

Abstract
BACKGROUND: Conventional chest physical therapy (CCPT), applied by therapists using cupped hands to perform percussion, is commonly used in hospitalized adults. However, increased work load demands and occupational health concerns (eg, carpal tunnel syndrome) limit the overall utilization of this therapy. Therefore, we conducted a study to compare the overall effectiveness of CCPT to high-frequency chest wall compressions (HFCWC) applied via a vibratory vest.
METHODS: A single-center, randomized trial among hospitalized intubated and non-intubated adult patients requiring chest physical therapy comparing CCPT and HFCWC. The primary outcome measure was hospital stay.
RESULTS: A total of 280 per-protocol patients (out of an a priori estimated 320 patients required to demonstrate a 20% relative reduction in hospital stay) were randomly assigned to receive CCPT (no. = 146, 52.1%) or HFCWC (no. = 134, 47.9%). The hospital stay was 12.5 ± 8.8 days for patients randomized to CCPT and 13.0 ± 8.9 days for patients randomized to HFCWC (P = .62). Patient comfort was assessed using a visual analog scale (increasing score reflects greater discomfort) and was statistically greater for patients randomized to CCPT compared to HFCWC (2.2 ± 0.8 vs 1.9 ± 0.8, P = .009). The duration of time until radiographic resolution of lobar atelectasis trended less for CCPT compared to HFCWC (5.2 ± 4.3 d vs 6.5 ± 5.2 d, P = .051). All other secondary outcomes, including hospital mortality and nosocomial pneumonia, were similar for both treatment groups.
CONCLUSIONS: This study was inadequately powered for the primary outcome of interest and hence we cannot make recommendations on the preferential use of HFCWC or CCPT for intubated and non-intubated adult patients. HFCWC was associated with statistically better comfort scores. (ClinicalTrials.gov registration NCT00717873.)
Introduction
Conventional chest physical therapy (CCPT) is a technique employed by healthcare providers to assist patients in clearing secretions from their airways. This technique requires a trained practitioner to position patients correctly and to vibrate the thorax using a clapping technique of the hands to facilitate secretion mobilization.1 CCPT has been associated with various complications, including hypoxemia, arrhythmias, and increased intracranial hypertension, as well as carpal tunnel syndrome for the therapists or nurses providing the treatments.2–4 The available clinical evidence does not support the routine use of chest physical therapy for common conditions, including pneumonia, the postoperative state, and respiratory failure requiring mechanical ventilation.5–7 Chest physical therapy may be of benefit in specific clinical circumstances, including patients with lobar atelectasis, bronchiectasis, and patients with impaired ability to clear secretions due to neuromuscular deficits, although recommendations for the use of chest physical therapy are limited due to the absence of well-designed long-term trials.7–10
Current estimates are that the number of patients requiring hospitalization for acute care is rising and will continue to rise for the foreseeable future.11,12 This will likely increase the need for supportive medical therapies to include chest physical therapy. High-frequency chest wall compressions (HFCWC) applied via a vibratory vest is a mechanical approach for providing chest physical therapy as an alternative to CCPT. Potential advantages of HFCWC include standardizing chest physical therapy regimens and eliminating the need for manually administered treatments.13 Therefore, we conducted the current study to compare the overall effectiveness of HFCWC to CCPT among hospitalized adult patients ordered to receive chest physical therapy by their treating physicians.
QUICK LOOK
Current knowledge
Chest physical therapy is used to promote secretion clearance in mechanically ventilated patients. Both manual percussion and high-frequency chest wall compressions via an automated vest system are used, but no evidence supports the superiority of either technique.
What this paper contributes to our knowledge
High-frequency chest wall compressions was associated with better comfort, compared to manual percussion. There was no difference in measurable clinical outcomes such as length of stay, resolution of atelectasis, or incidence of nosocomial pneumonia.
Methods
From July 2008 to December 2010, patients were recruited from Barnes-Jewish Hospital for study participation. Washington University's institutional review board approved the study protocol, including written, informed consent, prior to enrolling any patients. The trial was registered with ClinicalTrials.gov on July 1, 2008, (NCT00717873) to comply with National Institutes of Health requirements. All patient screening was performed daily by the investigators.
Patients were enrolled in the study if they were 18 years of age or older, had an acute or chronic pulmonary condition requiring secretion mobilization as per hospital protocol,14 and had a physician's order for chest physical therapy. The protocol-approved indications for CCPT at Barnes-Jewish Hospital include lobar atelectasis and bronchiectasis, as well as cystic fibrosis.4,8 All other non-approved indication requests for CCPT required approval by the medical director of the Department of Respiratory Care Services. Patients were excluded from the study if they had absolute contraindications for postural changes or chest percussion, were pregnant, received prior HFCWC or CCPT during the current hospitalization, were hospitalized for more than 15 days, were previously enrolled in the study, or the patient's primary attending physician refused participation. Immediately after enrollment, patients were randomized to CCPT or HFCWC. Patients receiving at least one treatment, CCPT or HFCWC, a priori were included in the per-protocol analysis.
The following adverse events associated with chest physical therapy, both CCPT and HFCWC, during the study period were screened for: hypoxemia (arterial oxygen saturation less than 90% during treatment); arrhythmias (any arrhythmia resulting in a heart rate < 60 or > 120 beats/min); increased intracranial pressure (> 15 mm Hg); hemodynamic instability (systolic blood pressure < 100 or > 180 mm Hg); pulmonary hemorrhage; emesis; witnessed aspiration; or bronchospasm. Additionally, other adverse events felt to be related to the administration of either CCPT or HFCWC could be recorded by the respiratory therapist administering the treatments. All patients receiving HFCWC or CCPT had continuous monitoring of oxygen saturation and heart rhythm. Frequency of blood pressure measurements was assessed per the hospital ward or intensive care unit policy. Patient comfort during chest physical therapy was assessed with a visual analog scale, using a written script delivered by one of the investigators (KS, PW) who were unblinded to the intervention, to elicit the patient's comfort response as follows: 1 = comfortable with therapy; 2 = uncomfortable with therapy, but able to tolerate therapy; 3 = some pain, more uncomfortable, but will continue therapy; 4 = significant pain, but can tolerate therapy; 5 = intolerable pain. Patient comfort was assessed immediately following every treatment, either CCPT or HFCWC, and the average of the comfort scores was reported.
The primary outcome variable was hospital stay. Secondary outcomes assessed included intensive care unit stay, duration of mechanical ventilation, time to resolution of lobar atelectasis when present, occurrence of nosocomial pneumonia, and hospital mortality. Nosocomial pneumonia was defined as the presence of a new or progressive pulmonary infiltrate and 2 of: temperature > 38.3°C or < 36.0°C; leukocyte count > 12,000/mL or < 4,000/mL; purulent tracheal secretions in the absence of other infections requiring antimicrobial treatment. Severity of illness was assessed with the Acute Physiology and Chronic Health Evaluation (APACHE) II score.15 Adverse events and deaths were reviewed by members of a data safety monitoring board and reported to Washington University's institutional review board.
CCPT was performed by a respiratory therapist up to 4 times daily, immediately after patients had received their prescribed bronchodilator therapy. Patients received manual clapping over the chest wall, with the patient positioned so that gravity could aid mucus drainage from the lobes or segments being percussed.1 Postural drainage with percussion and vibration was performed for 2 min in each of 8 standard positions for patients with cystic fibrosis/bronchiectasis. For patients with lobar atelectasis, patients were placed in a position favoring drainage of secretions from the obstructed lobe for 4 min during percussion and vibration. This was repeated as tolerated by the patient. Following percussion and vibration in each position, patients took deep breaths, coughed, and expectorated. Sessions lasted 15–20 min.
HFCWC was also performed up to 4 times daily, using The Vest Airway Clearance System Model 205 (Hill-Rom, St Paul, Minnesota) immediately after patients had received their prescribed bronchodilator therapy. Each patient was fitted with either a Wrap or Full-Torso vest connected to the air pulse generator via 2 flexible tubes. Patients remained in an upright sitting position throughout the 15–30 min treatment session. HFCWC was applied for no longer than 15 min at a time, at a frequency of 10–15 Hz, followed by a 5 min rest period. The frequency and pulse pressure were set according to individual patient's reported comfort. During both the HFCWC and rest periods, patients were instructed to huff or cough as they felt necessary in order to expectorate loosened bronchial secretions. The total duration of CCPT and HFCWC, from the time it was initially ordered, was determined by the treating respiratory therapists according to hospital guidelines.14 For patients with atelectasis, therapy was discontinued when the atelectasis resolved radiographically. For patients with cystic fibrosis/bronchiectasis, therapy was stopped when patients no longer tolerated the therapy or clinical improvement warranted discontinuation of the therapy.
Concealed randomization was conducted using a blocked randomization schedule. A priori, the number of patients with cystic fibrosis was capped at no more than 25% of the total number of patients enrolled. Based on previous local data,14 the predicted stay for hospitalized patients receiving chest physical therapy was estimated to be 6.0 ± 3.0 days. The trial was designed to enroll 320 patients, to demonstrate a 20% relative reduction in hospital stay, from a mean of 6 days to a mean of 5 days, with an α level of .05 and a power level of 80%. Values are reported as mean ± SD or median and interquartile range. Comparisons between groups (CCPT vs HFCWC) were conducted using the chi-square test, Fisher exact test, 2-tailed t test, and the Wilcoxon signed rank test. Kaplan-Meier curves were compared using the log-rank test. Analyses were conducted with SPSS, version 11.0 for Windows (SPSS, Chicago, Illinois).
Results
Study Population and Assigned Treatment
Between July 2008 and December 2010, a total of 1,050 patients were screened for eligibility; 296 were considered to be eligible for inclusion in the study and were randomly assigned to receive either CCPT (no. = 148) or HFCWC (no. = 148) (Fig. 1). A total of 146 of the 148 patients assigned to CCPT and 134 of the 148 patients assigned to HFCWC were included in the per-protocol analysis. Seven (4.7%) patients in the HFCWC group were withdrawn from the study after being unable to be fitted with the vibratory vest; an additional 5 (3.4%) patients with cystic fibrosis assigned to the HFCWC group were withdrawn because their attending pulmonary physicians preferred that the patient receive CCPT. The baseline demographic and clinical characteristics were similar between the 2 per-protocol groups (Table 1). There were more patients with cystic fibrosis/bronchiectasis and lobar atelectasis in the CCPT group and more patients requiring secretion mobilization in the HFCWC group; otherwise the groups were well matched.

Study enrollment, randomization, and assessment. CPT = chest physical therapy. CCPT = conventional chest physical therapy. HFCWC = high-frequency chest-wall compressions.
Characteristics of the Per-Protocol Study Population
There were 4,453 chest physical therapy treatments administered as part of the study; 2,016 treatments (13.8 ± 13.6 treatments per patient) in the CCPT group and 2,437 treatments (18.2 ± 16.5 treatments per patient) in the HFCWC group (P = .02). Overall, there were 62 (42.5%) patients in the CCPT group and 37 (27.6%) patients in the HFCWC group who received less than 8 chest physical therapy treatments respectively (P = .009).
Outcomes
The hospital stay was similar for patients receiving CCPT (median 10 d, 25th and 75th percentiles 5 and 18 d) and HFCWC (median 10 d, 25th and 75th percentiles 6 and 19 d) (Table 2, Fig. 2). The intensive care unit stay and duration of mechanical ventilation were also similar in both treatment groups. No episodes of nosocomial pneumonia were observed in any of the study patients during the investigation period. Resolution of lobar atelectasis during treatment was also similar between treatment groups (see Table 2). The duration of time until radiographic resolution of lobar atelectasis was also similar between HFCWC and CCPT (6.5 ± 5.2 d vs 5.2 ± 4.3 d, P = .051). Patients receiving HFCWC and CCPT had similar 30-day mortality (6.7% vs 2.7%, P = .16). Kaplan-Meier plots of the probability of remaining alive are shown in Figure 3. Patients receiving HFCWC had similar probability of 30-day survival, compared to patients receiving CCPT (P = .14 by the log rank test). Patient comfort scores (increasing score indicates greater discomfort) were statistically greater for patients randomized to CCPT, compared to HFCWC (2.2 ± 0.8 vs 1.9 ± 0.8, P = .009) (Fig. 4). The outcomes for the subgroups with cystic fibrosis/bronchiectasis and lobar atelectasis were also similar for the 2 treatment groups (see Table 2). Patient comfort scores were greater for patients receiving CCPT in both subgroups, but failed to reach statistical significance.
Clinical Outcomes

Bar graphs depicting hospital stay for patients receiving conventional chest physical therapy (CCPT) and patients receiving high-frequency chest-wall compression (HFCWC). The lines within the boxes represent the 50th percentile, the lines at the bottom and top of the boxes represent the 25th and 75th percentiles, and the whiskers lines represent the 5th and 95th percentiles.
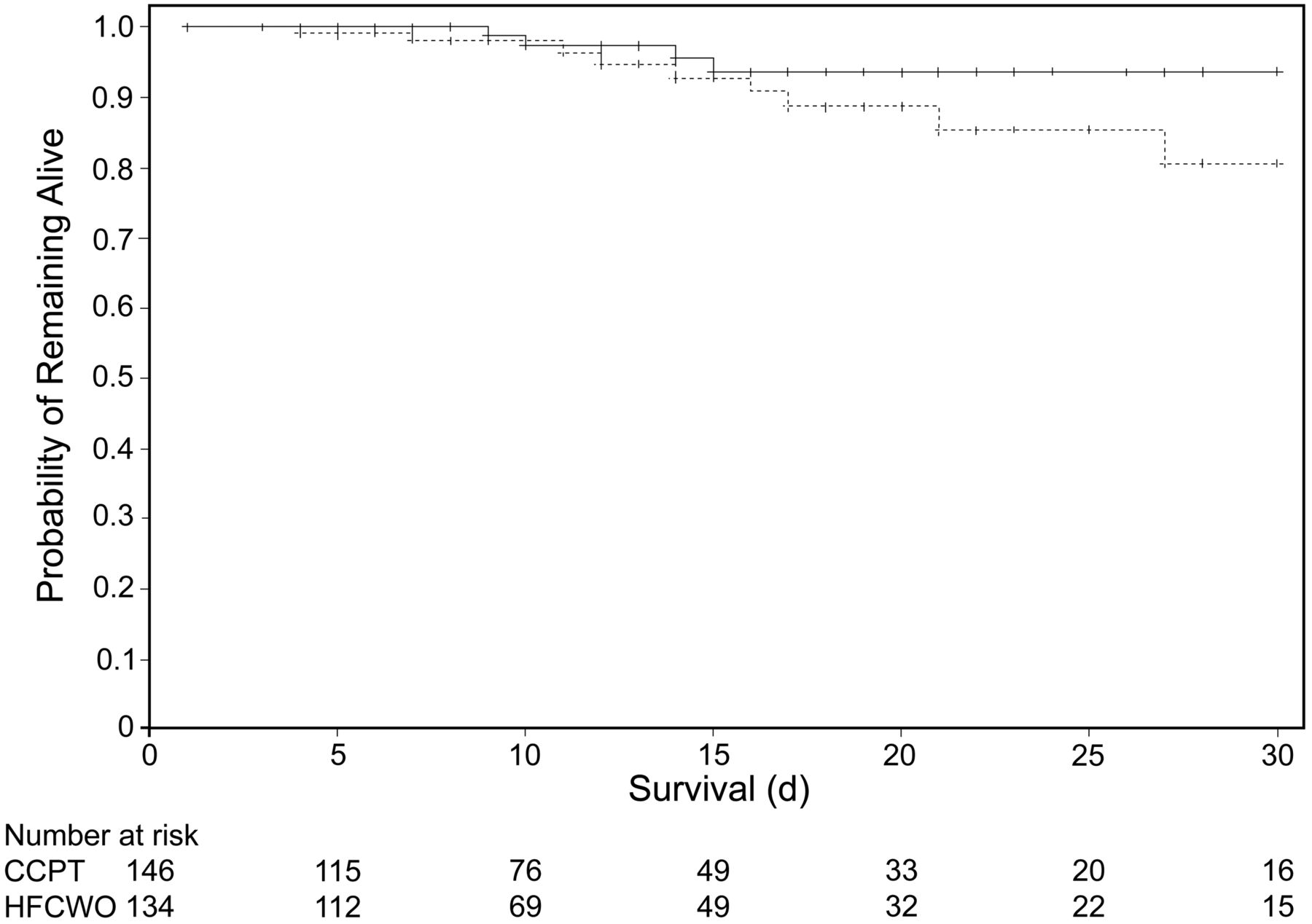
Kaplan-Meier curves depicting the probability of survival from study enrollment in patients receiving conventional chest physical therapy (CCPT) (solid line) and patients receiving high-frequency chest-wall compressions (HFCWCs) (dashed line) (P = .14 by log rank test).HFCWC

Bar graphs depicting comfort scores for patients receiving conventional chest physical therapy (CCPT) and patients receiving high-frequency chest-wall compressions (HFCWC). The dashed line represents the 50th percentile, the lines at the bottom and top of the boxes represent the 25th and 75th percentiles, and the whiskers lines represent the 5th and 95th percentiles.
All 13 hospital nonsurvivors were reviewed by the data safety monitoring board. In none of these patients was the cause of death attributed to a complication or failure of CCPT or HFCWC. There were 9 (6.2%) adverse events in the CCPT group attributed to the treatment (1 patient with increased secretions unable to be expectorated, 8 with intolerable pain/discomfort) and 9 (6.7%) in the HFCWC group attributed to the treatment (1 patient with nausea, 8 with intolerable pain/discomfort).
Discussion
This single-center comparative-effectiveness study, although underpowered for the primary outcome, suggests that CCPT and HFCWC may be equivalent in terms of their effects on patient outcomes. Patient-reported comfort during chest physical therapy was statistically greater for patients receiving HFCWC, compared to CCPT. The number and type of adverse events were similar for the 2 modes of chest physical therapy. However, not all patients assigned to receive HFCWC could be adequately fitted with a vest and there were statistically more treatments administered among patients in the HFCWC group.
A Cochrane review evaluating the role of chest physical therapy in patients with cystic fibrosis found that airway clearance techniques have short-term effects in terms of increasing mucus transport.16 However, there was no evidence that these techniques resulted in any long-term benefits. In a recent Cochrane review assessing the efficacy of chest physical therapy for treating pneumonia in hospitalized adults, chest physical therapy could not be recommended as routine adjunctive treatment.5 Although the numbers of patients evaluated were small, osteopathic manipulative treatment (vs placebo) and positive expiratory pressure (vs no physiotherapy) reduced mean duration of hospital stay by 2.0 days (95% CI −3.5 to −0.6) and 1.4 days (95% CI −2.8 to −0.0), respectively.5
A recent randomized trial of 180 adult patients requiring mechanical ventilation for more than 48 hours evaluated the efficacy of chest physical therapy versus placebo.17 The primary end point was initial time to become ventilator-free. Kaplan-Meier analysis censored for death revealed a significant prolongation of median time to become ventilator-free among patients receiving chest physical therapy (P = .047). The time taken for 50% of patients (median time) to become ventilator-free was 15 and 11 days, respectively, for chest physical therapy and control groups. Routine use of chest physical therapy is not generally recommended as adjunctive treatment for pneumonia, abdominal surgery, or respiratory failure in adults.5–7 However, in a small study ventilator-associated pneumonia occurred in 39% (14/36) of the control group and 8% (2/24) of patients receiving chest physical therapy (odds ratio = 0.14, 95% CI 0.03–0.56, P = .02) without any influence on mortality or stay.18 Routine use of chest physical therapy also appears to be inferior to intermittent positive-pressure ventilation and walking programs for hospitalized adults with COPD.19
Another major issue with chest physical therapy is the various techniques available for administering this therapy, with a lack of robust comparative data. One prospective randomized trial of long-term chest physical therapy modalities included 166 individuals with cystic fibrosis and reported that overall satisfaction was higher with the use of HFCWC and a flutter device, compared to CCPT.20 Overall declines in lung function (FEV1 and FVC) appeared to be similar for the 3 modalities studied, and study drop-out was greatest for those receiving CCPT (51%), compared to a flutter device (26%) and HFCWC (9%). However, the annual forced expiratory flow during the middle half of the forced vital capacity maneuver (FEF25–75%) rate of decline was greater in those using HFCWC (P = .02). This study differed from our trial in evaluating 3 different chest physical therapy techniques over a long-term period, up to 2.8 years, and primarily on an out-patient basis.
A more recent study of 29 hospitalized patients with cystic fibrosis compared HFCWC with CCPT.21 No statistically significant change in pulmonary function testing or oxygen saturation was observed after either HFCWC or CCPT compared with baseline. No significant differences were observed in comfort scores or urinary leakage between HFCWC and CCPT. However, of those patients who completed the study, 17 (55%) expressed a preference for their usual CCPT over HFCWC. Significantly more sputum was expectorated during a single treatment session and over a 24-hour period (mean difference 4.4 g and 6.9 g, respectively) with CCPT than with HFCWC (P < .001), which may explain the trend to more rapid resolution of acute lobar atelectasis with CCPT we observed in the current trial. The paucity of comparative studies of airway clearance techniques has led to a call for appropriately designed trials of adequate size using new alternative outcomes, including patients' preferences, so that more informed treatment decisions can be made.22
An unexpected finding from our study was that there were significantly more chest physical therapy treatments administered in the HFCWC group, compared to the CCPT group, despite using the same protocol criteria for the discontinuation of chest physical therapy. Our study did not allow us to capture the reasons for this difference. One possibility is that HFCWC was not as effective as CCPT and thus required that more individual HFCWC treatments be administered. This seems unlikely given the similar outcomes associated with both CCPT and HFCWC. Another possibility is that patient comfort may have played a role. The greater comfort level associated with HFCWC may have allowed more HFCWC treatments to be administered, compared to CCPT. Another potential explanation for this observation is that therapists developed a preference for HFCWC and were more inclined to continue its use.
Some strengths of the present trial include the relatively large sample size, the use of a well-defined outcome, as well as precise secondary outcome measures, careful assessment of adverse events associated with each treatment, and the inclusion of a patient comfort score to directly measure the acceptability of the treatment from the patient's perspective. Several potential limitations of our trial should be noted. First, it was performed at a single center, limiting the generalizability of the results, and we used a heterogeneous patient population. The latter may have limited our ability to detect differences in outcomes between the 2 forms of chest physical therapy in more specific patient subpopulations (cystic fibrosis, postoperative patients, COPD, lobar atelectasis). Second, the evidence in support of CCPT is limited, as noted above. It is important to note that the majority of the indications for CCPT at our hospital are lobar atelectasis and cystic fibrosis (see Tables 1 and 2). Future studies are needed to determine the benefits of CCPT or HFCWC compared to standard airway care (humidification and suctioning) for these indications, as well as any other indications where they are currently being employed. Third, we focused on hard end points like hospital stay. Therefore, we did not determine the influence of CCPT and HFCWC on the resolution of the clinical problems they were ordered for with the exception of lobar atelectasis, where we saw a trend in favor of CCPT.
Another limitation of our study is that we underestimated the duration of hospitalization among patients requiring chest physical therapy. This probably occurred as we used estimates for hospital stay that were almost 10 years old at the inception of our trial.14 Additionally, we recruited only 280 out of a required 320 patients in our per-protocol group, due to the length of the study and lack of funding. Therefore, this trial is underpowered to assess the primary outcome measure of hospital stay. This may also have limited our ability to detect other important differences between the study groups, due to underestimation of the needed sample size. The fact that 42.5% of the patients in the CCPT arm and 27.6% of the patients in the HFCWC arm received less than 8 treatments, despite having indications for the treatments, also limits our ability to discern differences between these 2 modalities. Similarly, our study was not powered to investigate the effects of these therapies on mortality. The investigators obtaining the comfort scores following the administered treatments were also not blinded to patients' treatment group assignment. This may have resulted in assessment bias accounting for the differences in the scores we observed between the treatment groups. However, as previously noted, we employed a standardized script for assessment of the comfort scores regardless of treatment group assignment, which should have minimized the potential for such bias. Finally, the greater number of treatments in the HFCWC group suggests a potential bias on the part of the staff and/or investigators favoring this treatment modality.
Conclusions
In summary, we demonstrated that among hospitalized adults with a physician's order for chest physical therapy, the use of HFCWC and CCPT yielded similar outcomes except that HFCWC was associated with statistically better comfort scores and a greater number of administered therapies, while CCPT was associated with a trend toward more rapid resolution of lobar atelectasis. These data suggest that HFCWC may be used as a substitute for CCPT with overall equivalent effectiveness and patient comfort in hospitalized adults requiring assistance with airway clearance. However, the use of both HFCWC and CCPT should be carefully monitored so that treatments are not administered when they are not indicated. Most importantly, additional clinical trials are needed to evaluate the overall effectiveness of chest physical therapy in intubated and non-intubated adults. Such trials should include a control group receiving humidification and airway suctioning alone to help address this important question.
Footnotes
- Correspondence: Marin H Kollef MD, Division of Pulmonary and Critical Care Medicine, Washington University School of Medicine, 660 South Euclid Avenue, Campus Box 8052, St Louis MO 63110. E-mail: mkollef{at}dom.wustl.edu.
Dr Kollef's efforts were supported by the Barnes-Jewish Hospital Foundation. The authors disclose that they received an unrestricted grant from Hill-Rom to conduct this study. Hill-Rom reviewed the final study protocol but did not have any role in the study's design. The authors have disclosed no other conflicts of interest.
See the Related Editorial on Page 323
- © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}