

Abstract
BACKGROUND: Patients with chronic neuromuscular disease represent less than 10% of those receiving mechanical ventilation in the intensive care unit (ICU). Little has been reported regarding either ICU management of acute respiratory failure (ARF) in the era of noninvasive mechanical ventilation (NIV) or long-term outcomes.
OBJECTIVE: To describe the respiratory management of patients with chronic neuromuscular diseases admitted to our university hospital ICU for ARF, and the long-term outcomes.
METHODS: We retrospectively analyzed patients with chronic neuromuscular diseases admitted to our ICU for a first episode of ARF between January 1, 1996, and February 27, 2007. We assessed severity of illness on ICU admission, respiratory management during ICU stay, and outcomes on June 15, 2008.
RESULTS: During the study period, 87 patients (44 with hereditary and 43 with acquired neuromuscular diseases) had their first ARF episode that required ICU admission. In the hereditary-diseases group and the acquired-diseases group, respectively, the rates of NIV use during the ICU stay were 82% and 63% (P = .040), the intubation rates were 30% and 56% (P = .02), and the tracheotomy rates were 9% and 12% (difference not significant). At the final assessment (median 3 years) the mortality rate was 58%, and mortality was not significantly related to the type of neuromuscular disease. At final assessment, 46% of the patients were on NIV and 29% had tracheotomy.
CONCLUSIONS: In our ICU, chronic neuromuscular disease is an uncommon cause of ARF, for which we often use NIV. These patients had a low probability of death in the ICU. Long-term outcome was independent of the type of neuromuscular disease.
- chronic neuromuscular disease
- amyotrophic lateral sclerosis
- muscular dystrophy
- noninvasive ventilation
- tracheotomy
- acute respiratory failure
- mechanical ventilation
Introduction
Although critical illness neuropathy/myopathy has received much attention in recent years,1 intensive care unit (ICU) weakness can also arise from various hereditary or acquired chronic neuromuscular conditions, such as amyotrophic lateral sclerosis (ALS), myasthenia gravis,2 and these patients are admitted to the ICU for various reasons, including acute respiratory failure (ARF), initiation of noninvasive or invasive mechanical ventilation for long-term ventilatory support, or gastrostomy for enteral nutrition. Though the underlying pathogenic mechanisms, the neuromuscular involvement patterns, and the disease courses differ in the aforementioned diseases, they share common pathophysiological factors. The most important are global hypoventilation due to inspiratory muscle weakness, inability to cough and clear airway secretions (due to expiratory muscle weakness), upper-airway obstruction during sleep (due to pharyngeal muscle weakness), and swallowing impairment and consequent risk of aspiration (due to uncoordinated functioning of the pharynx and the larynx). Ensuring the adequate management of such situations is a subtle and specific process3,4 that includes cough assist, clearing airway secretions,5 noninvasive ventilation (NIV), the appropriate timing of tracheal intubation, and the decision of whether or when to carry out a tracheotomy. These strategies might not be implemented in all ICUs, even though ICU use of NIV has exploded.6 These patients are probably best managed in specialized ICUs that have the appropriate technical and human resources. Our department has been involved for many years in the care management of patients with chronic neuromuscular disease.7 The ICU management of and long-term post-ARF/ICU outcomes in such patients have been rarely reported. We describe the respiratory management and long-term outcomes of patients with the chronic neuromuscular diseases who were admitted to our ICU for ARF. We compare the patients with hereditary versus acquired neuromuscular diseases. Our hypothesis was that the patients with the acquired diseases would have worse outcomes, after controlling for confounding factors.
Methods
Our ethics committee approved this study and waived the informed consent requirement, provided the patients' identities were protected.
Patients
We retrospectively analyzed the records of consecutive patients with chronic neuromuscular disease admitted to our medical ICU between January 1, 1996, and February 28, 2007. We searched our administrative database for all ICU admissions of patients with the following International Classification of Diseases, 10th Revision, codes: G35 ALS or multiple sclerosis; G122 motor neuron disease; G700 myasthenia gravis; G709 neuromuscular dystrophy; G710 Duchene or Becker muscular dystrophy; G711 myotonic dystrophy; G712 congenital muscular dystrophy; G713 mitochondrial muscular dystrophy; G729 myopathy; G825 quadriparesis.
The codes were indexed as a primary or secondary diagnosis or comorbidity during the ICU stay.
Our inclusion criteria were:
Clearly identified muscular dystrophy, ALS, myasthenia gravis, or other acquired neuromuscular disease
Absence of another cause of chronic respiratory failure (COPD, interstitial lung disease, or non-neuromuscular restrictive lung disease)
First admission to our ICU for ARF
ARF was defined as acute breathing discomfort plus any of the following:
Respiratory rate ≥ 25 breaths/min
PaO2 < 60 mm Hg on room air, or PaO2/FIO2 < 300 mm Hg
PaCO2 ≥ 45 mm Hg
pH ≤ 7.36
Need for tracheal intubation
Increase in daily NIV use above the patient's baseline use
We excluded patients who did not have a firm diagnosis of neuromuscular disease and/or who had another cause of chronic respiratory failure or were admitted for a reason other than ARF.
Data Collection
We recorded patient identification number; age; sex; neuromuscular disease; NIV or invasive ventilation (tracheotomy) for long-term home mechanical ventilation prior to ICU stay; cause of ARF; Simplified Acute Physiology II (SAPS II) score8; at-admission arterial blood gas values and respiratory condition at the time of the arterial blood sampling; ICU respiratory management (need for NIV, ventilation mode and duration, need for and duration of tracheal intubation, tracheotomy); status at ICU discharge (dead or alive); and respiratory status/management at ICU discharge (spontaneous breathing, NIV, tracheotomy). Two of us reviewed and classified the admission chest radiographs as normal, pneumothorax, pleural effusion, atelectasis, or infiltrate. The causes of ARF were: alveolar hypoventilation (PaCO2 ≥ 45 mm Hg and pH ≤ 7.36), inability to clear airway secretions, pneumonia, aspiration, left cardiac failure, weaning failure from mechanical ventilation, other, and undetermined.
We followed the patients until June 15, 2008, when we recorded their status (alive or dead) and their respiratory and ventilatory management. This final assessment was by direct patient interview (telephone or consultation) or contact with the patient's general practitioner or other physician in charge of the patient. At the final assessment we also recorded the total number of stays and the corresponding cumulative days in our ICU for additional ARF episodes, in addition to the first ICU stay for ARF.
Our ICU has 5 full-time physiotherapists who cover the ICU 24 hours a day, 7 days a week, and play a key role in managing neuromuscular patients, including:
Clinical assessment of coughing, swallowing capabilities, and airways secretions, several times a day
Support of the respiratory muscles with manual assistance, intermittent positive-pressure breathing, or mechanical insufflation-exsufflation
Involvement in NIV, including selection of the appropriate interface, mode, and settings, and training nurses
Involvement in moving the patients out of bed at the first opportunity
Involvement in weaning from invasive mechanical ventilation, which in our ICU is per a written protocol9 driven by the nurses and physiotherapists10
Involvement in elective extubation when indicated by the physician.
Unfortunately—and this is an important flaw of the present study—we did not enter the daily activities of the physiotherapists in the database.
Data Analysis
The values are presented as median and IQR or mean ± SD. The normal distribution of variables was verified with the Kolmogorov-Smirnov test and by inspecting the Q-Q plots. The comparisons between groups were made with Mann-Whitney U test or analysis of variance and chi-square or the Fisher exact test for continuous and categorical variables, respectively. We grouped the patients according to the neuromuscular disease categories, presence or absence of long-term home NIV before the ICU stay, and the success or failure of NIV during the ICU stay. We grouped the neuromuscular disorders into 2 groups: hereditary and acquired (Table 1). NIV success was defined as use of NIV in the ICU without intubation or tracheotomy. NIV failure was defined as NIV use in the ICU followed by intubation or tracheotomy. Patient survival was estimated from Kaplan Meier plots, and we compared the groups with the Breslow test. The starting point for the survival analysis was the date of entry into our ICU for the first ARF episode. To investigate the effect of covariates on patient survival at the final assessment, we used the Cox proportional hazards model for survival time, with the following covariates: neuromuscular disease group, sex, long-term mechanical ventilation from NIV or tracheotomy before ICU admission, SAPS II, age at the time of ICU admission, and tracheal intubation during the ICU stay. The proportional hazards assumption was verified by plotting the log survival against time for each covariate, then by testing the significance of the interaction between each of them and time to death. The level of statistical significance was set at P < .05. The statistical analysis was carried out with statistics software (SPSS 15.0, SPSS, Chicago, Illinois).
Causes of Neuromuscular Weakness in 87 Patients Admitted to the ICU for Acute Respiratory Failure
Results
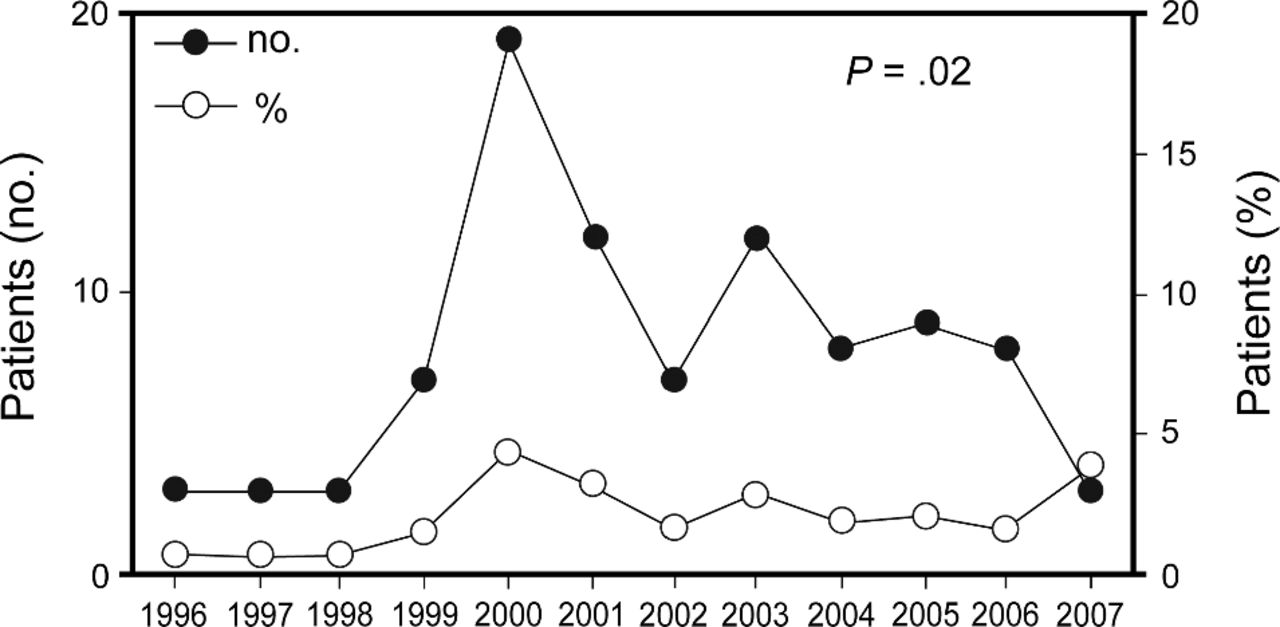
During the study period, 4,813 patients were admitted to our 15-bed medical ICU. Of these we selected 138 patients from the database. We excluded 5 patients who had no clear diagnosis of chronic neuromuscular disease, 16 with no neuromuscular disease, 2 with an associated cause of chronic respiratory failure, 3 whose records were lost, and 25 with chronic neuromuscular disease admitted to our ICU for reasons other than ARF. Those exclusions left 87 patients admitted to our ICU in the study period for a first ARF episode and met the inclusion criteria (see Table 1). The number of admissions of chronic neuromuscular patients with ARF significantly increased during the study period (chi-square for trend = 5.223, P = .02) (Fig. 1), with no significant difference between the neuromuscular diseases (data not shown). One case of dermatomyositis and 3 of ALS were diagnosed during the ICU stay. NIV use for long-term respiratory support prior to ICU admission was significantly different between the hereditary and acquired groups, but this was not the case for tracheotomy (Table 2).

Number and percent of patients with neuromuscular diseases admitted to our intensive care unit during the study period.
Rates of NIV Versus Tracheotomy for Long-Term Ventilatory Support*
Table 3 shows the etiologies of ARF, the distribution of which was not different between the 2 groups. Apart from age, which, as expected, was significantly lower in the hereditary than in the acquired neuromuscular diseases group (Table 4), there were no significant differences between the groups in sex, SAPS II, and arterial blood gas values, or respiratory condition at time of arterial blood sampling and chest radiograph (data not shown).
Etiologies of Acute Respiratory Failure*
Characteristics on ICU Admission
During the ICU stay the rate of use of NIV went up in both groups, as compared to before ICU admission, and was still significantly higher in the hereditary than in the acquired group (see Table 2). The median and IQR numbers of NIV days and NIV hours per ICU day were 6 (3–15) and 12 (8–17), respectively (difference not significant). Volume controlled NIV was most frequently used in the ICU, but the rate was not significantly different between groups (P = .58 via the Fisher exact test) (Fig. 2). During the ICU stay, tracheal intubation was required in 37 patients (43% overall, 30% in the hereditary group, and 56% in the acquired group, P = .02 via the Fisher exact test). The median duration of mechanical ventilation via the tracheal intubation was 10 (5–21) days (difference not significant). The rate of tracheotomy during the ICU stay was also not significantly different between the groups (see Table 2). NIV failed in 11 patients, who were therefore intubated (NIV failure rate 11/63 = 18%). This NIV failure rate was similar across the neuromuscular diseases (P = .99 via the Fisher exact test). Of the 11 NIV-failure patients, 2 died (18% mortality rate) and 4 underwent tracheotomy (36% tracheotomy rate). Among the 15 patients who received NIV after intubation, 2 died (13%) and one underwent tracheotomy (7%). These latter proportions were not significantly different in the NIV-failure patients. Of the 37 patients who were intubated, 23 (61%) were extubated, a proportion which was not significantly different between the groups (P = .49 via the Fisher exact test). Two of them eventually died during the ICU stay and none of them were tracheotomized. Of the 14 patients who could not be extubated, 5 died during the ICU stay and 9 were tracheotomized. After excluding the 10 patients tracheotomized before the ICU stay, the outcomes of the 31 patients from both the groups who received NIV before ICU admission was the same as for the 46 who did not (Table 5).

Use of volume controlled versus pressure support or bi-level positive airway pressure (BiPAP) noninvasive ventilation in patients with hereditary versus acquired neuromuscular disorders during intensive care unit stay.
ICU Ventilation Events and Variables in Patients Who Did Versus Did Not Use Home NIV Before the ICU Stay
Eleven patients died during the first ICU stay (mortality rate 13%) and there was no significant difference between the groups: 5 (11%) in the hereditary group versus 6 (14%) in the acquired group (P = .76 via the Fisher exact test). Except for significantly lower SAPS II (median 22 [18–29] vs 37 [27–57] P < .001 via the Mann-Whitney test), there were no significant differences between the patients who survived and those who did not during their ICU stay, in age, sex, NIV or tracheotomy prior ICU stay, cause of ARF, arterial blood gas and chest radiograph on ICU admission, or respiratory management in ICU.
A median of 3 (1–6) years passed from the first ICU admission in the present study to the final assessment (June 15, 2008). At that time, 2 patients were lost to follow-up and 50 had died (mortality rate 58%). The probability of survival was significantly higher in the hereditary group than in the acquired group (Breslow test = 6.49, P = .011). (Fig. 3). The median time to death was 6 (4–8) years in the hereditary group and 3 (1–5) years in the acquired group. Age and SAPS II were the 2 covariates that did not meet the assumptions for the proportional hazards, so we entered the interaction between each of them and time to death into 2 separate Cox models (Table 6). The diagnosis of neuromuscular disease was not significantly associated with death in model A or model B. The covariates that were significant predictors of death were the interaction between time to death and age, in model A, and SAPS II, in model B. At the final assessment, 39 patients (46%) were on NIV, and 25 (29%) were on tracheotomy (see Table 2), and these proportions were not significantly different between the 2 groups.

Kaplan-Meier graph of cumulative survival probability in patients with hereditary versus acquired neuromuscular disorders.
Cox Proportional Hazards Models for Long-Term Survival
Discussion
We found that:
NIV was the first ventilation method used during the ICU stay.
The rate of NIV use differed across the neuromuscular diseases.
The rate of tracheal intubation was substantial.
Long-term outcome was independent of the underlying disease, after controlling for some confounding factors.
Limitations
This study was retrospective, so some data are lacking. In particular, we could not precisely assess the physiotherapy administered. Second, the study starting point was the first stay for ARF in our ICU, so we did not account for previous stays in our ICU for reasons other than ARF, previous stays in other ICUs for ARF, or stays in other ICUs during the follow-up period. Therefore, our study underestimates these patients' use of ICU resources. Also, the number of patients was small.
This study's long time span is also a potential weakness, in that our practices may have changed; however, we do not think we made any important changes in our medical or physiotherapy management of these patients during the study period, and it was a single-center study, so there were no inter-center practice differences. However, that it was a single-center study limits the generalizability of the findings. In particular, physiotherapists are not used in many countries. This study provides a picture of contrasted neuromuscular diseases, some of which, such as hereditary neuromuscular disorders, are rarely reported on in the acute care setting. Finally, it provides information on long-term outcome that is also rarely reported.
In a recent international survey of ICU mechanical ventilation practices, neuromuscular disorders were found to be the indication for the initiation of mechanical ventilation for ARF in less than 10% of cases.11 Our study shows that that proportion may change over time. In the years covered by the international survey (1996 and 1997), neuromuscular patients accounted for less than 1% of our ICU admissions. Given that 60% of our ICU patients receive mechanical ventilation, the incidence of neuromuscular patients among those mechanically ventilated is roughly 1.2%, which is below the lower range in the countries surveyed.11 We have no explanation for this discrepancy, apart from the different case mix.
In the present study we administered NIV in 72% of the patients during their ICU stay, which indicates that NIV is our first choice, though 35% of the patients were on home NIV before ICU admission. From the literature, the level of evidence to support the use of NIV in this setting is low. In a small case-control study, mortality and ICU stay were with NIV combined with mini-tracheotomy in 14 patients with hypercapnic ARF (8 hereditary muscular dystrophy and 4 ALS).12 However, the mini-tracheotomy is definitely not a noninvasive means. An open study with 17 patients with neuromuscular disease found NIV effective in avoiding tracheal intubation in 79% of the patients.13 A randomized controlled trial that compared NIV (32 patients) to usual medical care (29 patients) in patients with ARF, sub-grouped according to the underlying respiratory disease, found less need for tracheal intubation with NIV.14 Mortality was not different between the 2 groups. In that study the number of patients with neuromuscular disease was very small. Swallowing disorders may further complicate the use of NIV and compromise its effectiveness.
Our study's retrospective design precludes any conclusions regarding benefit or harm from NIV. Note that our NIV rate was also due to the fact that it was used after extubation. Our high rate of NIV use and success in this study is explained by the skills of our team of physiotherapists, who have been involved for many years in applying NIV and clearing secretions, either manually or instrumentally. Unfortunately, we don't have enough data to objectively determine the impact of physiotherapy management. The role of airway secretion management by physiotherapists, either done manually or with intermittent positive-pressure breathing or mechanical insufflation-exsufflation, is well known.15 On a case-by-case basis in patients in the present cohort, we observed that intensive physiotherapy, close clinical monitoring, and NIV can be effective in treating ARF and thus avoid tracheal intubation.
The rate of tracheal intubation in the present study was 43% (37/87), across the neuromuscular diseases. Apart from myasthenia gravis, the tracheal intubation rate in patients with neuromuscular diseases such as hereditary muscular dystrophy and ALS is largely unknown, since reports have focused on the patients who received intubation. As an example, Bradley et al retrospectively reviewed 24 patients with motor neuron disease, all of whom had undergone tracheal intubation for ARF.16 Seventy-one percent of them were discharged alive from the ICU, which is close to the 76% of intubated patients in the present study who were discharged alive. In patients with myasthenia gravis our intubation rate was 83%; in myasthenia gravis lung volumes change sharply,17 and in that unstable situation, intubation is a safer way to deliver mechanical ventilation. Some uncontrolled studies suggested that NIV might reduce the need for tracheal intubation in myasthenia gravis.18
The long-term outcomes of our patients with neuromuscular diseases after an ICU stay for ARF were poor. In a study of a very large national database in Sweden, Laub et al reported the outcomes of 1,526 patients receiving home mechanical ventilation and found that one of the determinants of long-term mortality was the initiation of mechanical ventilation in an acute setting, which occurred in 32% of patients with neuromuscular disease, and 17% of patients with ALS.19 In our study, severity of illness and age at the time of ICU admission for ARF were the only covariates significantly associated with death, in interaction with time to death for both of them. A previous report from our department reported that the 5-year survival rate in patients with muscular dystrophy treated with tracheotomy and invasive mechanical ventilation was 65%.20 Then, when NIV emerged as an option for long-term ventilatory management, the muscular dystrophy patients followed at our institution were the first to be treated with this technique. The probability of continuing NIV 3 years after its onset was 40% in the 16 muscular dystrophy patients surveyed.21 The reasons for discontinuing NIV were discomfort, a switch to tracheotomy, or death. The probability of continuing NIV was lower than in patients with kyphoscoliosis or tuberculosis sequelae, where it was as high as 80%.21 In other reports the outcome was better, as the 5-year actuarial survival rate in 29 patients with neuromuscular disorders treated with NIV was 81% (95% CI 61–100%).22
Conclusions
In our ICU, chronic neuromuscular disease was an uncommon cause of ARF. In these patients we frequently use NIV, but also intubation. There was a low probability of ICU death. Long-term outcome was independent of the neuromuscular disease.
Footnotes
- Correspondence: Claude Guerin MD PhD, Service de Réanimation Médicale et d'Assistance Respiratoire, Hôpital de la Croix Rousse, 103 Grande Rue de la Croix Rousse, 69004 Lyon, France. E-mail: claude.guerin{at}chu-lyon.fr.
-
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}