

Abstract
BACKGROUND: Studies of ventilation strategies that included higher PEEP in patients with acute lung injury (ALI) or acute respiratory distress syndrome (ARDS) have yielded conflicting results.
OBJECTIVE: To determine whether higher PEEP during volume-limited and pressure-limited ventilation is associated with 28-day mortality or barotrauma rates in patients with ALI/ARDS.
METHODS: We searched MEDLINE, CENTRAL, EMBASE, CINAHL, Web of Science, and the bibliographies of retrieved papers to identify randomized controlled trials that compared higher and lower PEEP in adult patients with ALI/ARDS who were already receiving volume-limited or pressure-limited ventilation. Two of us independently abstracted study-level data, including study design, patient characteristics, study methods, intervention, and main results. We pooled the study-level data with a random-effects model, unless heterogeneity was low (I2 < 50%), in which case we used a fixed-effects model. The primary outcome was 28-day mortality.
RESULTS: Four randomized trials (2,360 participants) were evaluated. Higher PEEP had a nonsignificant trend toward lower 28-day mortality (pooled relative risk 0.90, 95% CI 0.79–1.02). There was no difference in barotrauma between the 2 groups (pooled relative risk 1.17, 95% CI 0.90–1.52). Two studies reported an adjusted hospital death rate, and the pooled results of sensitivity analysis with those adjusted rates were identical to those of the unadjusted analysis.
CONCLUSIONS: In 4 recent studies that used volume-limited or pressure-limited ventilation in ALI/ARDS patients, higher PEEP was not associated with significantly different short-term mortality or barotrauma. This study does not support the routine use of higher PEEP in patients with ALI/ARDS.
- acute respiratory distress syndrome
- adult
- acute lung injury
- mechanical ventilation
- meta-analysis
- mortality
- randomized controlled trial
- review
Introduction
Acute lung injury (ALI) is a syndrome of life-threatening respiratory failure characterized by the acute onset of hypoxemia (PaO2/FIO2 ≤ 300 mm Hg) and bilateral pulmonary infiltrates that are not primarily attributable to left atrial hypertension.1 Acute respiratory distress syndrome (ARDS) is a subset of ALI with more severe hypoxemia (PaO2/FIO2 ≤ 200 mm Hg).1 ALI affects approximately 190,000 patients each year in the United States, and the hospital mortality rate is approximately 39%.2
Mechanical ventilation is essential for survival in most patients with ALI/ARDS. However, mechanical ventilation can also cause ventilator-induced lung injury (VILI), which can delay or prevent recovery from acute respiratory failure.3,4 One cause of VILI is excessive tidal volume and pressure, which can overdistend aerated lung tissue.3–5 In a study by the National Institutes of Health ARDS Network, a mechanical ventilation strategy with lower tidal volume and pressure was associated with a 9% absolute lower short-term mortality in ALI patients, compared to a more traditional strategy that used larger tidal volume.6
Another cause of VILI involves exhalation to a low lung volume and pressure,4,7 which injures small bronchioles and alveoli by repeated opening and closing during tidal ventilation,7 and there may be excessive stress and strain between aerated and atelectatic regions of lung parenchyma.8 The traditional approach to mechanical ventilation involved modest PEEP (5–12 cm H2O) to prevent atelectasis and severe hypoxemia.9–11 However, some investigators recommend higher PEEP, to increase the proportion of aerated lung at end-expiration (ie, maintain alveolar recruitment) and prevent VILI from exhalation to low volume and pressure.7,12 Moreover, higher PEEP may improve arterial oxygenation and allow a lower FIO2, which could reduce pulmonary oxygen toxicity.13 However, these benefits of higher PEEP may be offset by additional lung injury due to overdistention or decreased cardiac output, due to increased intrathoracic pressure and increased pulmonary vascular resistance.14
The potential benefits of higher PEEP in patients with ALI/ARDS already receiving volume-limited or pressure-limited ventilation remain unclear, as existing randomized controlled trials may have been underpowered to find a potentially small but clinically important reduction in short-term mortality.15–18 Two study-level meta-analyses have been performed19,20: one concluded that higher PEEP was beneficial in unselected patients with ALI/ARDS.19 However, that study's methods were suboptimal21 because those researchers pooled adjusted hospital mortality from one of the studies15 but did not include the adjusted hospital mortality data from another trial, in which there were also imbalances in baseline characteristics.16 Our objective was to evaluate the benefits and harms of higher versus lower PEEP in adults with ALI/ARDS receiving volume-limited or pressure-limited ventilation, via meta-analysis of relevant randomized controlled trials that evaluated short-term unadjusted mortality and barotrauma.
Methods
This study was performed at Johns Hopkins University School of Medicine, Baltimore, Maryland, and was conducted and is reported according to the Quality of Reporting of Meta-analyses (QUORUM) guidelines for meta-analyses of randomized controlled trials.22
Data Sources and Search Strategy
We electronically searched the MEDLINE, CENTRAL, EMBASE, CINAHL, and Web of Science databases up to November 15, 2008, to identify potentially relevant publications. Our search strategy included controlled vocabulary and related text words for: ALI/ARDS (study population), use of PEEP (study intervention), and randomized controlled trials (study design). The search strategy employed standard filters for the identification of randomized clinical trials23,24 and included no language restrictions. In addition, we hand-searched conference proceedings (2005 through 2007) from the European Society of Intensive Care Medicine, American Thoracic Society, and the Society of Critical Care Medicine, and the bibliographies of all selected articles and relevant review articles to find additional relevant abstracts and studies.
Study Selection
Eligible studies were randomized trials in which the study groups received volume-limited or pressure-limited ventilation and either higher or lower PEEP in adult patients (age ≥ 18 y) with ALI or ARDS, as defined by, or consistent with, the American-European Consensus Conference criteria.1 We excluded studies that only reported physiologic and/or radiologic outcomes. Two reviewers (ECD and EF) independently screened titles, abstracts, and studies for study eligibility, and disagreements were resolved via consensus. We assessed the reviewers' agreement on study inclusion with the Cohen κ statistic.
Data Extraction
Two reviewers (ECD and EF) independently abstracted data and methods from the included studies, using standardized forms. Abstracted data included study design, patient characteristics, study methods, intervention, and main results. Differences in data abstraction were resolved via consensus. The methodological quality of studies was evaluated according to published guidelines including: description of randomization sequence generation; allocation concealment; assessor blinding; completeness of outcome data; and selective reporting of outcomes, eligibility criteria, therapies, and excluded patients.25 Furthermore, study quality was quantified with the Jadad score.26 Studies were not excluded from the primary meta-analysis on the basis of their quality assessment.
The primary outcome was all-cause mortality at 28 days. Secondary outcomes were mortality in the intensive care unit and hospital, and barotrauma (as defined in each trial).
Statistical Analysis
We report dichotomous outcomes as relative risk (RR) and 95% confidence interval. If mortality at 28 days was not explicitly stated, it was determined from data in the published study.15 Studies with zero total events (ie, in both the higher and lower-PEEP groups) were excluded from the pooled analysis for that outcome.27,28 The I2 statistic was used as a measure of heterogeneity, calculated as the proportion of total variation attributable to the between-study variation, and interpreted with published guidelines: low heterogeneity 25–49%, moderate heterogeneity 50–74%, and high heterogeneity ≥ 75%.29 A priori, we pooled study-level data with a random-effects model,30 unless heterogeneity was low (I2 < 50%), in which case we used a fixed-effects model.31 We assessed for publication bias with funnel plots and the Begg test.32
A nominal P value of < .05 was taken as statistically significant. The analyses were performed with statistics software (Stata 10.0, StataCorp, College Station, Texas).
Results
Search Results and Study Characteristics
The search identified 1,620 citations, and evaluation found 4 eligible studies (Fig. 1).15–18 The 2 reviewers had complete agreement (κ = 1.0) on study inclusion. There was no evidence of significant publication bias for the primary or secondary outcome. The eligible studies were conducted in 5 different countries and enrolled a total of 2,360 (mean 590, range 61–983) adults with ALI/ARDS (Table 1). Three of the studies were multicenter.15–17 All the studies enrolled patients with both ALI and ARDS.

Study selection. ALI = acute lung injury. ARDS = acute respiratory distress syndrome.
Characteristics of the Included Randomized Controlled Trials
The studies used different mechanical ventilation strategies. In the higher-PEEP group, PEEP was set in the following ways: two used tables of fixed combinations of PEEP and FIO2 settings to reach an oxygenation goal range,15,16 and two set PEEP according to physiologic variables: one used the maximum values permitted while maintaining a plateau pressure < 30 cm H2O,17 and the other adjusted PEEP according to end-expiratory transpulmonary pressure (ie, difference between airway-opening pressure and pleural pressure, with pleural pressure estimated from esophageal pressure).18
In the lower-PEEP group, PEEP was set in the following ways: three used fixed combinations of PEEP and FIO2 to reach a target oxygenation goal,15,16,18 and one used the lowest PEEP to target oxygenation and/or hemodynamic goals.17 Plateau pressure on day 1 was greater in the higher-PEEP group (range 27–32 cm H2O) than in the lower-PEEP group (21–25 cm H2O). Primary outcomes differed between the studies: the 28-day mortality range was 22–39% in the lower-PEEP groups, and 17–28% in the higher-PEEP groups (Table 2).
Outcomes of the Included Randomized Controlled Trials
Quality Assessment
Overall, all the studies met most or all of the criteria for methodological quality (Table 3). All the studies met American-European Consensus Conference criteria for the diagnosis of ALI/ARDS,1 and had clearly defined eligibility criteria, therapies, and reasons for patient exclusion. In all the studies the investigators were not masked to treatment allocation after randomization.
Methodological Quality of Included Studies*
Evidence Synthesis
None of the studies found a statistically significant difference in 28-day mortality between the PEEP groups.
Mortality
The pooled analysis found a nonsignificant 28-day mortality trend that favored the higher-PEEP group (27%, n = 1,166 vs 30%, n = 1,194, pooled RR 0.90, 95% CI 0.79–1.02, I2 = 11%) (Fig. 2). Only one study reported intensive care unit mortality, so a pooled analysis for that outcome was not possible.16 Hospital mortality was reported in 3 studies (n = 2,299 patients).15–17 Higher PEEP was not associated with a significant difference in hospital mortality (pooled RR 0.94, 95% CI 0.84–1.05, P = .25, I2 = 0%).15–17

Association of higher PEEP and 28-day mortality. The size of the data marker indicates the weight of the study.
Two studies adjusted for imbalances in baseline characteristics, including age and severity of illness.15,16 In the first study, adjustment for these baseline imbalances led to a nonsignificant trend toward lower in-hospital mortality in the higher-PEEP group (25.1% vs 27.5%, P = .47).15 In the second study, adjustment for these imbalances, when compared to the unadjusted results, increased the RR of in-hospital mortality in the higher-PEEP group, compared to the lower-PEEP group (RR 0.97, 95% CI 0.84–1.12, P = .74).16 When we used the adjusted hospital mortality from these studies in the analysis, the pooled results were identical to the unadjusted analysis (pooled RR 0.94, 95% CI 0.84–1.05, P = .25, I2 = 0%).15–17
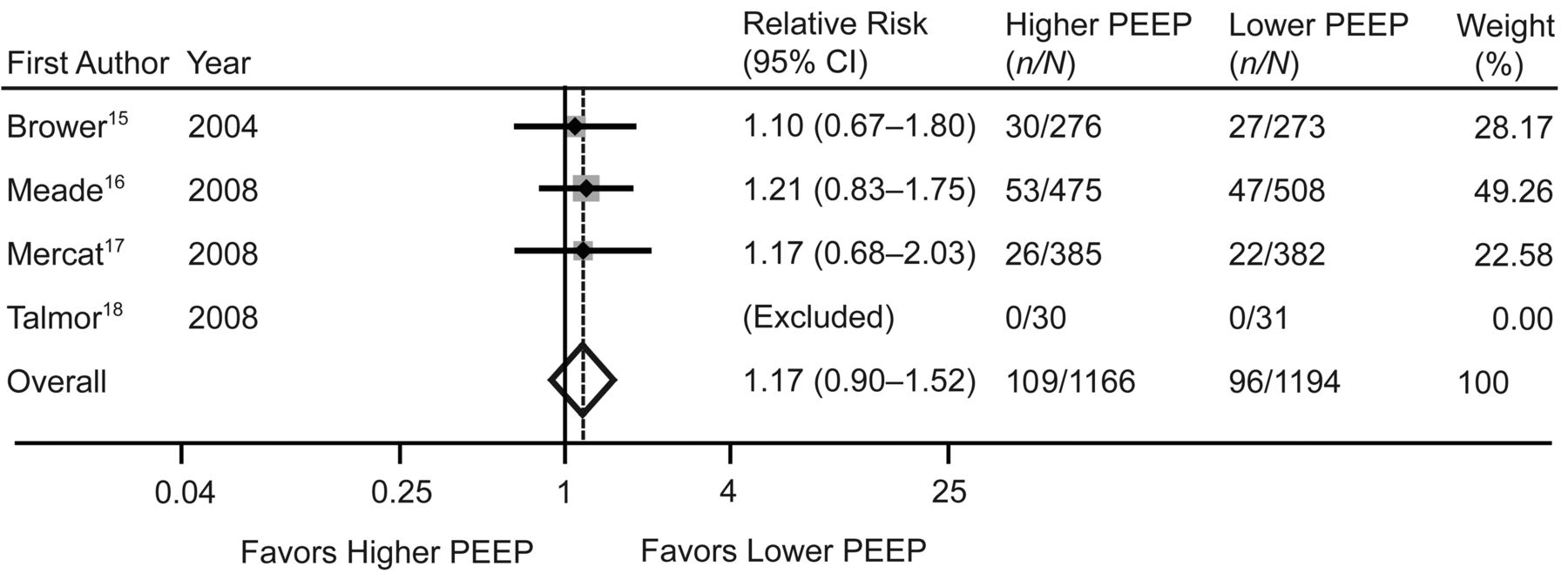
Barotrauma
Barotrauma was reported in all of the studies, but was excluded from the analysis in one study as there were no events in either group.18 Higher PEEP was associated with a nonsignificant increase in barotrauma (pooled RR 1.17, 95% CI 0.90–1.52, P = .25, I2 = 0%) (Fig. 3). These 4 studies included 109 (9%) barotraumas among 1,166 patients in the higher-PEEP group and 96 (8%) barotraumas among 1,194 patients in the lower-PEEP group.

Association of higher PEEP and barotrauma. The size of the data marker indicates the weight of the study.
Discussion
In this meta-analysis of randomized trials of mechanical ventilation strategies in patients with ALI/ARDS receiving volume-limited or pressure-limited ventilation, higher PEEP was not associated with lower short-term mortality or an increased risk of barotrauma.
Our study differs from prior meta-analyses19,20,33 in several ways. First, our study includes the most recently published randomized controlled trial.18 Second, for the primary analysis we pooled unadjusted data. Third, we performed a sensitivity analysis with adjusted data from the 2 studies in which those data were available.15,16 In contrast, 2 prior meta-analyses19,20 pooled adjusted hospital mortality from one study15 (where adjusted mortality favored higher PEEP), but did not include adjusted data from another trial that had imbalances in baseline characteristics16 (adjusted data less favorable to higher PEEP). These 2 meta-analyses consequently reported an effect of higher PEEP on hospital mortality as a pooled odds ratio of 0.86 (95% CI 0.72–1.02)20 and a pooled RR of 0.90 (95% CI 0.81–1.01).19 Despite a nonsignificant trend toward benefit of higher PEEP, one of the 2 meta-analyses concluded that the “current evidence supports the use of high PEEP in unselected groups of patients with ALI/ARDS.”19 Our primary analysis, which pooled unadjusted hospital mortality and reported an RR of 0.94 (95% CI 0.84–1.05), resolves the conflicting conclusions from those 2 prior meta-analyses, as our trend in unadjusted hospital mortality cannot support the conclusion that unselected patients with ALI/ARDS may benefit from higher PEEP.
A recent meta-analysis that used patient-level data evaluated the association between higher PEEP in adults with ALI and hospital mortality34 and reported an adjusted RR of 0.94 (95% CI 0.86–1.04) for hospital mortality with higher PEEP.15–17 This result is very similar to our meta-analysis result and reinforces the accuracy of our study-level meta-analysis, as compared to the other meta-analyses that have used study-level data. Briel and colleagues conclude that unselected patients with ALI/ARDS do not benefit from a higher-PEEP strategy, but the subgroup of patients with severe hypoxemia (ie, ARDS patients) may derive the greatest benefit from a higher PEEP strategy (adjusted RR for hospital mortality 0.90, 95% CI 0.81–1.00), and should be evaluated in future studies to confirm if a mortality benefit is present.34
Experimental models7,35 and observational studies in humans with ALI/ARDS36,37 suggest that higher PEEP can ameliorate VILI, but in the present systematic review we found no significant differences in mortality with higher PEEP in ALI/ARDS patients. A potential explanation for these discrepant results is the heterogeneous patient population captured by the current definition of ALI/ARDS.1 Recent data suggest that there may be distinct subgroups of ALI/ARDS patients with markedly different responses to higher PEEP.38–42 Whole-body computed tomography has demonstrated that higher PEEP in patients with a low percentage of recruitable lung (non-responders) provides little benefit and may be harmful.39 In another study, non-responders (< 150 mL alveolar recruitment) who received a higher PEEP protocol similar to that used in one of the studies in our systematic review15 experienced no change in arterial oxygenation, but did experience significant increases in static lung elastance.40 Therefore, ALI/ARDS patients with predominantly recruitable lung may benefit from a higher PEEP strategy, whereas those with predominantly non-recruitable lung may not benefit and may be at greater risk of VILI from overdistention.43 While none of the trials included in our study screened for recruitability at enrollment or during the treatment course, identification of PEEP responders may be useful for selecting a subgroup of ALI/ARDS patients who might benefit from higher PEEP.39,44,45
Two studies reported important differences in patient outcomes with higher PEEP: a significant increase in ventilator-free and organ-failure-free days, and a nonsignificant mortality advantage,17 and a significant improvement in 28-day mortality, after adjustment for baseline Acute Physiology and Chronic Health Evaluation II score (RR 0.46, 95% CI 0.19–1.00, P = .049).18 These 2 studies were similar in that they both used physiologic variables to adjust PEEP. One study increased PEEP until the plateau pressure was between 28 and 30 cm H2O,17 whereas the other used transpulmonary pressure to adjust PEEP.18 These strategies probably delivered greater PEEP to responders and lower PEEP to non-responders.46 In support of this hypothesis, approximately 10% of patients actually had their PEEP lowered from the baseline value when guided by esophageal pressure.18 Importantly, titrating PEEP to oxygenation response (ie, with a table of fixed combinations of PEEP and FIO2)15,16 may not lead to alveolar recruitment, but to overdistention and an increase in VILI in some patients.44 Despite 40 years of research, the optimal level of and best approach for setting PEEP in ALI/ARDS patients remain elusive.46,47
Our study also suggests that there may be an increased risk of barotrauma with higher PEEP in ALI/ARDS patients receiving volume-limited or pressure-limited ventilation. Higher PEEP can increase plateau pressure, which, when greater than 35 cm H2O, is associated with a greater risk of barotrauma.48 The fact that most patients in the 4 included studies did not have plateau pressure higher than 35 cm H2O may explain why there was no significant difference in the risk of barotrauma. Another possibility is that, despite pooling, our study was underpowered to detect a statistically significant difference in the barotrauma rate between the groups. For example, our meta-analysis was powered (assuming a 2-sided alpha of .05 and power of 0.80) to detect a 3.6% absolute difference in barotrauma (11.6% vs 8.0%), but not the 1.3% difference in barotrauma that we identified (9.3% vs 8.0%). Demonstrating statistical significance for the identified 1.3% absolute difference in barotrauma between groups would require 14,878 patients.
Limitations
First, our meta-analysis was underpowered to detect a small, but potentially important, effect of higher PEEP on 28-day mortality. For example, our meta-analysis was powered (assuming a 2-sided alpha of .05 and power of 0.80) to detect a 5.2% absolute difference in 28-day mortality (24.6% vs 29.8%), but not the 3.1% difference that we observed (26.7% vs 29.8%). Demonstrating statistical significance for the observed difference would require 6,566 patients.
Second, many aspects of the intensive care in the studies were not protocolized, with the exception of mechanical ventilation. Since the investigators could not be blinded to the PEEP treatment arm, differential treatment to patient groups could have resulted in important biases.
Third, barotrauma was variably defined and screened for in each trial, which may have been associated with misclassification and detection biases, respectively. Evidence for a detection bias may be suggested, as the incidence of barotrauma was higher than that reported in observational studies of ARDS patients.49
Finally, moderate differences in age, baseline severity of hypoxemia (ie, PaO2/FIO2), illness (ie, Acute Physiology and Chronic Health Evaluation score),50 and specific ventilation strategies may limit the generalizability of our findings to a particular population.
Conclusions
In adult patients with ALI/ARDS receiving volume-limited or pressure-limited ventilation there was no significant association between higher PEEP and short-term mortality or barotrauma. Future studies should investigate the potential benefit of an approach designed to identify patients more likely to respond with recruitment, applying higher PEEP only to patients who are more likely to respond with recruitment, and avoiding it in those less likely to respond. Our study does not support the routine use of higher PEEP in patients with ALI/ARDS already receiving volume-limited or pressure-limited ventilation.
Acknowledgments
For methodological and statistical advice, we thank Steven N Goodman MD MHS PhD, Department of Biostatistics, Elizabeth Colantuoni MSc PhD, Department of Biostatistics, Kay Dickersin PhD, Department of Epidemiology, and Tianjing Li MD, Department of Epidemiology, Johns Hopkins University, Baltimore, Maryland.
Footnotes
- Correspondence: Elliott C Dasenbrook MD MHS, Division of Pulmonary, Critical Care, and Sleep Medicine, Department of Medicine, University Hospitals Case Medical Center, Case Western Reserve University School of Medicine, 11100 Euclid Avenue, Mail Stop WRN 5067, Cleveland OH 44106. E-mail: ecd28{at}case.edu.
-
Dr Dasenbrook was partly supported by Cystic Fibrosis Foundation Clinical Fellowship Research Award DASENB08D0. Dr Brower was partly supported by National Institutes of Health grant P50 HL073994 and contract N01 HR56170. Dr Fan was partly supported by a fellowship award from the Canadian Institutes of Health Research.
-
Dr Dasenbrook presented a version of this paper at the International Conference of the American Thoracic Society, held May 15-20, 2009, in San Diego, California.
-
The authors have disclosed no conflicts of interest.
-
See the Related Editorial on Page 710
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}