

Abstract
OBJECTIVE: To describe survival outcomes with noninvasive ventilation (NIV) for full ventilatory support, and a mechanically assisted cough and oximetry protocol in a series of patients with Duchenne muscular dystrophy.
METHODS: We monitored end-tidal carbon dioxide (PETCO2), SpO2, vital capacity, maximum insufflation capacity, and cough peak flow. Nocturnal NIV was initiated for symptomatic hypoventilation. An oximeter and mechanically assisted cough device were prescribed when the patient's maximum assisted cough peak flow fell below 300 L/min. Patients used up to continuous NIV and mechanically assisted cough to return SpO2 to ≥ 95% during intercurrent respiratory infections or as otherwise needed. We recorded respiratory and cardiac hospitalizations and mortality, and quantified survival by duration of continuous NIV dependence (ie, unable to maintain oxygenation without the ventilator).
RESULTS: With advancing Duchenne muscular dystrophy, 101 nocturnal-only NIV users extended their NIV use throughout the daytime hours and required it continuously for 7.4 ± 6.1 years to 30.1 ± 6.1 years of age, with 56 patients still alive. Twenty-six of the 101 became continuously dependent without requiring hospitalization. Eight tracheostomized users were decannulated to NIV. Thirty-one consecutive unweanable intubated patients were extubated to NIV plus mechanically assisted cough. Of the 67 deaths (including 8 patients who died from heart failure before requiring ventilator use), 34 (52%) were probably cardiac, 14 (21%) were probably respiratory, and 19 (27%) were of unknown or other etiology.
CONCLUSIONS: Continuous NIV along with mechanically assisted cough and oximetry as needed can prolong life and obviate tracheotomy in patients with Duchenne muscular dystrophy. Unweanable patients can be decannulated and extubated to NIV plus mechanically assisted cough.
- Duchenne muscular dystrophy
- mechanical ventilation
- noninvasive ventilation
- cough
- respiratory paralysis
- respiratory therapy
- mechanical insufflation-exsufflation
- vital capacity
- cough flows
Introduction
In patients with Duchenne muscular dystrophy the vital capacity (VC) peaks between 9 and 16 years of age, and then decreases by 5–10% per year until ventilatory support is required for survival.1 Approximately 90% of patients with Duchenne muscular dystrophy who do not use ventilatory support die from pulmonary complications associated with respiratory muscle weakness between 16 and 19 years of age, and uncommonly after age 25.2–6 Ninety percent of episodes of pneumonia and acute respiratory failure (ARF) that require intubation occur during otherwise benign upper-respiratory infection, mainly because of inability to cough effectively.7 If unable to wean from the ventilator, these intubated patients conventionally undergo tracheotomy for ongoing tracheostomy ventilation.
In 2002 we reported that Duchenne muscular dystrophy patients with respiratory infections who used continuous NIV and mechanically assisted cough with oximetry feedback to prevent sustained SpO2 of < 95% avoided over 100 hospitalizations.8 There have also been numerous reports of prolonged survival (zero to up to 39 months) with predominately nocturnal use of low-span bi-level positive airway pressure (inspiratory-expiratory pressure difference < 10 cm H2O), as opposed to single-pressure continuous positive airway pressure; 42 such studies were listed in one paper.9 In addition, 2 other centers have reported on Duchenne muscular dystrophy patients using continuous long-term NIV.10,11 However, in all previous reports, all unweanable intubated patients underwent tracheotomy.12 In Duchenne muscular dystrophy patients with end-stage respiratory muscle failure we studied the effect of continuous full-setting NIV plus as-needed mechanically assisted cough on survival, the need for tracheostomy, and the incidence of death from cardiac, pulmonary, and other causes.
Methods
This research was performed at and approved by the institutional review board of University Hospital, Newark, New Jersey. We considered all referred Duchenne muscular dystrophy patients. We excluded patients who were too young to need NIV and who did not die during follow-up or were lost to follow-up before using mechanical ventilation. Thirty-four of the long-term continuous NIV users were also in a 2002 study, at which time none of the patients were 40 years old.
We monitored, at 4–12-month intervals, PETCO2, SpO2, VC, maximum insufflation capacity, and unassisted and assisted cough peak flow. We required a minimum of 5 data points to determine peak (plateau) VC. Maximum insufflation capacities were measured spirometrically by the patient maximally air stacking consecutively delivered volumes of air delivered via manual resuscitator or volume ventilator.13 Assisted cough peak flows were measured with a peak flow meter as an abdominal thrust was delivered, timed to glottis opening, after the patient had air-stacked as deeply as possible. The patient was also instructed to routinely air stack 10–15 times, 3 times daily. If the glottis was too weak or the patient unable to perform air stacking, he was trained to do deep passive insufflations by using a manual resuscitator while blocking its exhalation or by using the insufflation mode of the insufflator-exsufflator (CoughAssist, Respironics, Murrysville, Pennsylvania) at 40–60 cm H2O, 10–15 times per session, 3 sessions daily. The deep lung volumes were to augment cough flow (and thus prevent atelectasis), maintain pulmonary compliance, and raise voice volume.13,14
Nocturnal NIV was prescribed for symptomatic hypercapnia, the symptoms of which were fatigue, morning headaches, daytime somnolence, decreased appetite, depression, and weight loss. Polysomnography was not used because we treated only symptoms, not asymptomatic central or obstructive apneas. When symptoms were questionable and diurnal PETCO2 was not elevated, we measured nocturnal SpO2 and PETCO2, as recommended.15 PETCO2 > 50 mm Hg and multiple hourly desaturations to < 95% prompted a trial of NIV. If the patient did not feel that symptoms were relieved by NIV, we told him that its use could be deferred and that we would reassess in 6 months.
We used portable ventilators on assist/control mode with tidal volume 800–1,500 mL, respiratory rate of 10–12 breaths/min with all patients, to alleviate symptoms, normalize alveolar ventilation, facilitate inspiratory muscle rest, and permit independent air stacking.13 If aerophagia occurred, we used pressure control mode at ≥ 18 cm H2O. Volume-cycling was preferred over pressure-cycling, to permit air stacking on demand.
If discontinuing nasal NIV in the morning caused dyspnea, we extended NIV use into the daytime hours. We used a 15-mm angled mouthpiece for diurnal NIV unless the patient's lips were too weak to grab the mouthpiece, in which case we used nasal prongs for daytime support. If daytime hypoventilation decreased SpO2 to < 95%, we used oximetry to guide the use of daytime NIV to maintain SpO2 ≥ 95%. When this occurred, patients quickly went from using NIV 12–14 hours a day to > 23 hours a day and, eventually, with little ventilator-free breathing ability (ie, upon cessation of ventilator use they developed progressive hypercapnia, oxyhemoglobin desaturation, and distress within minutes). Tracheotomy was always discussed but never agreed to, because the patients were informed that an ARF episode or the need for general anesthesia necessitating translaryngeal intubation could be managed with extubation to NIV and mechanically assisted cough.16–18 The patients were visited monthly by home-care respiratory therapists trained in NIV and mechanically assisted cough and oximetry.
Life was considered prolonged from the point of requiring full-time (> 23 h/d) NIV. We recorded VC at baseline, VC at onset of nocturnal NIV, and at the need for > 23 hours per day of NIV. We also recorded the ability to glossopharyngeal breathe for independence from continuous NIV.19
We instructed patients in mechanically assisted cough and provided an insufflator-exsufflator for home use once the patient's assisted cough peak flow was < 300 L/min.8 Patients used up to continuous NIV and used mechanically assisted cough to maintain or return SpO2 to ≥ 95% during respiratory infection and following extubation or decannulation at pressure ≥ 40 cm H2O. We instructed them to seek medical attention if they had a respiratory infection and could not maintain SpO2 ≥ 95%.8,20
Death was assumed to be of respiratory etiology if associated with a respiratory infection, an increase in airway secretions, or ventilator or interface malfunction prior to death. The etiology of sudden death at home was considered cardiac if there were no concurrent respiratory symptoms, CO2 and SpO2 had been normal at the last monthly evaluation, and left-ventricular ejection fraction was ≤ 20%, or there had been no respiratory symptoms and a history of hospital admission for congestive heart failure. Death was considered of unknown etiology if it occurred during sleep without evidence of ventilator or interface malfunction, recent oxyhemoglobin desaturation, cardiac history, or low left-ventricular ejection fraction.
Those who required intubation were extubated to the NIV plus mechanically assisted cough protocol once they met specific criteria, including SpO2 ≥ 95% on room air.18 Patients who failed ventilator weaning trials or extubations in other centers were transferred to us for extubation without tracheotomy. Patients presenting with tracheostomy tubes were offered decannulation.
Analysis was performed with statistics software (SPSS 8.0, SPSS, Chicago, Illinois).21 We used a nonparametric method (Mann-Whitney U test) because the data had a non-normal distribution. A P value < .05 was considered statistically significant.
Results
Of 126 Duchenne muscular dystrophy ventilator users and 8 others who died from cardiomyopathy (Fig. 1), 3 patients were diagnosed via DNA analysis of brothers with the same condition, 31 via DNA analysis, 64 via absence of dystrophin on muscle biopsy, and 36 via both those methods. The mean age of wheelchair dependence was 9.7 ± 1.2 years, and none of the patients walked beyond age 12 years. The mean plateau VC of the 31 patients with a minimum of 5 data points around the plateau was 2,073 ± 940 mL, which occurred at 13.0 ± 3.1 years of age. Assisted cough peak flow had decreased to < 300 L/min by 16.2 ± 2.3 years of age.
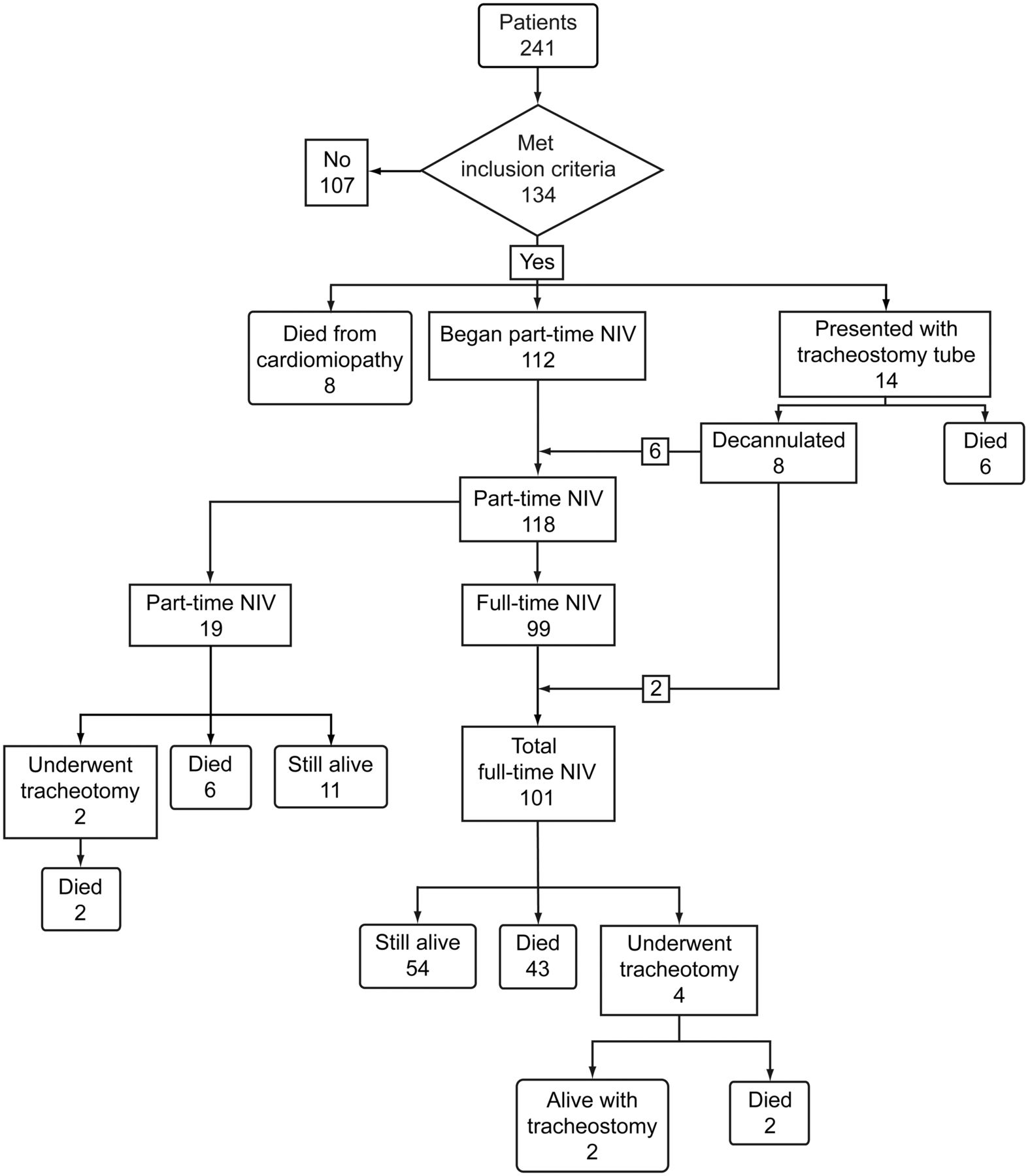
Flow chart. NIV = noninvasive ventilation.
Fourteen patients presented using tracheostomy ventilation. Eight who had no ventilator-free breathing ability since undergoing tracheotomy and had been using tracheostomy ventilation for 5 months to 4 years were decannulated and switched to continuous NIV. Six of those eight then weaned to nocturnal-only NIV within 3 weeks of decannulation. They definitively became continuous NIV users 13 ± 17 months later. All had vital capacities of 120–650 mL at decannulation. Their post-decannulation continuous NIV use data were added to those of the other full-time NIV users. All six of those who did not have their tubes removed died, including five who died from causes related to the tube, after a mean of 12 years of tracheostomy ventilation, including one at age 46 years.
Six out-of-state patients placed on NIV by us were intubated for respiratory-infection-associated ARF and underwent tracheotomy locally after 12, 7, 5, and < 1 year of full-time NIV, or, in 2 patients, part-time NIV. Three of the 6 died from tube-related causes after 12 years, 11 years, and 2 months of tracheostomy ventilation; one died from cerebrovascular disease; and two are still alive. Four of the 6 patients lived beyond age 30.
One-hundred fifteen of the 120 NIV users (including 92 who used full-time NIV) were capable of air stacking (ie, maximum insufflation capacity was greater than their VC) and practiced it daily.13 Air stacking ability indicates sufficient glottic control to protect the airways. Indeed, none of the 120 patients ever aspirated saliva to the extent that baseline SpO2 decreased to < 95%, which is our indication for tracheotomy.22
Their mean diurnal PETCO2 at the start of nocturnal NIV was 44 ± 3 mm Hg. Mean PETCO2 improved to 42 ± 3 mm Hg at the next evaluation. However, diurnal PETCO2 gradually increased to 49 ± 8 mm Hg during the 3.2 ± 2.9 years of part-time NIV, during which their NIV use gradually increased and they were switched to using 15-mm angled mouthpieces when awake. Once NIV became full-time, the PETCO2 of all the users was < 40 mm Hg (mean PETCO2 35 ± 4 mm Hg).
One hundred twenty patients used NIV with access to mechanically assisted cough and oximetry for a mean of 10.5 ± 6.1 years. Table 1 summarizes the data. The patients who died from cardiac failure had significantly lower left-ventricular ejection fraction and more cardiac hospitalizations than the other groups.
Characteristics of 120 Patients with Duchenne Muscular Dystrophy on Noninvasive Ventilation
Twenty-six patients became continuously NIV dependent without being hospitalized or experiencing ARF. Seven continuous NIV users lived to over age 40. The Kaplan-Meier survival curve (Fig. 2) indicates median survival to age 29.5 for 45 patients who are deceased, and to 30.6 for the 56 living patients. The oldest living continuous NIV users were wheelchair-dependent at ages 7, 9, 10, and 11, respectively; at least three of the four have multiple-exon deletions at chromosome Xp21, essentially no dystrophin on muscle biopsy, and have required continuous NIV support for 28, 19, 21, and 24 years, to ages 41, 44, 48, and 47, respectively. Thus, these patients have typical (in the first patient, who was continuously NIV dependent since age 14) to unusually severe Duchenne muscular dystrophy.

Kaplan-Meier survival curve.
The last measured VC of the 101 full-time NIV users was a mean 176 ± 102 mL, or 3% of predicted normal, which is not compatible with survival without continuous ventilator support. Twenty-two patients with mean VC of 224 ± 145 mL and no ventilator-free breathing ability with conventional inspiratory muscles used glossopharyngeal breathing for partially to fully ventilator-free breathing ability during daytime hours.19
All 31 consecutive intubated Duchenne muscular dystrophy patients who failed extubation at other institutions and/or failed ventilator weaning parameters and spontaneous breathing trials were successfully extubated to full-setting NIV and mechanically assisted cough, despite VC as low as 80 mL.
Discussion
Our key findings are:
VC peaked at age 13, then daily air stacking and maximal insufflation therapy was begun
Assisted cough peak flow decreased to < 300 L/min at age 16, then oximetry and mechanically assisted cough were required during respiratory infections
Hypoventilation symptoms appeared at age 19, at a VC of about 640 mL, when nocturnal NIV was begun
Continuous NIV dependence began at 22 years of age, at a VC of about 320 mL
The four most favorable nocturnal NIV studies reported 50% Duchenne muscular dystrophy survival to 25.3–30.4 years.9,23–25 However, since none of the patients required continuous NIV, they clearly had more autonomous breathing ability than our patients with little to no VC. Also, none of those studies noted use of 15-mm angled mouthpiece, eliminated tracheostomy via extubation/decannulation for unweanable patients, or used lung recruitment and mechanically assisted cough. Those and many early studies were generally confined to the use of bi-level positive airway pressure at unspecified settings or settings inadequate to sustain a patient with little or no VC and insufficient to augment cough peak flow sufficiently to avert pneumonia and ARF during respiratory infection. Indeed, some reported no prolongation of survival using NIV.26,27
Three other centers reported the use of long-term continuous NIV in patients with Duchenne muscular dystrophy: 50% of their patients survived to 33, 35, and 39.6 years (41, 43, and 88 patients, respectively).10,28,29 Although Kohler et al did not report the use of daytime mouthpiece NIV or mechanically assisted cough,28 they had reported it in previous papers. Toussaint et al reported daytime NIV provided via 15-mm mouthpiece, plus mechanically assisted cough.10 In both reports, however, unweanable patients intubated for ARF underwent tracheotomy.30 Our survival results are comparable, though we had more than twice as many patients and we extubated and decannulated unweanable patients to NIV, thus prolonging survival with continuous NIV and often permitting resumption of oral intake and temporary recovery of some ventilator-free breathing ability.31 The 2011 study by Ishikawa et al reported that 40% of their Duchenne muscular dystrophy NIV users survived beyond age 40, and routine extubation/decanulation of unweanable Duchenne muscular dystrophy patients, with none of 88 continuously NIV-dependent patients requiring tracheostomy.29 All of their patients resided in a community living center with a cardiopulmonary team specialized in these noninvasive techniques. In addition, their patients benefitted from a cardioprotective medication protocol pioneered by the investigators.32 While none of our local patients underwent tracheostomy, all those who did and most who died from respiratory causes were unable to come to us for emergency care and extubation.
While our patients began to use nasal NIV with mean VC < 700 mL, and continuous NIV at VC < 350 mL, 10 of 15 Duchenne muscular dystrophy part-time NIV users in another study underwent tracheotomy because of progressing disease and hypercarbia not controlled by nocturnal-only NIV, and the others underwent tracheotomy because of bulbar dysfunction, even though their mean VC was 530 mL. They resorted to tracheostomy despite their bulbar-innervated muscle function being comparable to that of our patients, since 18% of both their patients and ours (22 of 120) required gastrostomy tubes. In our patients there was no evidence of saliva aspiration causing a decrease in baseline SpO2, which was our only indication for tracheotomy.22,33
All 8 decannulated patients who lacked ventilator-free breathing ability noted that prior to tracheotomy they had breathed unassisted. Yet, all six of the decannulated patients with VC > 250 mL weaned to part-time NIV. Thus, as described previously for post-polio ventilator users,34 it appears that in Duchenne muscular dystrophy patients ventilator-free breathing ability is facilitated by decannulation to NIV, for various reasons.35
Three centers (one of them ours) reported a 6–9-year survival prolongation in Duchenne muscular dystrophy patients with tracheostomy ventilation, though some patients died because of tracheostomy-tube-associated complications.28,33,36 All the other published studies that have mentioned survival outcomes of tracheostomy ventilation in Duchenne muscular dystrophy were less successful.37–39 While tracheostomy ventilation users can die from accidental disconnection, ventilator failure, trachiectasis, infection, fistula, mucus plugging, or hemorrhage, as our study demonstrates, NIV users can also die from losing access to the noninvasive interface, ventilator failure, or airway congestion. Some new interfaces decrease leak and improve security.40 Overall, however, noninvasive management is associated with fewer respiratory hospitalizations,7 lower costs (by facilitating community care),41 and a 75–100% lower incidence of ventilator-associated pneumonia.42 Patients also prefer NIV over tracheostomy, for speech, safety, convenience, sleep, swallowing, appearance, comfort, and general acceptability.43 None of our 8 decannulated Duchenne muscular dystrophy NIV users ever wanted or needed tracheostomies replaced.
In a recent study that found comparably prolonged survival with continuous NIV or tracheostomy ventilation, morbidity was worse in the tracheostomy group, due to “mucus hypersecretion and tracheal injuries.”44 In another study the 27% of Duchenne muscular dystrophy patients who could glossopharyngeal breathe needed daytime ventilatory support later and used it less than those who could not,19 and had less fear of accidental ventilator disconnection or ventilator failure, even when sleeping, since they could awaken glossopharyngeal breathing to discover that the ventilator no longer functioned.19 Effective glossopharyngeal breathing is not possible with tracheostomy ventilation.
Limitations
Unlike the Ishikawa et al study,29 this study lacked a controlled comparison of invasive versus noninvasive approaches. However, because NIV is now known to be effective, randomization into an invasive-ventilation group would be unethical. Since invasive/tracheostomy outcomes have not been shown to be superior, continuous NIV is the approach of choice, as suggested by many.10,15,45 Another limitation is that we had no autopsy confirmation of the causes of death.
Conclusions
Although most reports of NIV in neuromuscular disease consider only nocturnal NIV,9 recent consensus statements emphasized that NIV can and should be used up to continuously long-term if needed.15,45 The present study is the largest to date demonstrating this, and by extubation/decannulation of unweanable patients to NIV, maintaining it for over 25 years in some patients.
Footnotes
- Correspondence: John R Bach MD, Department of Physical Medicine and Rehabilitation, University Hospital B-239, New Jersey Medical School, 150 Bergen Street, Newark NJ 07103. E-mail: bachjr{at}umdnj.edu.
-
The authors have disclosed no conflicts of interest.
-
See the Related Editorial on Page 878
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}