

Abstract
BACKGROUND: Head of bed elevation ≥ 30° reduces ventilator-associated pneumonia in mechanically ventilated patients, but adherence is variable and difficult to monitor continuously. Unlike many clinical variables, head of bed elevation is not electronically displayed or monitored with audible alarms. HYPOTHESIS: Continuous monitoring of head of bed elevation with audible alerts and visual cues when the elevation is < 30° will improve adherence by 15%.
METHODS: Head of bed elevation was continuously monitored and recorded on a central monitoring station and displayed on the bedside monitor of 16 of 24 medical intensive care unit beds. Manual bedside checks were performed twice daily at varying times.
RESULTS: Continuous head of bed angle was available from 98 of 313 (31%) patient beds over a 7.5 month period, representing 322 of 1,373 mechanical ventilator days (24%). Continuous monitoring was performed for 7,720 hours, 5,542 hours with the data displayed on bedside monitors and 2,178 hours with the data available only from central monitors. Head of bed elevation was ≥ 30° for 76% of the hours when the data were displayed on bedside monitors, and for 61% of hours when it was not (P < .001, odds ratio = 2.3, 95% CI 2.0–2.6). Intermittent bedside checks for head of bed elevation ≥ 30° found 97 ± 2% adherence.
CONCLUSIONS: Real-time monitoring of head of bed elevation is feasible, and when combined with audible alarms and visual cues, improves ≥ 30° elevation adherence. Intermittent bedside checks over-estimate actual adherence.
Introduction
Ventilator-associated pneumonia (VAP) is a costly and preventable complication of patients receiving mechanical ventilation, and is a leading cause of mortality and morbidity in the intensive care unit (ICU).1–4 Consensus recommendations endorsed by the Centers for Disease Control,5 the Joint Commission,6 and the Institute for Health Improvement7 have identified a variety of strategies to reduce or prevent VAP, including meticulous hand hygiene, maintenance of adequate endotracheal tube cuff pressures, daily sedation vacation and spontaneous breathing trials, thorough oral care with the use of chlorhexidine, and keeping the head of the bed elevated ≥ 30°.3 Although head of bed elevation (HOBE) appears to be a simple intervention associated with reducing micro-aspiration of gastric contents8 and VAP,9,10 adherence is often difficult to achieve.11–15
Adherence to HOBE standards for VAP prevention has been reported as suboptimal. Recently published prospective quality improvement efforts for VAP prevention identified baseline pre-intervention adherence rates of between 5% and 50%.16,17 Notably, adherence rates improve significantly with multi-faceted quality improvement initiatives.17,18
Low adherence rates persist, despite the ready availability of ICU beds that include a simple monitor of HOBE angle visible on the side of the bed (Fig. 1A and 1B), which could be used for intermittent adherence assessment. Further, low adherence to the HOBE standard, when determined by intermittent surveillance, raises the likelihood that continuous adherence to HOBE ≥ 30° is even lower over a 24-hour period as a result of patient condition or care interventions (eg, hemodynamic instability, bathing). To establish continuous adherence to the HOBE ≥ 30° standard and to evaluate disparities between intermittent and continuous monitoring, we developed and installed devices that would electronically monitor the HOBE with a visual bedside electronic tracing of head of bed angle, and generate an alarm whenever the angle was < 28°. The purpose of this study was to evaluate the utility of this device. Our hypothesis was that continuous visual monitoring when combined with audible alarms and visual cues would improve HOBE adherence by 15%.

A and B: Head of bed elevation (HOBE) angle indicators. C: HOBE angle, measured by automated device, displayed on the bedside monitor.
QUICK LOOK
Current knowledge
Head of bed elevation ≥ 30° is associated with a reduction in the incidence of ventilator-associated pneumonia in mechanically ventilated patients; however, adherence is variable and difficult to monitor continuously.
What this paper contributes to our knowledge
Real-time monitoring of head of bed elevation is easily accomplished, and, when combined with audible alarms and visual cues, improves > 30° elevation adherence. Intermittent bedside checks by clinical staff over-estimate actual adherence.
Methods
We conducted a prospective cohort study of real-time digitally alarmed HOBE monitoring that was approved by the Colorado Multiple Institutional Review Board with waiver of consent.
Environment
The study was conducted in the 24 bed medical ICU (MICU) at Denver Health, a 477 bed acute care university-affiliated public safety net hospital. To establish adherence to VAP bundle components (see the table in the supplementary materials at http://www.rcjournal.com), adherence rates were monitored daily, prior to and during the intervention period. Since this was not a study of patient outcomes, comparisons by clinical condition, including patient demographics, were not recorded.
Study Device and Monitoring
Continuous measurement of HOBE was performed using a sealed water column in non-distensible intravenous tubing connected to a standard electro-mechanical pressure transducer mounted under all beds (see Fig. 1 in the supplementary materials at http://www.rcjournal.com). The HOBE angle was displayed as a continuous linear time trend and instantaneous numerical value on the bedside monitor (Fig. 1C and Fig. 3 in the supplementary material at http://www.rcjournal.com). Calibration of the HOBE monitor was performed to determine accuracy using a spirit-level protractor set between 10° and 40°, and precision determined by correlation between device-measured HOBE versus bed-indicated HOBE angle (see Fig. 1A and B) at 30° on 8 individual beds. Calibration was within 1% of gold-standard for both accuracy and precision. Additional descriptions of the device, including calibration details, are included in the supplementary materials at http://www.rcjournal.com.
Study Procedures
Real-time HOBE tracings with alarm limits set to activate when HOBE was < 28° were visible (V) on the bedside monitor of 16 of 24 randomly selected beds, and not visible (NV) on the remaining 8. We randomized ICU beds (not individual patients) to be visibly monitored or concealed, and documented the number of hours the HOBE was < 30° in each group. A pre-assigned block randomization table based on room numbers was used to determine which monitored beds would have the HOBE visibly displayed or concealed. The assigned block of monitored beds was rotated every month, according to the randomization table.
The HOBE device was introduced into clinical care during a 3 month run-in period during which clinical ICU staff received formal education and orientation regarding maintenance and use of the device. Nursing documentation of HOBE angle derived from bedside angle indicator had been an existing unit standard for all mechanically ventilated patients for at least 3 years prior to the study period and was continued through all phases of the study. During the run-in period, nurses and respiratory therapists were provided with general information regarding the purpose of the study to test feasibility and reliability of the real-time HOBE device to measure the position of the head of bed. However, to minimize potential Hawthorne effect, bedside providers were not aware of the intention to compare HOBE adherence to the new device versus intermittent checks.
HOBE data were collected continuously on all patient beds. A sign was placed on the bedside monitor of all visibly monitored beds as a reminder to keep the HOBE at ≥ 30° (see Fig. 1C). Alarm activation state was randomly checked on the visibly monitored beds. All beds were electronically monitored at the central nursing station for data acquisition and analysis purposes (see Fig. 3 in the supplementary materials at http://www.rcjournal.com) Bedside alarms, but not nursing station alarms, were used to alert staff if HOBE was < 30°. Computerized orders were entered for HOBE to be at least 30° from the horizontal. For the purposes of this report we analyzed HOBE adherence for periods in which beds were allocated to patients requiring mechanical ventilation only.
All data were entered on an Excel spread sheet (Microsoft, Redmond, Washington) for analysis. The amount of time that data were not collected due to device failure, non-monitored beds, and daily results of a verification check that the head of bed monitor alarm was properly functioning was also recorded. Adherence was defined as the percent of time that the HOBE was ≥ 30°.
We reviewed chart records of patient care activities on a daily basis to reconcile HOBE ≥ 30° adherence and correlated pre-specified contraindications to HOBE or patient care events (Table 1) by time with recorded HOBE. HOBE adherence was not included in the analysis for periods when there was a recorded contraindication or if mechanical ventilation duration was shorter than 24 hours.
Pre-specified Patient Care Events Interrupting Continuous HOBE Monitoring
Scheduled HOBE “point-in-time” adherence checks were performed twice daily by trained unit staff as part of usual care quality monitoring between 10:00–12:00 and 22:00–24:00, using the bed elevation angle device located on the side of each bed (see Fig. 1A and 1B).
Statistical Methods.
The primary outcome variable was number of hours HOBE ≥ 30° in V versus NV. A power analysis was performed to estimate the number of monitored “bed-hours” required to detect a 2-tailed 15% difference in HOBE ≥ 30° between V and NV beds. To account for repeated measures, type I error probability (alpha) was set at .01. To achieve 90% statistical power we estimated needing to monitor 993 hours of NV (8 beds) and 1,987 hours of V (16 beds) HOBE. Data are presented as mean ± SD, median and IQR, counts, or percentages. Outcomes were compared with the McNemar test, paired t tests, and the Wilcoxon rank sum test, as appropriate, based on the variable's distribution. Chi-square analyses and repeated-measures analysis of variance F tests were used to compare HOBE time between groups, using JMP 8 software (SAS Institute, Cary, North Carolina).
Results
After the run-in period of 3 months, HOBE adherence was prospectively monitored from May 15, 2007, through December 31, 2007. During this period 313 patients were ventilated, for a total of 1,373 ventilator days. Ninety-eight of these patients were monitored with the HOBE device, for a total of 322 ventilator days (23.5% of total ventilator days). Sixty-nine percent of episodes were excluded from analysis, mainly if a ventilation period was < 24 hours (eg, post-procedure or acute alcohol intoxication or if prolonged inadvertent device disconnection occurred, usually over a weekend when study personnel where not physically present). Of the 7,720 monitored hours, 5,542 hours were in beds that continuously displayed the HOBE and provided an alarm whenever the HOBE fell below 28°, and 2,178 hours were in beds that did not have in-room displays.
Patients with in-room displays and alarms were adherent to HOBE ≥ 30° 76% of the total hours monitored. Those without in-room displays were adherent for 61% of the hours monitored (P < .001, Table 2). The odds of patients with HOBE-V having HOBE > 30° was 2.3 (95% CI 2.0–2.6) over the study period.
HOBE Monitoring Period Characteristics*
Data were not available 9.3% of the time (520 h) in HOBE-V and 11.6% of the time (254 h) in HOBV-NV (P = .03). Major reasons for absent data were missed collection (55%) and mechanical disconnection (36%). No reason was identified for 9% of monitored time. Reasons for absent data did not differ significantly between V and NV. When all monitored episodes were analyzed, including those with missing data, the odds ratio favoring HOBE-V was 2.0 (95% CI 1.8–2.2, P < .001).
Point in time adherence checks of HOBE were completed on 92% and 98% of day and night shifts, respectively. Adherence by intermittent check with HOBE ≥ 30° was consistently higher each month of the intervention period for all day shifts (99.1 ± 0.64%), compared with night shifts (94.1 ± 1.89%, P = .02, Fig. 2). Intermittent in-room visual checks of HOBE consistently over-estimated HOBE ≥ 30° adherence (intermittent 96.6 ± 0.73%, continuous adherence 71.9 ± 1.2%, P < .001).
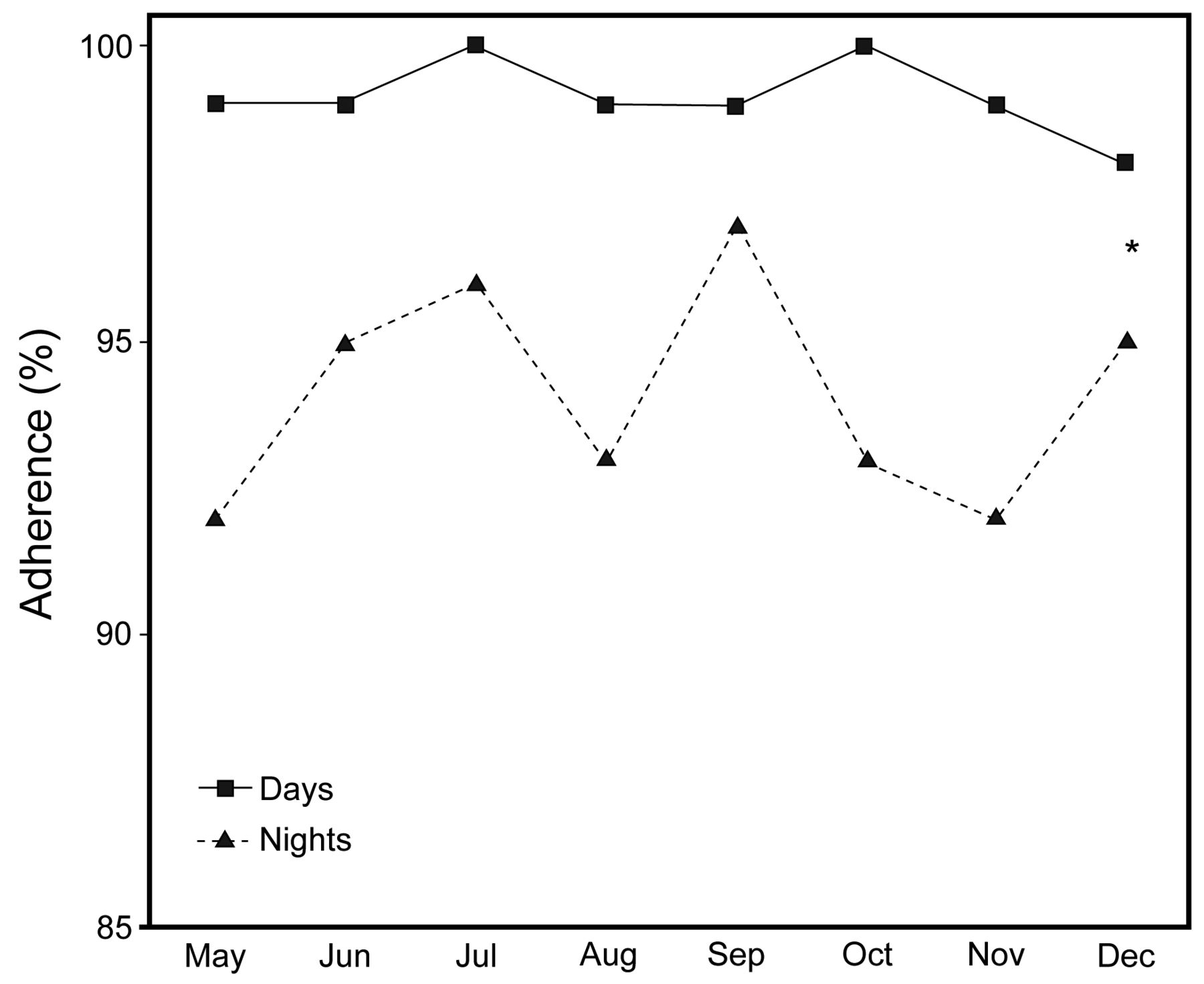
Intermittent head of bed elevation adherence checks (study period 2007). * P = .02.
There were no significant changes in adherence rates with non-HOBE VAP bundle components during the intervention period, compared with either the 3-month run-in period or compared with the 2 years prior to the study (data not shown).
Discussion
The important findings of this study are that continuously monitoring HOBE with an electronic device that allows continuous data display at the bedside, when combined with visual and auditory cues, improves adherence to maintaining the HOBE ≥ 30°. We also found that intermittent in-room bed checks consistently overestimated adherence to HOBE ≥ 30°.
HOBE ≥ 30° is a core component of the multi-parameter mechanical ventilation/VAP care pathway in our MICU. Drakulovic et al demonstrated a significant reduction in both clinically suspected and microbiologically confirmed pneumonia when ventilated patients were cared for in the semi-recumbent (45°) position.9 Kollef et al10 demonstrated that HOBE < 30° during the first 24 hours of mechanical ventilation was one of 4 independent risk factors for VAP. While these earlier studies demonstrated the benefit of 45° head-up position, more recently De Blasio et al reported that gastroesophageal reflux and aspiration is comparable between the 30° and 45° HOBE.19
We used bundled standard care orders including HOBE ≥ 30°, combined with adherence assurance quality check lists that have been demonstrated to be effective in reducing VAP rates.16,17,20 Despite these efforts supplemented with the visual and auditory alarms during continuous HOBE monitoring, adherence in the HOBE V group was only 75.5%. However, this finding is in line with other reports.17,18,21 Scales et al reported that adherence increased from a baseline of 50.2% to 89.6% at the end of one year after implementation of standard care bundles and educational interventions to reduce VAP.17 HOBE observations were made intermittently in that study and not derived from continuous HOBE monitoring. While adherence improved overall, it is likely that actual adherence to HOBE ≥ 30° over 24 hours would have been lower when measured continuously rather than intermittently. Whether adherence would improve in a more consistent and sustainable fashion with prolonged implementation of the HOBE device is the focus of ongoing investigation.
Our study has a number of potential limitations. First, we did not collect HOBE data for the entire duration of mechanical ventilation in all patients (see Table 2) and we excluded ventilation episodes < 24 hours, since this would preclude comparison over a day and night shift. The number of hours monitored represented a quarter of those that could have been monitored and were distributed reasonably evenly over time such that the data should not have been biased by selective recording and that our observations were representative. The odds of HOBE ≥ 30° was consistently and statistically higher in V, compared with NV, monitored beds. This was true even when monitoring episodes were included during which monitor disconnection resulted in missing data (odds ratio 2.0 for all episodes, and odds ratio 2.4 when episodes with missing data were excluded). However, we were not able to perform secondary analyses controlling for the imbalance in rates of missing data between V and NV to explore the reasons for this imbalance.
Second, although we recorded data from only a single MICU, data from the literature indicate that adherence to HOBE is poor, and generally worse than what we observed in our control (ie, non-visible monitored) group.11,16,17,22 This could, in part, be attributable to the fact that patient care practices in our MICU emphasize a team-based approach such that nursing and respiratory therapy staff could be more integrally involved in patient care practices in our MICU than in other units. While other units might not achieve similar degrees of adherence, the difference we observed in adherence in the 2 groups should, if anything, underestimate the difference that might be found in other units reporting lower baseline adherence.
A third potential limitation to the external validity of our findings with a real-time HOBE device is that HOBE was monitored using spot-checks on a continual basis for several years before the study. While many ICUs do not routinely monitor HOBE adherence, this has been more frequently performed in many ICUs in recent years. We anticipate that a similar increment in performance adherence may be achievable in those ICUs, but are unable to assert the potential impact of the intervention in ICUs that do not routinely monitor HOBE adherence.
Fourthly, environmental and human factors vary significantly and contribute to the effectiveness of alerts and alarms in high care environments.23–32 Threshold alarms are routinely used for alerting providers to perturbations in physiologic parameters in the ICU.31 However, audible and visual alarm systems with high sensitivity but low specificity are frequently ignored or deactivated by providers, with variable consequences, including potential patient harm.27 Whether the visual cue prompts alone or in combination with auditory alarms triggered by HOBE < 30°, or some combination of these account for the improved adherence in our study is unknown. Since the study was limited to HOBE measurements and did not include patient or provider level information, we were not able to perform multivariable analyses to explore this further. We also did not measure the frequency with which the audible alarm for the HOBE device was deactivated.
Current international standards (International Electrotechnical Commission standard 60601-1-8)33 require that medical device audible alarms, including category and urgency alarm components, should be validated for efficacy and priority-encoded.34 Innovations in ICU monitoring technologies have focused on enhanced reliability and integration of multisensory cues and alarms to incorporate human and environmental factors. Our HOBE monitor used traditional threshold alarms as provider alerts. However, future development to reduce false alarms could incorporate multi-parameter fuzzy-logic algorithms.35
A fifth potential limitation is that while VAP rates are continuously monitored by routine surveillance in the MICU, VAP incidence was not a prespecified outcome for this study. Thus we were not able to conclude that the HOBE monitoring system reduces the incidence of VAP.
Conclusions
In conclusion, real time continuous bedside monitoring of HOBE using a visual display and audible alarms is a feasible intervention and improves adherence to HOBE 2.3-fold. HOBE intermittent checks consistently over-estimated adherence by as much as 25%. Despite a unit practice standard of HOBE ≥ 30°, optimal adherence was difficult to achieve even when visual monitoring and audible alarms were provided. Efforts to modify the alarm so as to allow for temporary lowering of the head of bed may improve adherence. Whether this approach reduces VAP has not yet been determined.
Acknowledgments
We thank Katherine Overdier and Angela Keniston MSPH for clinical coordination, data management, and production of the online video material.
Footnotes
- Correspondence: Ivor S Douglas MD, Denver Health Medical Center; 777 Bannock Street, MC 4000, Denver, CO 80204. E-mail: Ivor.Douglas{at}dhha.org.
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
See the Related Editorial on Page 659
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}