

Abstract
With the introduction of the stair climb test of surgical patients in the 1950s, the role of exercise-based testing as a useful diagnostic tool and an adjunct to conventional cardiopulmonary testing was established. Since then, we have witnessed a rapid development of numerous tests, varying in their protocols and clinical applications. The relatively simple “field tests” (shuttle walks, stair climb, 6-minute walk test) require minimal equipment and technical support, and so are generally available to physicians and patients. At the other end of the spectrum is the cardiopulmonary exercise test (CPET), more complex in its equipment requirements, technical support, and with an often complex interpretive strategy. The 6-minute walk test (6MWT), in particular, has evolved into a versatile study with diagnostic utility in many disorders, including COPD, pulmonary hypertension, interstitial lung disease, congestive heart failure, and in the pre-surgical evaluation of patients, among others. With the added dimensions of optional O2 saturation monitoring and calculated post-exercise heart rate recovery, the 6MWT is providing important clinical information well beyond the measure of distance walked. Is it sufficiently robust and informative to replace the more demanding and less available CPET? In many instances, the clinical applications are overlapping, with the 6MWT functioning as an adequate surrogate. However, in the initial evaluation of unexplained dyspnea, in formal evaluation of impairment and disability, in detailed evaluation of congestive heart failure, and in the selected lung cancer patient prior to resection, CPET remains superior. Investigations of portable metabolic and cardiovascular monitoring devices aiming to enhance the diagnostic capabilities of 6MWT may further narrow or close the remaining gap between these two exercise studies.
Introduction
A January 2011 JAMA paper reporting on the importance of gait speed in the elderly promptly captured the interest of the popular media.1 It was then widely broadcast to an interested but somewhat puzzled public that men and women aged 65 years and older who walked at a faster pace also tended to live longer. Uncertain about its meaning, some aimed to quicken their gait to derive the reported benefit. Whatever the popular interpretation of this reported observation, it succeeded in advancing the idea that there is something of importance to be learned from observing humans in motion.
Similarly, healthcare professionals who evaluate or treat patients in a wide range of clinical settings are increasingly aware of the value of movement-based testing. This growing recognition has fueled an unprecedented development in the methodologies of testing, with ever expanding applications. Exercise testing of patients has evolved into a dynamic and vibrant field of study that cuts across multiple disciplines and disease processes. The current variety of exercise tests provide clinicians and investigators with useful tools to make assessments of functional status that compliment and extend the information gained from studies performed in a resting state.
Pulmonary Function Tests: The Current State
Pulmonary function testing at rest represents a time-honored tool that has aided the clinician in a broad range of scenarios. Its principal purpose, in simplest terms, is to distinguish normal from abnormal respiratory health and to define respiratory physiology. Longstanding perceptions of underutilization, variable quality of measurements, and disagreements of appropriate reference values and interpretive strategies serve to limit their value in patient care.
Analysis of an exhaled FVC is the basis of spirometric testing designed to detect obstructive airway disease. However, interpretative strategies based on percentile-based limits compared with percent of predicted conventional limits of normality are very much under active discussion, with a suggested misdiagnosis of as many as 20% of healthy patients referred for spirometric studies when fixed limits are utilized.2–7
Lung volume measurements performed either by constant volume/variable pressure body plethysmography, or by gas rebreathing methodology aim to identify and distinguish restrictive impairment from hyperinflation and from healthy lung volumes. As these methods reflect the static compliance properties of the entire respiratory system (lung and chest wall), the recordings are influenced by both pulmonary disorders and extra-pulmonary factors. The lung volume test results therefore often require correlation with physical exam and imaging studies. Newer applications of lung volume recordings include the use of inspiratory capacity before and after bronchodilator as a measure of dynamic hyperinflation and the impact of therapy.8 This is based on a recognition that hyperinflation reflected in inspiratory capacity/total lung capacity is a stronger corollary to dyspnea, exercise tolerance, and ultimately to survival than FEV1 in severe airway obstruction.9
Evaluating the efficiency with which the lungs transfer gas from inhaled air to the capillary blood is the aim of the single-breath carbon monoxide diffusing capacity measurement (DLCOsb). As a measure of the alveolar-capillary surface area for diffusion, it is the only routinely performed pulmonary function test (PFT) that is sensitive to vascular abnormalities. Its isolated reduction in the presence of normal spirometry and lung volume recordings may be an early clue to the presence of pulmonary vascular disorders. Care must be taken to identify spurious reductions in DLCOsb values due to anemia or to elevated carboxyhemoglobin (CO-Hb).
Resting PFTs provide useful information in a variety of settings. Indeed, in monitoring the progress of patients with asthma and COPD, spirometry at regular intervals is strongly encouraged. As predictive factors, changes in FVC and DLCOsb following one year of therapy are strongly predictive of survival duration in patients with idiopathic pulmonary fibrosis (IPF).10
In many symptomatic individuals, PFTs alone do not provide an explanation, or may not correlate with the level of functional impairment. In some instances, as for example, prior to lung resection surgery, cardiovascular health is an important determinant of a successful outcome. In this setting, and in numerous others, resting pulmonary measures will not suffice, and a broader data set of motion-based recordings is required. This need is increasingly addressed by a variety of exercise tests, whose discussion of methodology, utilization, and clinical value forms the remainder of this review. More detailed treatments of conventional pulmonary function testing are to be found in other papers that compose the present symposium.
Exercise Tests: The Theory
In the healthy state, exercise tolerance is ultimately limited by the oxidative ability of skeletal muscle, commonly termed aerobic conditioning. With advancing lung disease, limitations of ventilation and gas exchange can become more prominent, but may not be absolutely limiting until the very end stage. In time, the inactivity that accompanies advanced lung disease reduces muscle strength and conditioning and so further reduces exercise performance. Finally, the additional debilitating effects of concurrent illnesses that share common risk factors with chronic lung disease (eg, organic heart disease, neoplasia) may adversely influence strength and activity tolerance, but not alter PFT measurements.
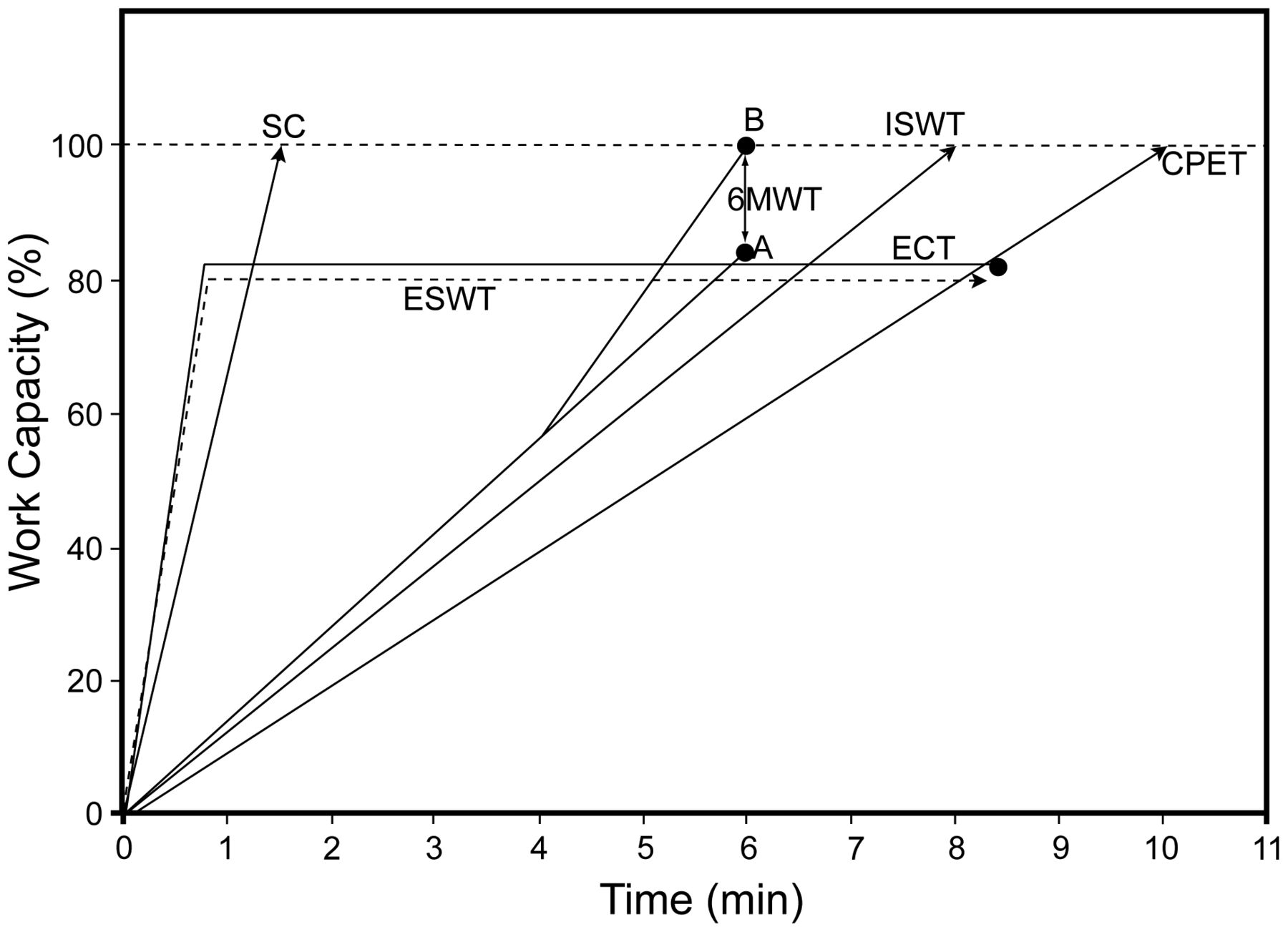
For these reasons, it should not be surprising that recordings of airway function, lung volumes, and gas diffusion properties alone may not adequately reflect daily functional status. It is these observations that historically have triggered the development of exercise testing of various designs (Fig. 1). A range of tests are in current use and so will be described, with a particular focus on and comparison of the 2 most evaluated and utilized studies, the 6-minute walk test (6MWT) and the cardiopulmonary exercise test (CPET).

Schematic representation of the major modes of exercise testing, including stair climb (SC); exercise challenge test (ECT); 6-minute walk test (6MWT) for healthy, mild (A) versus moderately to severely impaired (B); endurance shuttle walk test (ESWT); incremental shuttle walk test (ISWT); and cardiopulmonary exercise test (CPET). Protocols specify either a time limited end point (—●) or a symptom-based physiologic end point (→), and designate a maximal (100% work capacity) or non-maximal character.
Exercise Tests: The Methods
Stair Climbing
This simple but poorly standardized modality of exercise testing was introduced in the 1960s, chiefly as a preoperative assessment tool involving thoracic surgery patients.11,12 Stair climbing continues to be used in a limited numbers of clinical centers, largely due to its simplicity. Results have been associated in clinical reports with postoperative complications and hospital stay, reflecting costs.
The test consists of asking patients to climb as many stairs as possible to the point of exercise end, or dizziness, chest pain, or, more typically, dyspnea and leg fatigue.
The results are recorded variably as the number of stairs climbed, the flights of stairs ascended, or the time required to ascend the designated number of stairs.11,12
Variations have included attempts to measure oxygen consumption (V̇O2), but the additional equipment impeded patient effort and has not gained acceptance.11 Von Nostrand reported, in a retrospective review, that patients who were able to climb 2 flights or more had a postoperative mortality of 11%, versus a rate > 50% for those unable to climb that height.12 In a series of 109 patients more than 70 years of age who underwent pulmonary lobectomy for lung carcinoma, Brunelli determined that preoperative “low height climbed,” along with concurrent cardiac disease were the most significant predictors of postoperative complications.13 While not widespread, limited use of stair climbing is still practiced by experienced surgeons who appreciate its global character and simplicity.
Exercise Challenge Test
Exercise-induced bronchoconstriction (EIB) is a commonly experienced feature of asthma. Exercise challenge testing (ECT) is occasionally indicated for clarification of symptoms and to evaluate therapeutic or preventive treatment. One major stimulus to EIB involves the excessive loss of airway heat and water accompanying high minute volumes (V̇E). ECT aims to simulate these conditions. Although not as sensitive a study as methacholine provocation for the detection of nonspecific airway hyper-responsiveness,14,15 this study is often helpful in individuals with known or suspected asthma who perform tasks with high ventilatory demands (eg, athletes, military, firefighters).15 In these settings, ECT may be uniquely advantageous.
The protocols by which subjects are tested reflect some variations, although the American Thoracic Society (ATS) guidelines propose standardization to assure quality.15 Resting hyperpnea at up to 60% of predicted maximal voluntary ventilation (utilizing a gas mixture including 5% CO2, to avoid symptomatic hypocarbia) may be attempted in patients unable to perform general exercise during the test period. However, it does not precisely simulate all of the conditions that influence airway response to exercise, including the potentially bronchodilating influence of endogenous catecholamine release,16 and thus is not the preferred method of testing. Physical exercise performed via treadmill or by cycle ergometry are the recommended practices.
Treadmill exercise involves selection of speed and treadmill grade to produce 5 minutes of exercise near maximum work and ventilatory levels. Oximetry can monitor both oxygen (O2) saturation and heart rate, but it is principally the minute ventilation (target 40–60% of maximal voluntary ventilation) that represents the principal stimulus to EIB. The highest level of stimulus should be continued minimally for 5 min. Dry air from compressed gas tanks, with or without associated cooling below freezing temperatures, will strengthen the stimulus to EIB. Where the required equipment is available, this additional feature is recommended. Use of nose clips to block inhalation of better humidified ambient air is recommended, to strengthen the provocation.15
Following cessation of exercise, subjects are tested with spirometry at 5, 10, 15, and up to 30 min. Spirometry is performed at 2−3 repetitions, with the greatest value of FEV1 selected for comparison to pre-exercise baseline values. Ten percent reduction from baseline is considered abnormal, with 15% reduction in FEV1 diagnostic of EIB.
ECT as a study is safe, as unexpectedly severe or prolonged responses are rarely encountered. Nevertheless, the equipment for patient evaluation (eg, eletrocardiogram, oximetry), and properly trained personnel must be present close to the test site. A detailed treatment of this modality in the evaluation of suspected asthma is found elsewhere in these conference papers.
Shuttle Walk Test
An effort to develop a simple field test to quantitate the disability in patients with chronic airway obstruction produced the shuttle walk test (SWT). This development, published in 1992,17 aimed to eliminate variability between test subjects due to self-pacing (as in stair climbing or 6MWT) and within a test subject on serial studies. This is accomplished by setting an externally dictated tempo via an electrical metronome device that emits a tone for each stride. This course covers a distance of 10 meters between two traffic cones, with the pace increased by a set amount (0.17 m/s) every minute. The test is concluded when the individual stops because of prohibitive symptoms, the inability to maintain the directed pace, or when the entire course is completed. The entire test consists of 12 stages, with results principally reported as distance walked.17 This protocol, describing the incremental SWT (ISWT), was designed as a maximal study (ie, aiming to achieve and define maximum V̇O2). Validation of the ISWT distance-peak V̇O2 association was reported in stable COPD patients by Benzo and Sciurba in 2010.18 In this study of mild to severely impaired individuals, a portable metabolic computer recorded an achieved peak V̇O2 in the final minute of testing of 18–26 mL/kg/min. To date, however, there are no accepted reference values to identify and distinguish healthy versus impaired subjects for a given age or sex. The maximal nature of this relatively simple field test may have other applications. One may be serial testing in patients undergoing treatment changes (ie, to functionally evaluate the effect of a bronchodilator or pulmonary rehabilitation).19 Future studies designed to determine minimal distances representing significant change should make ISWT more useful and likely encourage broader utilization.
In order to broaden the diagnostic information provided by the SWT, and specifically to reflect an individual's endurance and capacity to perform sustained activity, a modification was introduced. In this version, the test subject would reach and maintain a predetermined submaximal level of exertion, but would retain the external pacing, to reduce the variability, due to motivation, encouragement, or individual strategy. Thus was conceived the endurance SWT (ESWT), a variant of the earlier incremental study.20
Performance of ESWT requires an initial ISWT in order to determine maximum sustainable walking speed. Walking pace is then calculated as 85% of the maximum and is maintained for the duration of the study, up to a maximum of 20 min. In the performance of this study, an initial 2-minute warm-up period at a reduced walking speed is permitted in order for the test subject to become familiar with the course surface and other conditions. Following a triple signal, the patient increases speed to the maintenance walking pace, then is instructed to walk until severe breathlessness, fatigue is experienced, or until the maximum allowable 20 min have elapsed.
The primary reported measure in the ESWT is walking time in seconds (rather than distance, as in ISWT). Optional measures of heart rate, O2 saturation, and subjective indices of dyspnea on exertion as perceived by the test subject may be reported.
6-Minute Walk Test
The 12-min walk, the earliest of the simple timed walk tests, was introduced by Cooper, as a fitness test for highly conditioned individuals. In time, it was adopted for use by the military to assess the benefits of their training programs.
As the 12 min duration exceeded the capabilities of pulmonary impaired individuals, Butland et al studied similarly conducted protocols lasting 2 minutes and 6 minutes.21 A comparison of the 3 outcomes revealed that the 2-min walk was less powerful in distinguishing impairment from normal health, while the 12-minute duration appeared unnecessarily exhausting. The intermediate, 6-minute duration appeared to be the most attractive option, producing the current 6MWT. Unlike the ISWT, the 6MWT is sub-maximal, that is, most exercising subjects do not achieve peak V̇O2. However, in the moderate to severely impaired individual (eg, COPD, congestive heart failure), maximum V̇O2 will nearly be achieved during the 6MWT study (see Fig. 1).
In order to reduce variability between test subjects, and to improve reproducibility in a given individual, standards for conducting the 6MWT were established by the American Thoracic Society Pulmonary Function Standards Committee.22 These guidelines specify a 30-meter linear track marked by plainly visible cones, in an enclosed corridor with a flat, firm surface to provide sure footing (Fig. 2). Warm-up practice sessions are discouraged. Instructions to test subjects are to be given before the start, with only brief updates, using standardized phrases to be spoken at one-minute intervals thereafter. While pausing as needed is permitted, in keeping with the “self-paced” character of the study, assistance in carrying O2, and verbal encouragement are to be avoided as they introduce substantial variability.22,23

Six-minute walk test in progress. A test subject is rounding a traffic cone marking one end of the 30-meter course, in an enclosed space, and on a level walking surface. The simple format and equipment requirements of this “field test” are in contrast to the technical complexity of the cardiopulmonary exercise test (see Fig. 4).
The principal outcome is distance, in meters or feet. Over time, Borg scores for dyspnea and fatigue, and oximetry at baseline and at end-exercise have become so commonly employed as to become nearly standard features. Further enhancements include assessments of heart rate recovery (HRR), a feature utilized to great advantage in the cardiovascular assessment of patients.24 Enhanced portable hemodynamic and metabolic monitoring have also increased recovery of diagnostic information in particular patient groups. The perceived value of these optional measurements is still under investigation, and is further discussed below.
Treadmill 6-Minute Walk
In areas where 30-meter distances were not available, and where treadmills were familiar to patients, the 6-minute walk on treadmill has been adapted and compared to corridor walking. In some studies, the achieved distances were comparable,25 while in other areas the treadmill distance was nearly 15% lower.26 This may reflect the need for constant pace changing and possibly problems of balance for people not familiar with treadmill walking. While treadmill utilization has the appeal of easier cardiac and oximetry monitoring, and eliminates the need for a long, isolated, and specifically dedicated corridor, it reduces the “self-paced” character of the study, which is an integral characteristic of the distances achieved (6MWD). Nevertheless, in certain settings, the treadmill 6MWT continues to be used, at 0% elevation and at a constant speed that is selected for comfort and adapted to the individual test subject.26
Normal distances and minimal clinically important differences have covered a broad range, and reference equations for men and women have been proposed.27,28 Recent published work of the 6MWD project (Asociación Latinoamericana del Tórax [ALAT]), studying 444 subjects from 7 countries, ranging in age from 40 to 80 years, determined a mean 6MWD of 571 ± 90 meters (range 380 to 782 meters), with males walking on average 30 meters farther than females. Age was a significant influence on the walk distance in all of the 10 participating centers, with distance walk declining to a significant degree in the older population. Age specific reference standards were constructed for male and female subjects.28
Inherent variability of the self paced 6MWT requires a determination of minimal clinically important difference. To date, this has been estimated for the COPD population to be between 54 and 80 meters.29 In the population with idiopathic fibrosis, the measure was derived from a multicenter trial of interferon-γ1B in 126 patients. The obtained data of serial 6MWD in the test population determined a minimal clinically important difference between 24 and 45 meters in this population.30
The versatility of the 6MWT is reflected in its stand-alone importance in a variety of clinical settings, as well as its incorporation with other test metrics (eg, body mass index, degree of obstruction, a shortness of breath questionnaire, and exercise index into a “BODE [body mass index, air-flow obstruction, dyspnea, exercise capacity] index” metric predictive of mortality in COPD).31 Finally, while oximetry is often recorded at the start and at end-exercise, the 6MWT is not well suited for O2 titration, given the importance of uninterrupted self pacing.
Despite its many virtues, an important weakness of the 6MWT is the nonspecific nature of the result. A reduced 6MWT distance reflecting general functional impairment does not specify an etiology. Consequently, if not previously established, a search for an etiology requires further laboratory, radiographic, and clinical investigation to establish causality.
Cardiopulmonary Exercise Test
Any exercise involves a coupling of respiratory function, cardiovascular performance, and ultimate O2 uptake and utilization by peripheral tissues. CPET, by noninvasive assessment of inspired O2 (V̇O2), and expired CO2 (V̇CO2), is uniquely able to evaluate the contribution of respiratory, cardiovascular, and peripheral tissue function in support of maximal exercise. The complexity of this study is substantially greater than other functional exercise testing, with a greater equipment requirement, and often complex interpretation strategies.32 As such, it is not widely available in all settings of clinical practice. However, its unique contributions to patient assessment are well recognized and of considerable value.
CPET, when used to its maximal capability, has numerous clinical applications (Table 1). It is potentially useful in distinguishing cardiovascular from respiratory causes of limitation in patients in whom preliminary testing has not proved diagnostic. In established cardiovascular patients it is useful in determining prognosis in heart failure, eligibility for cardiac transplantation, and evaluation of therapeutics.33 In chronic respiratory impairment, its value is established in a broad spectrum of chronic obstructive lung disorders, diffuse parenchymal disease, and pulmonary vascular disorders.34,35 In the thoracic surgical candidate, peak O2 consumption corrected for body weight (mL/kg/min) is a strong prognosticator of postoperative complications and mortality, and has been a key discriminating factor in patient selection for lung-volume-reduction surgery.32,34,35
Characteristics and Applications of 6-Minute Walk Test Versus Cardiopulmonary Exercise Test
Optional monitoring performed during CPET includes arterial blood gas testing for evaluation of alveolar arterial O2 difference, and of acid/base balance. Of substantial value in the ABG determinations at baseline and at peak exercise are differences in serum pH and serum bicarbonate (HCO2) in helping to assess the adequacy of the exercise effort. In place of invasive placement of arterial catheter for continuous arterial blood sampling, arterial puncture at baseline and at the moment of exercise cessation has been proposed in an effort to harvest the uniquely important information with less pain and morbidity. While the discrete sampling at two points in time is widely practiced, there is no uniformity of opinion about the adequacy of this approach, based on rapid degradation of PO2, PCO2, and pH profiles.
Pulse Oximetry: Its Role in Exercise Testing
Pulse oximetry is utilized in the performance of cardiopulmonary exercise testing, and is a commonly used option in the 6MWT. It is performed both for reasons of patient safety and for its diagnostic value. Following its invention by Takuo Aoyagiao in the early 1970s, pulse oximetry has yielded important diagnostic and safety benefits, initially in the care of neonatal, pediatric, and adult patients in intensive care settings and in surgical suites. As its use expanded beyond the resting patient to exercise, the limits of its technology and accuracy have been tested. A review of 2,429 patients evaluated at the Cleveland Clinic, who had both arterial blood gas (PO2) and simultaneous pulse oximetry (SpO2) readings indicated that oximetry overestimated O2 saturation, failing to detect hypoxemia, in 154 individuals (Fig. 3). Conversely, pulse oximetry underestimated O2 saturation in a smaller number of test subjects (n = 92) (unpublished data).

Pulse oximetry overestimates ventilation/perfusion matching. Comparison of room air oxygenation recordings by arterial blood gasses (RA PO2) with simultaneous pulse oximetry measures (RA SpO2). Highlighted are threshold values of hypoxemia (RA PO2 55 mm Hg vs RA SpO2 88%) in 2,599 subjects.
Studies of different models of pulse oximeters indicated differences related to diverse calibration algorithms of the respective instruments.36 A study of oximetry in exercising patients utilizing both ear probe models and finger probe equipped instruments noted limited accuracy in settings of severe desaturation, and owing to variations in signal strength, with mild superiority noted in the finger over the ear location.37,38
New generation oximeters now widely in use employ enhanced signal processing algorithms and improved hardware to reduce sensitivity to motion and to variations in perfusion.39
In the 6MWT, O2 saturation by pulse oximetry is commonly recorded pre-exercise, and at the cessation of exercise.27 Multiple readings during the 6MWT for the purpose of O2 titration compromise the principal design and end point of the 6MWT (self pacing and total distance walked), and thus are incompatible with a well performed study. If O2 titration is desired, alternative testing (ie, without regard to distance walked or gait speed) should be scheduled and performed via standard protocol.
What Is Post-Exercise Heart Rate Recovery?
The adequacy of heart rate response to exercise (chronotropic competence) has long been an important indicator of cardiac health in exercising individuals. More recently, the rate of heart rate normalization (HRR), typically measured as a reduction in heart rate (HR/min) in the first minute following cessation of exercise has drawn increasing attention as an important marker of cardiovascular status.40
The basis for this measurement is the concept that an altered balance within the autonomic nervous system (“autonomic dysregulation”) is of central importance in the pathogenesis and progression of cardiac disease.41⇓–43 The imbalance favors an increase in sympathetic influence (“sympathetic dominance”), with a diminished role of the parasympathetic system (“parasympathetic withdrawal”). Thus, the measure of heart rate normalization following exertion becomes a simple and easily obtained index of parasympathetic/vagal function. Abnormal post-exercise HRR is typically defined as a first minute decline of less than 18 beats/min when exercise stops abruptly, or less than 12 beats/min when a cool-down period is employed.41,42 To avoid confusion and error, this post-exercise measure must be clearly distinguished from earlier established measures of heart rate response adequacy during exercise (heart rate response and heart rate reserve). These indices are distinct from the currently discussed heart rate recovery, but share the identical acronym (HRR).
Clinical reports of the post-exercise HRR in often large patient cohorts highlight its value in cardiopulmonary disorders. In 2,935 patients studied at the Cleveland Clinic, impaired HRR predicted mortality independent of coronary disease severity.44 Other reports associated impaired HRR with subsequent occurrence of new onset atrial fibrillation,43 with mortality in congestive heart failure,24 and with severity of coronary disease in a cohort of 208 patients,45 a finding at variance with the aforementioned report.44 On a hopeful note, studies of obese individuals with cardiac dysfunction and with metabolic syndrome showed improvement in cardiac function and in HRR following programs of exercise and weight reduction.46,47 These findings indicate that abnormal post-exercise HRR associated disease is not inevitably progressive but may be favorably impacted and partially reversed in high risk individuals by improving aerobic conditioning and reducing risk factors. The recognition of HRR as an index of cardiovascular health triggered interest in patients with diffuse parenchymal lung disease who may have concurrent circulatory impairment. In separate reports of patients with IPF, Swigris described impaired HRR following 6MWT as a predictor of pulmonary hypertension in IPF and of increased mortality.48,49
Referring the Patient for Exercise Testing: 6MWT Versus CPET
Recognizing the diagnostic value of exercise related testing, an often challenging decision, confronts the clinician: which test to order? Occasionally, the decision is influenced by the local availability of testing modalities and institutional expertise. In an ideal situation, the choice should rest on the desired characteristics of the studies, and on the clinical question to be answered.
CPET is a maximal exercise study whose multiple measurements and often complex interpretive strategies are designed to reliably detect and distinguish one or more sources of functional impairment. 6MWT on the other hand, is principally a sub-maximal, simple “field test” whose principal measure is the distance walked. In its simplicity, it more closely simulates daily function and so provides valuable information. While CPET and 6MWT are of comparable value in a range of clinical settings (see Table 1), it should be clearly noted that CPET is either preferred or uniquely advantageous in the following.
Unexplained Dyspnea
The noninvasive recordings of respiratory gas exchange (V̇O2, V̇CO2) related to other cardiorespiratory variables (eg, cardiac output via the Fick equation) makes CPET uniquely suited to identify causes of functional impairment not characterized by prior physical exam or preliminary studies.15,33,35 6MWT is not designed to identify specific etiologies of impairment and should not be used for this indication. Once identified, however, 6MWT may be utilized longitudinally to monitor the natural course, response to therapy, and to prognosticate in a range of cardiopulmonary disorders.22,27
Evaluation of Impairment and Disability
A World Health Organization 1980 statement formally defined impairment (“any loss or abnormality of psychological, physiological, or anatomical structure or function”) and disability (“any restriction or lack, resulting from impairment, of ability to perform an activity within the range considered normal for a human being”).50 Disability is typically determined by administrative or legal instruments. When required, CPET measurement of work capacity (peak oxygen consumption [V̇O2/kg]) provides an objective basis for determination of the presence and degree of impairment, not disability. Once again, 6MWT is not designed to meet the requirements of this task (see Table 1).
Congestive Heart Failure
While both exercise studies have reported value in the evaluation of cardiac disease, the multiple dimensions of recorded measurements in CPET (peak V̇O2, V̇O2 at anaerobic threshold, ventilatory equivalent for carbon dioxide [V̇E/V̇CO2], and post-exercise HRR) provide highly reliable, clinically useful information in every phase of disease management: at diagnosis, to evaluate response to therapies, to offer prognosis, and to evaluate candidacy for transplantation. Of particular interest is the reported clinical value of the aforementioned V̇E/V̇CO2 slope. This measure is recorded continuously throughout the exercise trial but is indexed and reported at anaerobic threshold. While respiratory physicians regard this as an indicator of pulmonary “dead space,” cardiovascular exercise physiologists term elevated values as “ventilatory inefficiency.” This exaggerated ventilatory response to exercise-related CO2 production is noted in advanced cardiac impaired individuals. Its prognostic value in congestive heart failure patients is on a par with peak V̇O2,51,52 and serves to improve risk stratification in moderate cardiac patients when the 2 are combined.53 As a marker of respiratory dead space and so the state of the pulmonary circulation, elevated V̇E/V̇CO2 slope reportedly indicates right-ventricular dysfunction in patients with left-ventricular systolic failure.54
Thoracic Resection Surgery
Evidence-based standards of physiologic assessment before planned thoracic resection surgery begins with PFTs. Surgical candidates with predicted postoperative (ppo) FEV1 values below 40% predicted, or ppo DLCO values below 40% predicted should undergo CPET evaluation to measure maximal oxygen consumption (V̇O2max).55
Peak V̇O2 levels below 15 mL/kg/min derived from CPET predicts increased perioperative complication and mortality risk. Decisions will typically rest on individual assessment of age, comorbidities, etc. Peak V̇O2 levels below 10 mL/kg/min predict very high perioperative risk and compel consideration of non-surgical therapy. Where CPET cycle ergometry or treadmill facilities are not available, stair climbing less than one flight of stairs roughly corresponds to a peak V̇O2 less than 10 mL/kg/min, the highest risk category.
The 6MWT, unlike the CPET or even the stair climb test, is not a maximal test in all but severely impaired patients. Consequently, no direct measure of maximal V̇O2, nor even a correlation with 6MWT distance with levels of V̇O2max, is possible. It does not therefore meet the requirements of optimal preoperative assessment of risk as posited in the American College of Chest Physicians statement.55
Exercising Your Patient: A Look to the Future
Promising trials are underway seeking to bridge the existing gap between 6MWT and CPET capabilities through enhanced portable monitoring. A trial of 6MWT in patients fitted with a lightweight (950 g) metabolic monitor with face mask yielded measures of V̇O2, V̇CO2, V̇O2 peak, breathing reserve, HR, and O2 saturation, in addition to the expected distance walked. The results included some surprising results (eg, patterns of ventilatory limitation in over 20% of patients with a diagnosis of pulmonary hypertension). These, among other unexpected data in the multiple diagnostic groups, led to treatment changes directly related to the findings.56
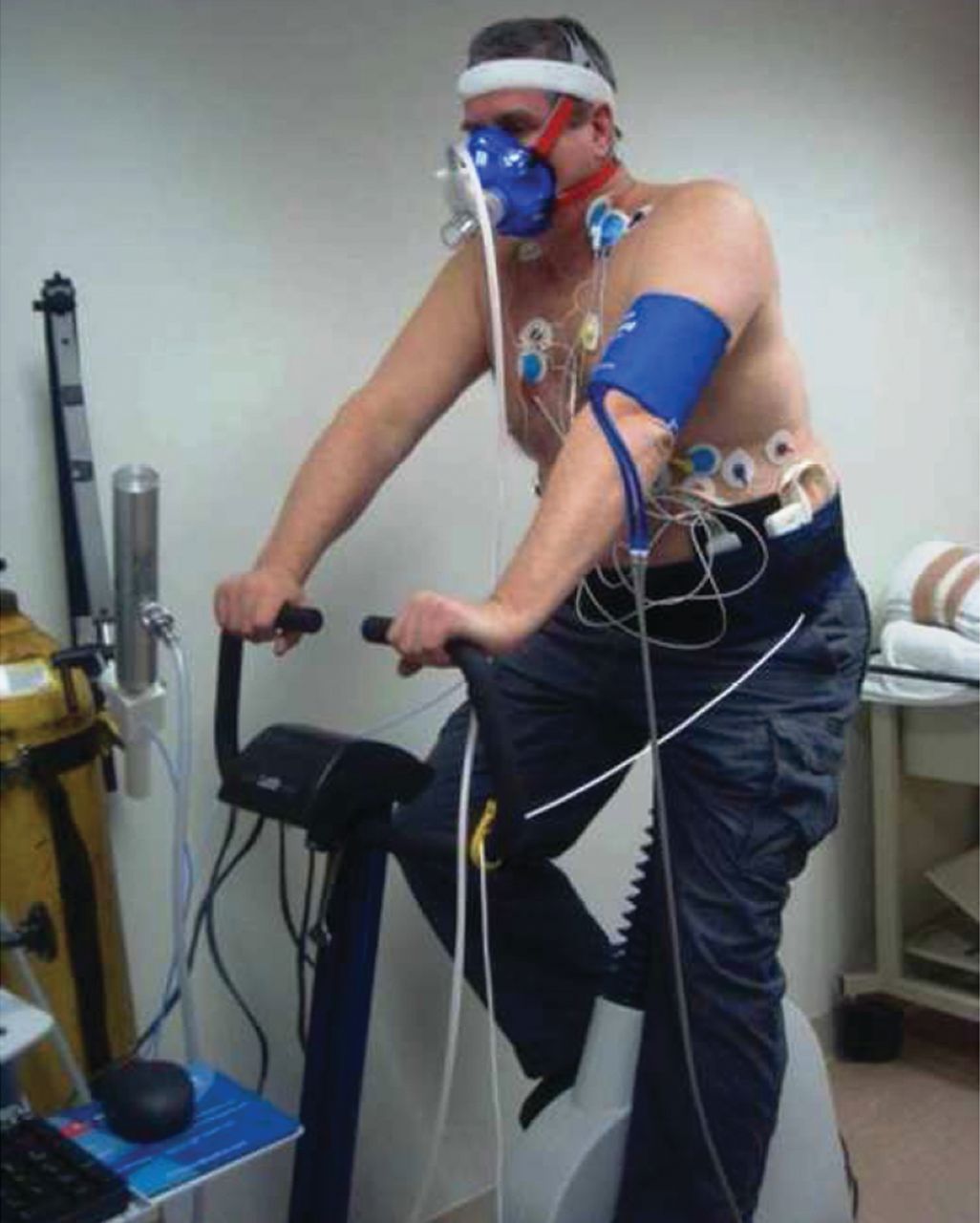
Another project currently in progress aims to introduce portable hemodynamic monitoring via impedance cardiography to 6MWT and CPET in pulmonary hypertension patients. Earlier trials of this technology by Tonelli et al57 in the critical care setting demonstrated excellent agreement between impedance cardiography measures of cardiac output with cardiac output calculations by Fick equation and by thermodilution methodologies. The lightweight portable impedance cardiography electrodes and transmitter (PhysioFlow, NeuMeDx, Bristol, Pennsylvania) affixed to the test subject offers no impediment to maximal performance (Fig. 4). The first derivative of instantaneous impedance variation signal (dZ/dt), directed at the thoracic aorta, is transmitted to a portable laptop via Bluetooth transmitter/receiver apparatus, and displayed on the computer screen in real time, both digitally and as trends of heart rate, stroke volume, cardiac output, and cardiac index (Fig. 5).

Cardiopulmonary exercise test via cycle ergometry in progress. In addition to the white colored electrocardiogram leads, evident also are the blue colored leads of impedance cardiography. The light, portable impedance cardiography instrument is secured in a waist holster, visible at the left side of the test subject.
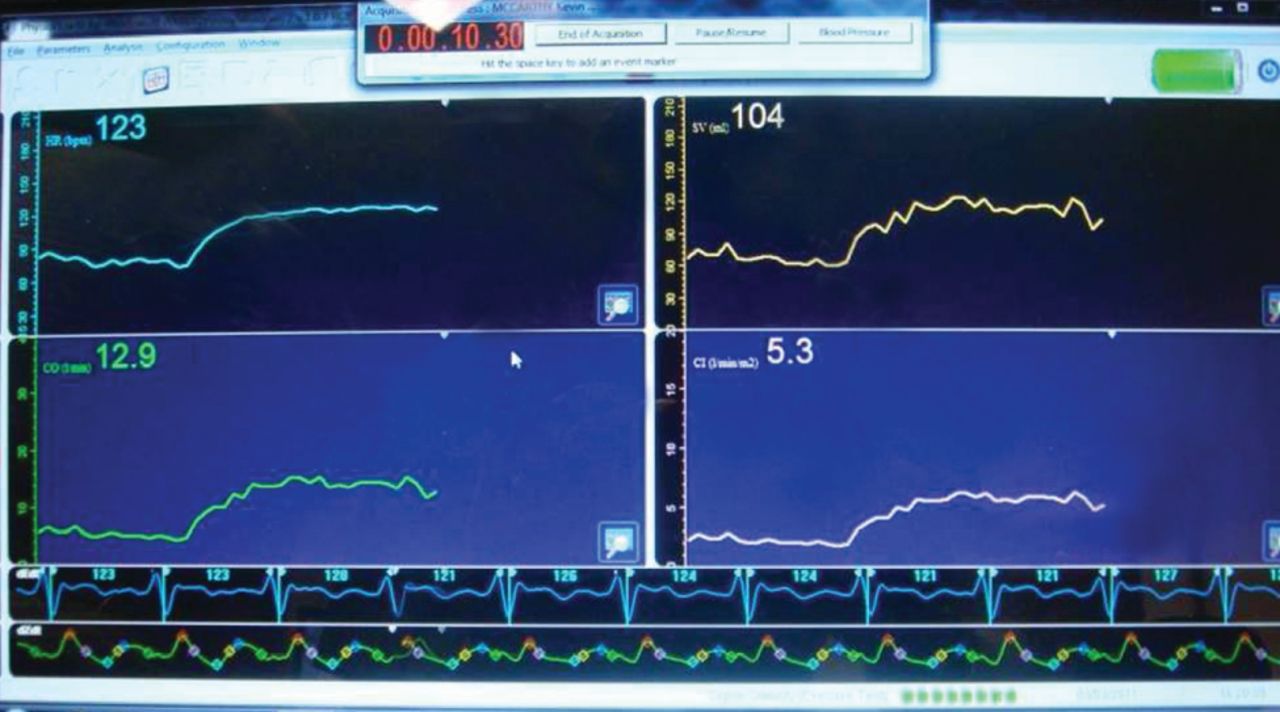
Impedance cardiography recordings from cardiopulmonary exercise test. Data include heart rate (upper left), stroke volume (upper right), cardiac output (lower left), and cardiac index (lower right). Recordings are presented as a continuous trend and as real-time digital display. Time elapsed is digitally presented in red at top, center.
The current complement of exercise-based testing modalities range from the simplest stair climb test to CPET, with its high equipment requirement and often complex interpretation strategies. Between the extremes is the 6MWT, a sub-maximal “field test” with broad applications and a still growing appreciation of its clinical value.
Given the present complement of exercise-based tests, and with the possible future addition of enhanced portable cardiopulmonary monitoring, it is important that physicians and their healthcare associates maintain a general awareness and understanding of exercise tests in common use, in order to make selections that will yield the best possible results.
Discussion
MacIntyre:
We do a lot of CPETs for our rehab population, and one of the patterns we see a lot is what we call our cardiac-limited patients. That is to say, they don't hit a ventilatory limit, they don't desaturate, but they shoot their heart rate up. We've tried to screen these people for intrinsic heart disease, and we think a lot of this is deconditioning: they have become couch potatoes. With the simple tests we do routinely, I don't know how to distinguish that from subtle heart disease. I was intrigued with your use of the V̇E/V̇CO2, which I think of as a dead space measurement, but maybe there's more to it than that. You also introduced this heart rate recovery; is there any hope of using some of these simple measurements to differentiate real heart disease from just somebody who's a couch potato?
Pichurko:
This is a common concern, as the deconditioned patient, whose cardiac output relies principally on an increase in heart rate, without a proportional increase in stroke volume (represented by O2 pulse), closely mimics the limitation due to structural cardiovascular disease. Absolutely. So I try to gather as much recorded data, including a markedly reduced ventilatory or anaerobic threshold, elevated ventilatory equivalent for carbon dioxide, that may suggest a pulmonary hypertensive response reflecting left-ventricular dysfunction, a reduced rate of heart rate normalization in recovery, electrocardiogram changes, and the like. Even with all the gathered data, the distinction may not be absolutely clear. I will often suggest that while reduced aerobic conditioning may be contributory, structural cardiovascular impairment is not excluded. We all struggle with that distinction. Thank you bringing up this important point. The question about the value of heart rate recovery is intriguing, but we haven't studied that well enough to answer the question. Dr Salzman, do you have any thoughts?
Salzman:
No, I don't have much experience with that parameter.
Pichurko:
The larger issue of distinguishing the cardiac-limited patient due to deconditioning from the one with a cardiovascular structural impairment: any insights that you wish to share?
Salzman:
One comment is the ventilatory equivalents for O2 and CO2 do seem to reflect the severity of the cardiomyopathy as well. We think of it as a dead space fraction parameter, so mostly relating to lung disease, but there's something about cardiac disease that causes abnormalities to this parameter as well. Probably dead space fraction in the cardiac patients is elevated due to poor cardiac output causing V̇/Q̇ [ventilation/perfusion] abnormalities by poor perfusion to upper lobes.
Pichurko:
Or pulmonary blood flow reductions creating an increase in physiologic dead-space.
Hnatiuk:
Neil, if I'm not mistaken, Eschenbacher1 about 20 years ago proposed an algorithm that included both of those in evaluating cardiopulmonary limitation. I don't know if it's ever been prospectively validated, but he looked at both of those in his algorithm.
Pichurko:
Both of?
Hnatiuk:
The V̇E/V̇CO2 and heart rate reserve.
Pirchurko:
Heart rate recovery?
Hnatiuk:
I believe it was “reserve,” but could have been “response.”
Pichurko:
The heart rate reserve is a comparison of peak achieved heart rate with the predicted maximum. It reflects the adequacy of the heart rate response to exercise. The heart rate recovery is in reference to the expected decline in heart rate in the first minute of rest, post-exercise. Persistent high heart rate or inadequate heart rate recovery (usually 18-24 beats/min) is a marker for cardiovascular disease.
Hnatiuk:
I obviously confused “heart rate recovery” and “heart rate response.”
Pichurko:
It has been proposed chiefly in the cardiovascular literature as an early indicator of a variety of cardiac and pulmonary vascular disorders.
Hnatiuk:
Let me ask you something: are you proposing that we stop doing oximetry on patients we do 6-minute walk tests on?
Pichurko:
Not at all. It's useful, but it's useful in a limited fashion. It is a commonly used option in the 6-minute walk test, but should not be used for titration, as it compromises the “self-paced” nature of the 6-minute walk test and, ultimately, the distance walked, which is the primary measure. It may best be measured at the start and at the end of the study. Other protocols are better suited to careful and repeated titration of a patient's O2 requirements.
Hnatiuk:
And the motion of the finger during cardiopulmonary exercise testing on a bike is still too much?
Pichurko:
Well, it remains a concern. We use a headband fitted with a forehead sensor. Other labs will use ear sensors. The more stable the better. I think the hand is least stable from the point of movement. Keep in mind the problems of reduced perfusion to the digits accompanying a tight hand grip on the bicycle. That may compound the problem of using digital sensors. Any thoughts to the contrary?
Coates:
I would only think that as exercise goes on and the heart rate goes up there would be an increased accuracy, compared to just moving the finger, because most of these devices use some mathematical way of eliminating movement noise. Masimo uses a Fourier transform that basically takes each pulse, divides it into a power spectrum, and then the most prominent members of the power spectrum are what you should have seen, and the rest is considered noise-related artifact. So the more pulses it gets per minute, the happier it should be with its signal: at least that's my way of thinking. Comparing something where you move the finger on a machine, even if you can do it very uniformly, to actually doing exercise where your heart rate is going up may not be exactly a fair comparison.
Pichurko:
The cases of the healthy subjects certainly do not reflect most of the people we measure. I do get your point, An exercise-related hemodynamic profile certainly involves an improved cardiac output. It is unclear whether that means better perfusion and a better signal to the digits. The activation of the sympatho-adrenal response accompanying exercise serves to redirect blood flow to working muscles and away from peripheral digits, et cetera. In the end, it is uncertain which will dominate in the healthy or cardiac impaired individual. Thank you for your comment.
Miller:
I'd like to take exercise testing in another direction. If one is interested in early detection and confirmation of disease, I'm thinking especially of ILD [interstitial lung disease!--005D--! where it's been said, “Well, if you really want to see whether the DLCO is impaired, you should re-check it after exercise.” So has anybody looked at diffusing capacity pre- and immediately post-CPET or the 6-minute walk test or any other standardized exercise test?
MacIntyre:
Yes, I actually did that back in my fellowship. It is a little tricky because the 10-second breath- hold doesn't work real well at high levels of exercise. Jay Nadel taught me the intra-breath technique, which is a much shorter and easier test to do, and it goes up in normal people about 20 or 30%.
Miller:
I'm aware of the intra-breath technique. We measured it1 in normal people at 6 increments during the incremental CPET, to establish normal values for increases in diffusing capacity and pulmonary blood flow. But I was thinking that when you cease exercise, during the first minute, and now you're looking at the heart rate recovery and you're measuring the blood gas, perhaps you could add DLCO. Perhaps by that time even the 10-second breath-hold would be tolerable, and it might add to the information we learn by stressing the patient.
Pichurko:
I believe that a challenging population is that composed of apparently healthy individuals who are sent for a complete PFT study and have mildly or moderately reduced DLCO and a reduced resting PO2 on arterial blood gases. I've always viewed it as a favorable sign if the PO2 and O2 saturation would improve with exercise, believing that they're recruiting lung tissue principally at the bases that is compressed and under-ventilated at rest. So I always thought the opportunity to exercise a patient would provide useful gas exchange information, but not exactly in the manner that you've asked. I have no direct information or experience with that.
Enright:
When I arrived at the Mayo Clinic about 30 years ago, Ward Fowler and Bob Hyatt had set up all of the DLCO tests to be done during a steady-state 2-step exercise. We replaced it with single-breath DLCO tests in order to improve the number of patients who could be tested each day. We failed to perform a study to demonstrate if measuring DLCO during submaximal exercise improves sensitivity for ILD.
Salzman:
One comment/question about pulse oximetry during the 6-minute walk test. It's been roughly 10 years since the ATS guideline1 was put out, and it's interesting to look back and realize that they said that pulse oximetry was optional, as I recall. And now it's become quite standard, and I think the literature over the last 10 years in ILD suggests that perhaps the degree of desaturation during exercise may be the more important prognostic information, rather than 6-minute walk distance. Does anybody in the group have comments about that?
Culver:
I think the same guideline also said the therapist wasn't supposed to be with the patient when they were walking. So, unless the patients are self-reporting or you've got an oximeter on a radio signal, you don't know what!--apos--!s going on. We're clearly not doing the tests routinely the way it was described, as we do have a respiratory therapist walking along, holding the oximeter.
Pichurko:
We use Bluetooth continuous signaling, but we don't use gas exchange as a reason for the test, and we do not interrupt or curtail the test based on the O2 saturation signal. We do report O2 saturation as an end-exercise value.
McCormack:
I have a couple basic questions for the group about the 6-minute walk test. Using predicted versus absolute values for the outcomes, you showed some data that seemed to mostly center on absolute values, but can you also comment on the role of the predicted value? Also, can you comment on test variability among patients who are already on supplemental O2: how the test is performed for those patients and whether, for example, the person administering the test walks with them and carries their device? This is not recommended but sometimes happens, even as part of a clinical trial. Finally, a slightly different issue, but can you comment on if there is any thought about whether or not there's a role for the 6-minute walk test in patients with underlying neuromuscular disease?
Enright:
I was the primary author of the 10-year-old 6-minute walk test guidelines.1 Drs Salzman and Culver and I are eager to add all of you who have just commented about deficiencies in the current guidelines to the ATS and American College of Chest Physicians Working Group, which plans to update that guideline during the next three years.
MacIntyre:
Maybe you covered this and it blew past me, but when you do pulse oximetry during a 6-minute walk test, if you put it on their finger and they carry their hands by their side, it always drops several percentage points. Has that been systematically studied?
Enright:
I've not seen it published.
MacIntyre:
But I think it's real and it's an issue.
Pichurko:
It's one of many concerns about using the digits in exercising individuals.
MacIntyre:
I agree.
Pichurko:
In part for that reason, we use the forehead, secured with a head band. Under any circumstance, it is hard to escape motion artifact and noise. So we consider the readings only as estimates, and pay particular attention to gradual trends, paying little or no attention to rapid, spiking up and down fluctuations.
MacIntyre:
But a lot of people get qualified for O2 based on a 6-minute walk test, and if you've got the pulse oximeter hanging down below their waist, you can see a drop of a couple of points and take somebody who doesn't need O2 and all of a sudden they're qualified.
Pichurko:
I find oximeter recordings to represent errors in either direction. Overestimates by pulse oximetry of true arterial O2 saturations are well described, sometimes but not always related to elevated carboxyhemoglobin. However, we see underestimates as well, based on comparison with concurrent ABG [arterial blood gas] and measured O2 saturations. I view exercise-related blood gases as a standard for gas exchange, and we incorporate that into our CPET.
Salzman:
You were saying that you don't actually look at the pulse oximetry data during the 6-minute walk test and terminate a test based on desaturation.
Pichurko:
Correct. That is also the common, even published practice. In a 6-minute walk test sub-study1 in IPF, the investigators would have a practice session during which they would do titration and patients would exercise at that level of O2 support that maintained the O2 saturation level above a level of 83%. The investigators would have them back on another day for the 6-minute walk test, which proceeded without interruption. If you made O2 titration the priority, to be incorporated in the protocol, you would unavoidably compromise the distance walked, the primary end point of the 6-minute walk test as presently conceived.
Footnotes
- Correspondence: Bohdan M Pichurko MD, Pulmonary, Allergy, and Critical Care Medicine, Cleveland Clinic, Mail Code A90, 9500 Euclid Avenue, Cleveland OH 44195. E-mail: pichurb{at}ccf.org.
-
Dr Pichurko presented a version of this paper at the 48th Respiratory Care Journal Conference, “Pulmonary Function Testing,” held March 25–27, 2011, in Tampa, Florida.
-
Dr Pichurko has disclosed a relationship with NeuMedDx.
- Copyright © 2010 by Daedalus Enterprises Inc.
References





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Pulmonary Function Tests: The Current State
- Exercise Tests: The Theory
- Exercise Tests: The Methods
- Pulse Oximetry: Its Role in Exercise Testing
- What Is Post-Exercise Heart Rate Recovery?
- Referring the Patient for Exercise Testing: 6MWT Versus CPET
- Exercising Your Patient: A Look to the Future
- Discussion
- Footnotes
- References
- Figures & Data
- Info & Metrics
- References