36 hours in the ICU she required several recruitment maneuvers and subsequent PEEP increases to maintain or improve oxygenation. The recruitment maneuver was a sustained inflation at 40 cm H2O for 40 seconds. During one recruitment maneuver she had a brief hypotensive response, and the recruitment maneuver was discontinued. On her second ICU day she was turned on her side for routine care and SpO2 fell to 78%. SpO2 then slowly increased to 85%, where it stayed for approximately one hour, during which 2 more recruitment maneuvers were attempted, but with no SpO2 response, and a final PEEP increase, from 22 cm H2O to 24 cm H2O.
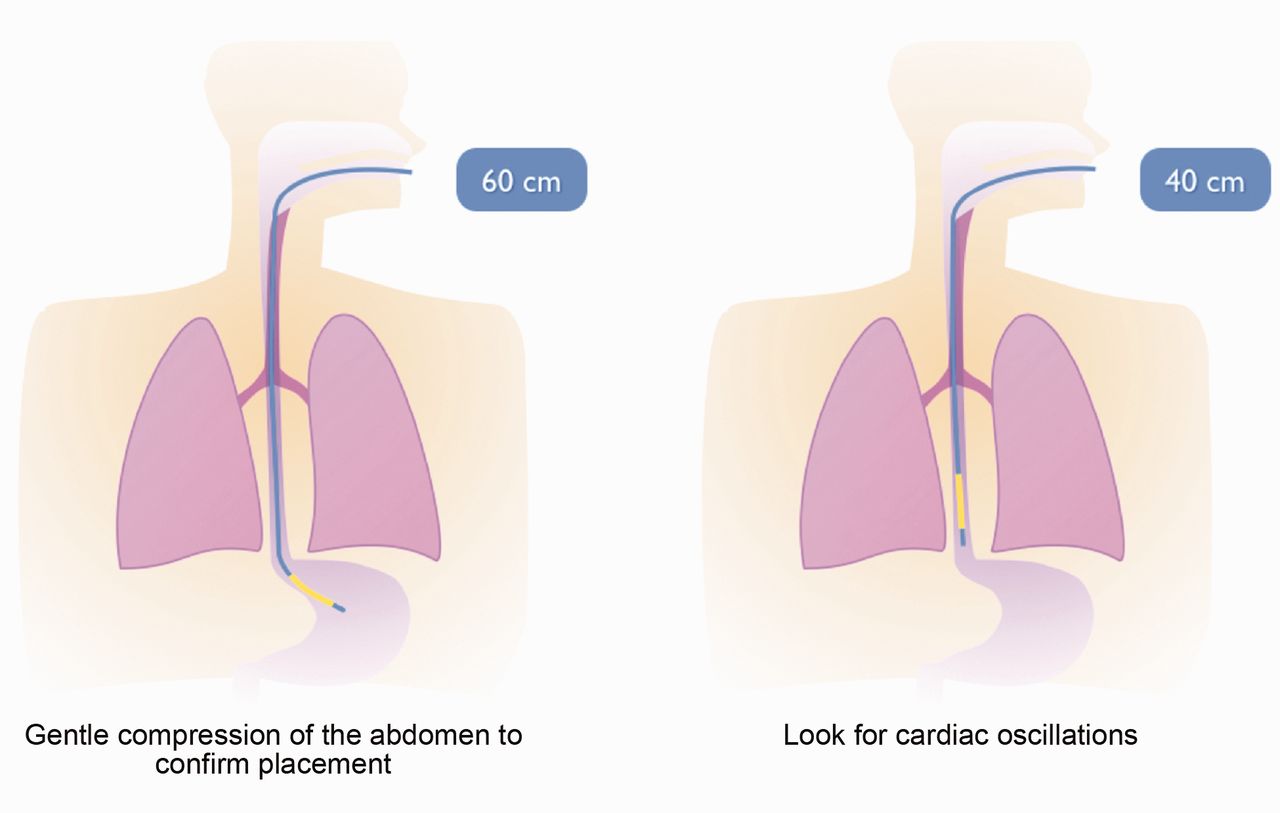
We inserted an esophageal balloon, using a technique previously described (Fig. 2).9 We monitored the esophageal pressure and Ptp with the ventilator (Avea, CareFusion, San Diego, California), which has integrated esophageal monitoring technology (Bicore Monitoring Systems, Irvine, California). An end-expiratory hold was done on the ventilator to assess Ptp (Ptp = airway pressure – pleural pressure measured via esophageal balloon). The Ptp at end-exhalation was –8 cm H2O, which implied that the PEEP necessary to prevent atelectasis was 32 cm H2O. Prior to increasing the PEEP, we drew an arterial blood sample (PaO2/FIO2 80 mm Hg, oxygenation index 35), and performed another recruitment maneuver, but with pressure control and a peak inspiratory pressure of 50 cm H2O. During the recruitment maneuver, SpO2 increased from 85% to 92%. After the recruitment maneuver we set PEEP at 32 cm H2O. An end-expiratory hold confirmed a Ptp of 0 cm H2O, which was our goal. We did not consider using a positive Ptp at this time, because PEEP of 32 cm H2O was higher than we usually use in our ICU.

The esophageal balloon catheter is advanced to approximately 60 cm, so the catheter tip is in the stomach, confirmed by gently compressing the abdomen, which increases the pressure reading on the manometer. The catheter is then withdrawn to approximately 40 cm while watching for pressure change and visualizing cardiac oscillations.
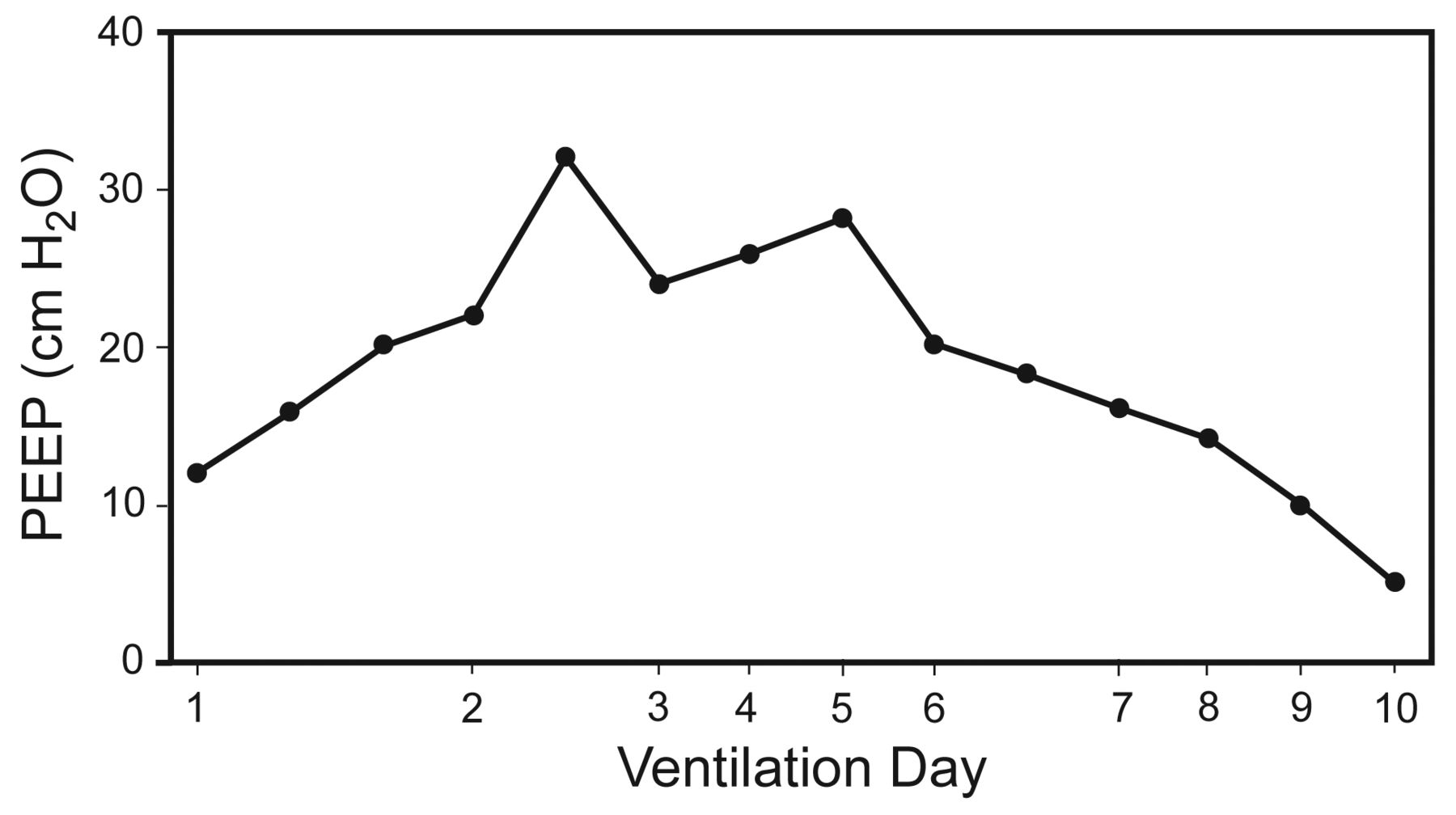
Arterial blood analysis showed a gradual increase in oxygenation, and FIO2 was titrated accordingly, leaving the PEEP at 32 cm H2O to maintain a Ptp of 0 cm H2O. Six hours after setting the PEEP at 32 cm H2O, PaO2/FIO2 was 244 mm Hg and oxygenation index was 18. The following day, bladder pressure had increased to 36 mm Hg. PEEP was still at 32 cm H2O, PaO2/FIO2 was 301 mm Hg, and oxygenation index was 13. We inserted an intraperitoneal pigtail catheter in the right lower quadrant and drained 2 L of clear yellow ascitic fluid. During the initial fluid drainage we clearly observed a rise in the Ptp waveform, indicating that she was now receiving “excessive” PEEP. After the initial drainage, end-expiratory maneuvers were done, and, guided by Ptp, PEEP was weaned down to 24 cm H2O. She continued to drain > 1 L per day from her abdomen for the next 2 days. 48 hours after esophageal balloon insertion, PaO2/FIO2 was 365 mm Hg and oxygenation index had decreased to 7 (Fig. 3). For the next 3 days the PEEP was guided by the Ptp (Fig. 4). On the sixth esophageal-balloon day (day 8 of mechanical ventilation) we switched to a pressure support mode (pressure support 10 cm H2O, PEEP 14 cm H2O, and FIO2 0.35) and removed the esophageal balloon. We then decreased PEEP by 2 cm H2O approximately every 6–8 hours, as tolerated, and on the tenth day she was extubated with a PaO2/FIO2 of 576 mm Hg. Fig. 5 shows the PEEP changes. There were no episodes of barotrauma (eg, pneumothorax) or hypotension associated with the high PEEP. She was discharged to the ward and eventually home.

PaO2/FIO2 and oxygenation index after insertion of the esophageal balloon.

Screen shot from the Avea ventilator, showing an expiratory-hold maneuver. The screen can be frozen and the cursor can be dragged over the area to display the transpulmonary pressure (Ptp) PEEP (A). The average Ptp PEEP can also be displayed on the side panel (B).

PEEP during the patient's intensive care stay.
This patient's course renewed our interest in measuring esophageal pressure to guide PEEP. The PEEP was much higher than expected, and helped us to liberate the patient from mechanical ventilation sooner than expected.
Discussion
This patient was the first in whom we used an esophageal balloon with such dramatic effect. The esophageal balloon was easily inserted. We did not compensate for body positioning during measurements. We also did not precisely follow the Ptp/FIO2 chart used by Talmor et al.9 If we had used the chart, and compensated for body positioning, we would have needed to set PEEP initially at 37 cm H2O. Weaning the PEEP was strongly influenced by the ascites drainage. In retrospect, it would have been best to have drained the ascites first, but the esophageal balloon helped to underscore the need for drainage, and to guide optimal PEEP. The initial bladder pressure of 29 mm Hg and her clinical presentation were consistent with abdominal compartment syndrome. The further increase in bladder pressure did not continue to affect the esophageal pressures (Fig. 6), which may also be expected with abdominal compartment syndrome once the abdominal pressure no longer causes displacement of the diaphragm.10 For 48 hours after insertion of the abdominal drain, the PEEP required for adequate end-expiratory Ptp was 24–28 cm H2O, which was previously above our PEEP comfort level.
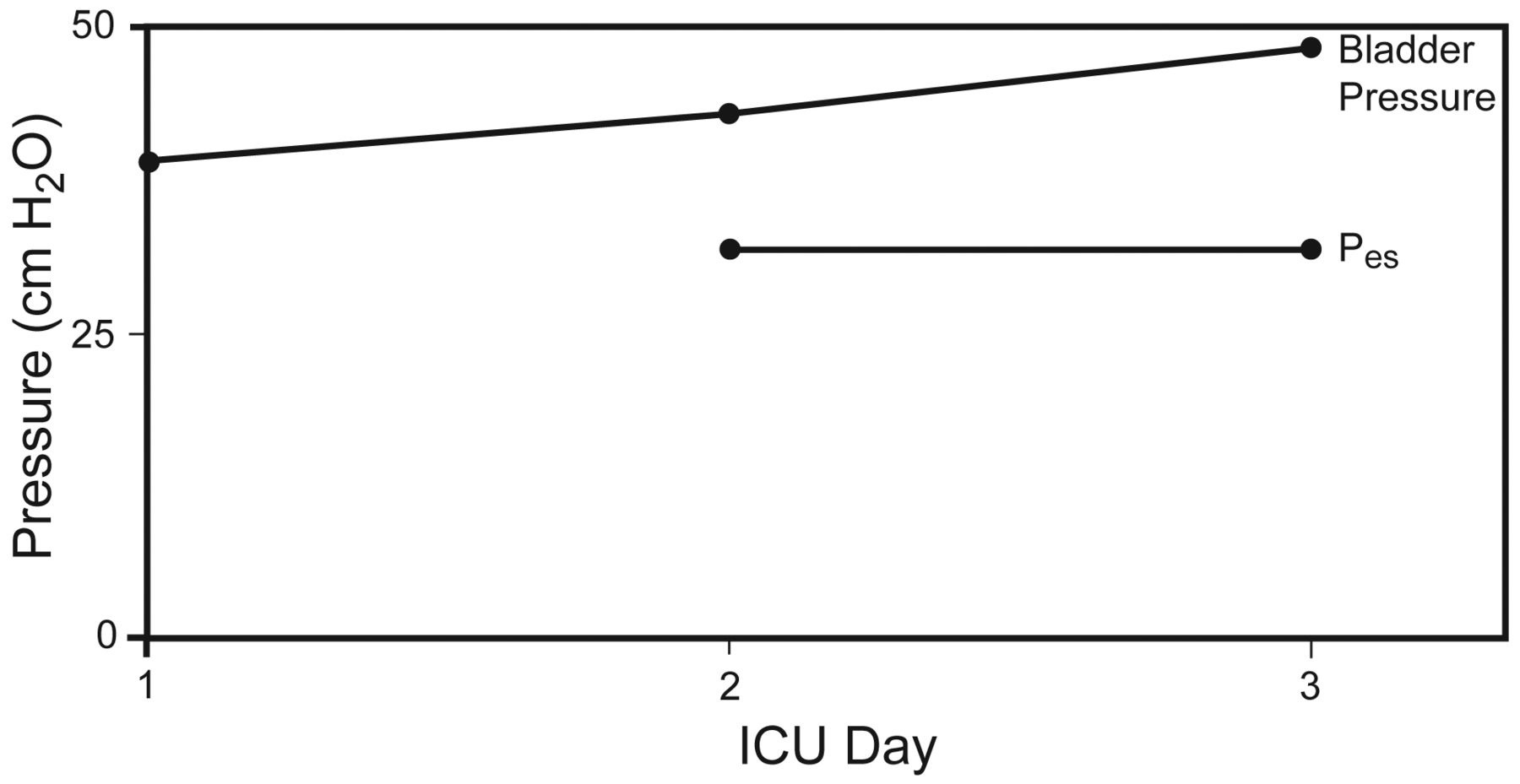
Esophageal pressure (Pes) and bladder pressure in the 3 days prior to inserting the abdominal drain.
Although esophageal pressure is only an estimation of mid-lung pleural pressure and does not necessarily represent the entire ARDS lung, we did perform inspiratory-hold measurements to estimate the Ptp reached during the pressure control breath. With PEEP set according to a Ptp of 0 cm H2O, the inspiratory hold showed that Ptp was consistently ≤ 12 cm H2O, which is well below the 25 cm H2O limit suggested in the trial by Talmor and colleagues.9
There are several considerations before using esophageal balloon manometry to guide PEEP. Talmor and Fessler discussed these concerns in detail in the February 2010 issue of Respiratory Care.11 The concerns include the lack of clinical data for use in patients with ARDS/acute lung injury, and measurement errors. We will discuss 3 concerns: catheter insertion, body positioning, and the ARDS lung.
Catheter Position
Insertion of the catheter can be challenging, depending on which catheter you use, and on operator familiarity. CareFusion offers 2 catheter styles for use with the Avea ventilator: a standard catheter, and a combination esophageal and feeding catheter. The combination catheter is much more rigid and probably easier to insert. The only limitation of the combination catheter is if the objective is to direct the catheter into the duodenum for feeding. For this reason we do not use the combination catheter.
Another brand of esophageal balloon catheter is made by Cooper Surgical (Ackrad Laboratories, Cranford, New Jersey). This vinyl catheter comes with a stylet wire, and can be transduced to a manometer, so Ptp can be calculated. However, this catheter does not work with the Avea ventilator. Catheter placement is typically done by inserting it into the stomach (to approximately 60 cm), and placement is confirmed by gentle compression of the abdomen and observation of a pressure increase on the screen. The catheter is then withdrawn into the esophagus (approximately 40 cm) while watching for pressure change and visualizing cardiac oscillations (see Fig. 2).9,10 The catheter is radiopaque and therefore visible on radiograph. The balloon portion of the catheter should be positioned in the lower third of the esophagus, behind the heart.
Body Position
As determined in studies by Washko,12 the patient's body position can also affect the measurements. The recommended compensation for positional artifact is to add 3 cm H2O to the Ptp ([airway pressure – esophageal pressure] + 3 cm H2O). Others have compensated by +5 cm H2O.10,13
The Heterogeneous ARDS Lung
The catheter is positioned mid-lung, in the lower third of the esophagus. If a patient has a large degree of consolidation (pulmonary ARDS) in the dorsal lung regions, it is difficult to be certain that the measured Ptp is equal throughout the lung. Overdistention may be occurring in areas not affected by consolidation.14
Since our experience with the above-described patient, we have increased our use of esophageal balloon for guiding PEEP in selected patients. We have begun to use bladder pressure as an indicator in patients with suspected or documented intra-abdominal pathology, who may benefit from Ptp-guided PEEP, in addition to lung-protective ventilation.10
Footnotes
- Correspondence: Tom Piraino RRT, Respiratory Therapy Services, St Joseph's Healthcare, 50 Charlton Avenue East, Hamilton ON L8N 4A6. E-mail: tpiraino{at}stjoes.ca.
-
The authors have disclosed no conflicts of interest.
-
Tom Piraino RRT presented a version of this paper at the 55th International Respiratory Congress of the American Association for Respiratory Care, held December 5–8, 2009, in San Antonio, Texas.
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}