

Abstract
BACKGROUND: We report the process implemented in our institution by a task force focused on the reduction of ventilator-associated pneumonia (VAP).
METHODS: Retrospective cohort study of all adults admitted to one of our 4 adult ICUs, intubated on invasive mechanical ventilation. We implemented a ventilator bundle in April of 2007; we report the incidence of VAP in 2008, and, after adjustment in the process (oral care performed by respiratory therapists), the incidence in 2009. The primary outcome was reduction of the microbiologically confirmed VAP rate over a 2 year period. Other outcomes were duration of mechanical ventilation, antibiotic days, ICU and hospital stay, and mortality.
RESULTS: During the study period, 2,588 patients received invasive mechanical ventilation in the adult ICUs. The VAP rate during 2008 was 4.3/1,000 ventilator days, and the 2009 rate was 1.2/1,000 ventilator days. The 2008 to 2009 VAP rate ratio was significantly greater than 1 (rate ratio 3.6, 95% CI 1.8–8.0, P < .001). Antibiotic days were less in 2009 versus 2008 (Hodges-Lehmann estimate of difference between 2008 and 2009, 1.0, 95% CI 0.0–1.0, P = .002). The median stay in the ICU was unchanged, and in the hospital was decreased in 2009 (Hodges-Lehmann estimate of difference between 2008 and 2009, 1.0, 95% CI 0.0–1.0, P < .001). The hospital mortality was 26.1%, and there was no difference between the 2 years. Adherence with the ventilator bundle was above 92% during the study period, but the oral care adherence improved from 33% to 97% after respiratory therapists assumed oral care.
CONCLUSIONS: Reduction of the incidence of VAP occurred with an intervention that included respiratory therapists doing oral care in patients receiving invasive mechanical ventilation. Oral care done by respiratory therapists may be associated with reduction of VAP.
Introduction
Ventilator-associated pneumonia (VAP) is an infection that occurs in patients in the ICU receiving invasive mechanical ventilation, and is associated with increased stay in the ICU and in the hospital, increased cost, and may be associated with an increased mortality.1–3 The incidence of VAP may be declining in the United States,2,4 probably due to the implementation of ventilator bundles, a set of practices that, if performed collectively and reliably, may improve patient outcomes.4 The components of the ventilator bundle are: elevation of the head of the bed, daily sedation “holidays” and assessment of the readiness to extubate, and prophylaxis for peptic ulcer disease and for deep venous thrombosis.5,6 Daily care of the oral cavity with chlorhexidine is used as well to try to reduce the rate of VAP.6,7
As part of a quality improvement process in our institution, the administrative leadership created a multidisciplinary VAP task force to implement evidence-based practices, including the ventilator bundle. The task force was led by an intensivist (ACA) and included a multidisciplinary group of registered nurses (RNs), respiratory therapists (RTs), and infection control practitioners. The objective of this task force was to reduce the incidence of VAP. We report the process that the task force implemented since April of 2007 and compare the rates of VAP in the adult population in the years 2008 and 2009, after adjustments in the program were made.
QUICK LOOK
Current knowledge
A ventilator-associated pneumonia (VAP) bundle is a set of procedures accomplished by a multi-disciplinary team, to decrease the incidence of VAP.
What this paper contributes to our knowledge
Tasking oral care to respiratory therapists increased adherence to the VAP bundle from 33% to 97%.
Methods
A retrospective single center observational cohort study was done at Scott and White Hospital, Temple, Texas, for all patients who received invasive mechanical ventilation in the adult ICUs between January 1, 2008, and December 31, 2009 (institutional review board study number 100506, exempt).
Setting and Organization of the ICUs
Scott and White Memorial is a 636-bed teaching, referral hospital in central Texas. The hospital has 55 adult ICU beds distributed in 4 units, including medical, surgical-trauma, cardiac, and cardiothoracic. The ratio of RNs to patients is 1:2, and the ratio of RTs to patients is 1:5. All of the units are closed and are staffed by board certified intensivists. All of the units are staffed by residents, and the medical and cardiac ICUs are staffed as well with fellows in pulmonary and critical care medicine and cardiology, respectively.
Implementation of a Pathway for Diagnosis and Prevention of VAP
In April of 2007 an integrated care pathway was introduced for the diagnosis and prevention of VAP. The initial step was standardization of the diagnostic criteria in all of the ICUs. We used the standard definition for VAP from the Centers for Disease Control and Prevention.8 After the patient was identified by clinical and radiological criteria, the case was reviewed by an infection control practitioner as well as an intensivist who was not involved in the care of the patient and adjudicated the case based on the clinical information provided. All suspected cases of VAP underwent a non-bronchoscopic protected catheter lavage (mini bronchoalveolar lavage) (Kimberley-Clark, Roswell, Georgia).9 The quantitative culture was positive if 104 colony-forming units/mL or greater grew in the specimens of patients intubated for at least 48 hours.10
Education was an important component of the pathway and included a lecture for RNs, RTs, residents, and fellows as part of the curriculum, which was given as well in local symposiums. In October of 2007 all clinicians participating in the care of patients in the ICUs had to watch a video that was produced and posted on the intranet, addressing the major components of the ventilator bundle. The video was based on the report by Babcock et al11 and had general information regarding VAP, including the definition, epidemiology, risk factors, bacterial etiology in our institution, clinical presentation, diagnostic methods, treatment, and outcomes, including mortality rate and cost. In-services were continued in 2008 and 2009 and were part of the yearly competency of RNs and RTs. Bulletin boards were posted in the ICUs, and discussion with emphasis on prevention of VAP was encouraged during daily rounds.
Epidemiologic surveillance was done by infection control practitioners. In June 2007, surveillance and adherence to the ventilator bundle was done by review of the daily ventilator report and review of the electronic medical records. In March 2008, daily rounding by the infection control practitioner was implemented to observe bundle adherence, for one month. In July 2007 the RTs started checking the position of the head of the bed and entering in their ventilator data sheet every 4 hours. They were instructed that if the head of the bed was < 30° they should ask the bedside RN for a reason, and if there was not a specific reason (ie, hypotension) then the head of the bed would be elevated to at least 30°. As part of our practice, supervisors randomly confirm the accuracy of the data entered into the ventilator sheet at least twice a week.
The care of the oral cavity was implemented by RNs in November 2007, with hydrogen peroxide solution every 4 hours, using oral swabs and a toothbrush. In July 2008, low adherence with oral care was observed and we implemented a new round of educational activities. In November 2008 we changed the process and the task force charged the RTs to do the oral care, because of their familiarity with suctioning of the oral cavity and the daily change of the endotracheal tube from side to side of the mouth. From November 2008 to January 2009 the oral care was done together by RTs and RNs. From February 1, 2009, the oral care was done entirely by the RTs. Finally, on March 1, 2009, we changed the oral care to chlorhexidine 2% solution, done by RTs every 12 hours.7 The timeline for the implementation of the process is shown in Figure 1.
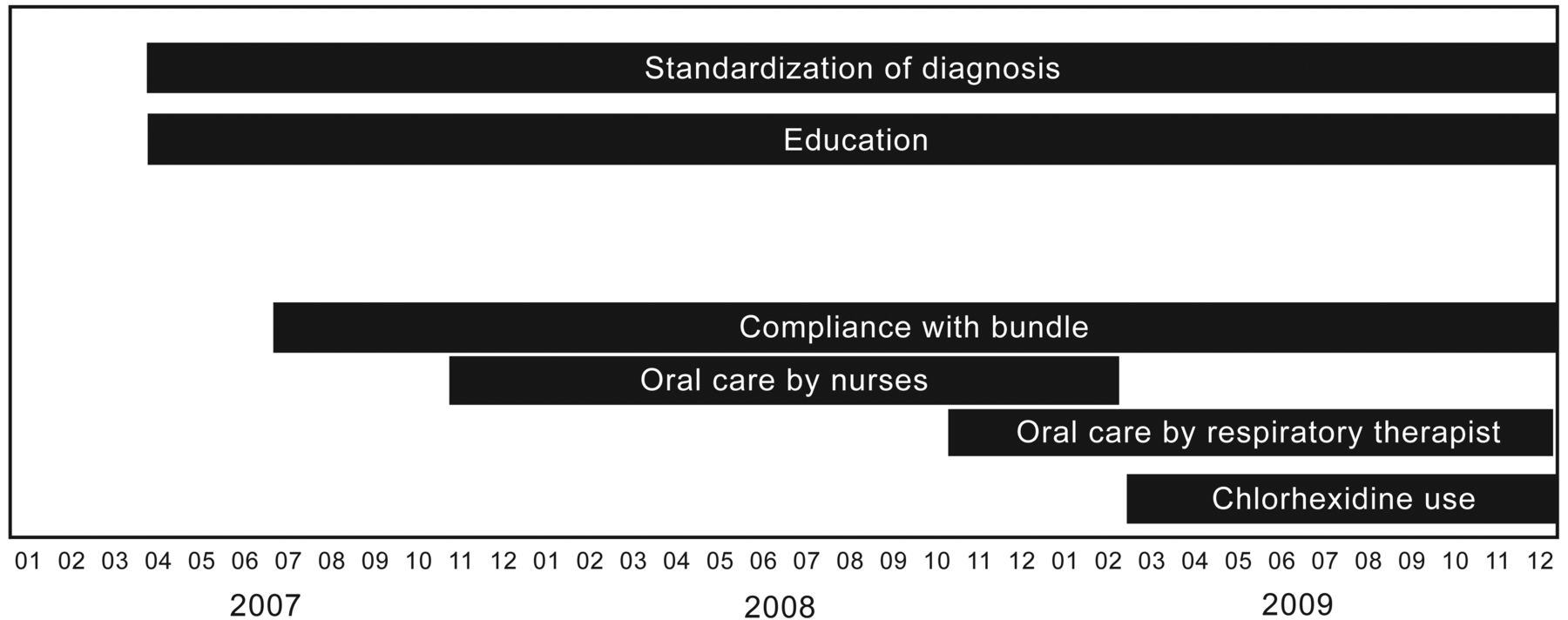
Timeline for the implementation process for the prevention of ventilator-associated pneumonia.
Local practices that may affect the rate of VAP, such as administration of proton-pump inhibitors,12,13 feeding via the enteral route, nurse-led sedation protocol,14 and weaning protocol,15 have been the usual practice in these units for several years, and were not changed during the observational period. Selective digestive tract decontamination and endotracheal tube with subglottic suction were not used. Restrictive use of red blood cell transfusion has been an established practice in the ICUs for several years.16 Silver-coated endotracheal tubes17 were used only sporadically since June 2008. There were no important changes in the heated humidification system used in 2008 and 2009 or in the frequency of changes of ventilator circuits and closed suction system; in general the ventilator circuits and the suction system were changed when visibly soiled.
Outcomes Measures
A database was constructed from our medical informatics system, based on claims data, clinical data in our electronic medical records, and the database kept by the department of infection control. The primary outcome was the reduction of the microbiologically confirmed VAP rate over a 2 year period. Other outcomes were duration of mechanical ventilation (ventilator days), antibiotic days (number of antibiotics multiplied by the duration of treatment in days),18 ICU and hospital stay, and mortality.
Statistical Analysis
Characteristics of ventilation cases during the January-December 2008 and the January-December 2009 periods were summarized and compared utilizing a 2 sample t test or Wilcoxon rank-sum test for continuous variables, and Chi-square test or the Fisher exact test for categorical variables. Median differences between 2008 and 2009 and CIs were reported using Hodges-Lehmann estimates, along with the respective Wilcoxon rank-sum test P values. Monthly VAP rates/1,000 ventilator days were estimated at each month from January-December 2008 and January-December 2009.
The median of monthly VAP rates of 2008 and the median of monthly VAP rates of 2009 were compared using the Wilcoxon rank sum test. The 2008 to 2009 VAP rate ratio was tested using the Z test.19 Univariate and multivariable logistic regression analyses were performed to investigate factors associated with higher incidence of VAP. A 2-sided test was used for P value calculation. A P value of < .05 indicated statistical significance. Software (SAS 9.2; SAS Institute, Cary, North Carolina) was used for data analysis.
Results
During the study period, 2,588 patients received invasive mechanical ventilation in one of the adult ICUs, and 194 patients were admitted more than once (2,782 cases). One patient who was transferred from another hospital and did not have specified ventilator days was excluded from the analysis. Therefore, 2,781 cases of 2,587 patients were included for further analysis, and 2,781 cases were considered as independent events. One hundred twenty-six patients had 2 ventilation cases, 27 patients had 3 ventilation cases, 2 patients had 4 ventilation cases, and 2 patients had 5 ventilation cases.
There were 1,357 cases in 2008, and 1,424 cases in 2009. The ages of the patients were similar in both years (Table 1). Other demographic information is also presented in Table 1.
Descriptive Statistics of Ventilation Cases According to Ventilator Year (2008 vs 2009)
The VAP rate during 2008 was 4.3/1,000 ventilator days, and the 2009 rate was 1.2/1,000 ventilator days, and the 2008 to 2009 VAP rate ratio was significantly greater than 1 (rate ratio 3.6, 95% CI 1.8–8.0, P < .001, Table 2). A significant difference was detected in the median of monthly VAP rates between 2008 and 2009, based on Wilcoxon rank-sum test (Hodges-Lehmann estimate 3.3, 95% CI 1.9–4.7, P < .001). Figure 2 presents a plot of monthly VAP rates over time, along with the median of monthly VAP for each year. The number of antibiotic days was reduced in 2009 (median 8 d, minimum 1 d, maximum 94 d) versus 2008 (median 10 d, minimum 1 d, maximum 124 d) (Hodges-Lehmann estimate 1.0, 95% CI 0.0–1.0, P = .002) (see Table 1).
VAP Rates/1,000 Ventilator Days and Quarterly VAP Rates

Monthly ventilator-associated pneumonia (VAP) rates and median for 2008 and 2009.
The bacteria more commonly isolated from the patients with VAP were methicillin-resistant (22%) and methicillin-sensitive Staphylococcus aureus (18%) and Pseudomonas aeruginosa (12%) (Table 3). The most common antibiotics used were vancomycin, piperacillin/tazobactam, ciprofloxacin, and cefepime (see Table 3).
Ten Most Common Pathogens and Antibiotics
The median (min-max) stay in the ICU was 5 (1–92) days in 2008, and 5 (1–49) days in 2009 (Hodges-Lehmann estimate 0.0, 95% CI 0.0–0.0, P = .60). The median (min-max) stay in the hospital was 10 (1–211) days in 2008, and 9 (0–83) days in 2009 (Hodges-Lehmann estimate 1.0, 95% CI 0.0–1.0, P < .001, Table 4). The hospital mortality for the whole cohort was 26.1%, and there was no difference between the 2 years (27.5% vs 24.8% for 2008 vs 2009, difference between 2008 and 2009 in proportions [2.7%, 95% CI −0.6 to 6.0%, P = .10]). The mortality values for patients diagnosed with VAP were similar in both years (see Table 4).
Hospital Stay and Mortality
The adherence with the ventilator bundle was high for all of the ICUs when it was measured by an infection control practitioner for the whole month of March 2008. The adherence was 98% with sedation “holidays,” keeping the head of the bed elevated, and prophylaxis for deep vein thrombosis and stress ulcer. A trial of weaning was attempted in 92% of patients eligible. After November 2008, RTs kept and documented elevation of the head of the bed every 4 hours, sedation holiday, and daily weaning trials as indicated, with an adherence rate of 97% in all components. The adherence rate for oral care was 33% in May 2008 and 100% in November 2008, and remained above 97% during the study period.
The univariate analysis (Table 5) showed that being admitted to the ICU in 2008, compared to 2009, younger age, more ventilator days, more antibiotic days, longer ICU and hospital stay, and having PaO2/FIO2 of < 200 mm Hg were significantly associated with increased incidence of VAP (see Table 5). In the multivariable logistic regression model (Table 6) the year admitted to the ICU, age, and ventilator days remained significant.
Univariate Logistic Regression Analysis According to Presence/Absence of VAP (n = 2,781)
Reduced Multivariable Logistic Regression Analysis According to Presence/Absence of VAP
Discussion
The important findings of this study are that the rate of VAP significantly decreased in 2009 and remained low for the whole year, and that the length of hospital stay and antibiotic days were reduced in 2009, when compared with 2008. The hospital mortality did not change in the 2 year period.
In this study we chose to measure an outcome, VAP rate, because we had a strong process anchored in a well accepted definition of VAP; adjudication of the diagnosis of VAP was done by clinical experts who were not involved in the clinical management and bacteriologic diagnosis. The adherence to key measures of the ventilator bundle during the whole period of the study was very high. Although we had very high adherence to the bundle, it has been suggested that self reported adherence may overestimate performance.20 Some authorities4 have suggested that documentation of adherence with the ventilator bundle is not a viable quality measure. The use of the ventilator bundle by trained staff was already in place months before the study period and was associated with adherence above 97%; therefore, the finding of a reduction of VAP rate was probably not related to adherence with the ventilator bundle, but to other changes in the process of care.
In November 2008 the RTs started performing oral care together with the bedside nurses, and in February 2009 we started using chlorhexidine gluconate done by the RTs.7 After the RTs started performing the oral care in every intubated patient admitted to the ICUs, the adherence rate for oral care improved dramatically, from 33% to 100%, and remained 97% for the study period. It was our clinical observation that RTs were comfortable doing oral care because they are used to dealing with the oral endotracheal tube, and our hypothesis was that it will be easier to perform consistent comprehensive oral care when it is done by RTs. We capitalized on that clinical observation, and although this study cannot establish causality, the significant reduction in the rate of VAP occurred at the period of time when oral care was done by the RTs, raising the possibility that RT oral care may be associated with decreased rate of VAP.
It is difficult, due to our study design, to pinpoint the exact reason for the reduction in the VAP rate. We believe that the increased adherence in oral care achieved after the RTs were involved may have played an important role in addition to the high adherence with the measures of the ventilator bundle.4 Our study differs from other studies reported in the literature in several aspects: the most important is that the RTs in this study not only played a role in the weaning process21,22 but did the oral care and were accountable because they were supervised closely. Another important difference is that, contrary to most studies that assess physician adherence to evidence-based guidelines for the prevention of infections,23 this study emphasizes the fact that it takes a team to reduce the VAP rate in these complex patients. We believe that we improved the care because we developed a new organization of the work; were more interested in how a task (oral care) was done; engaged a team of RNs, RTs, infection control practitioners, and MDs who assumed ownership of the project; had the support of the leadership of the institution; and created a collaborative culture within the ICUs.20
Another important observation of this study was that the number of antibiotic days was reduced in 2009 (see Table 1). We reported antibiotic days as a proxy for the use of antibiotics. If a patient received vancomycin for 7 days and ciprofloxacin for 6 days, then the number of antibiotic days was 13 days.17 In 2008 the median duration of antibiotic days was 10 days (minimum 1, maximum 124 d), and in 2009 the median was 8 days (minimum 1 d, maximum 94 d): a reduction of 2 days (Hodges-Lehmann estimate 1.0, 95% CI 0.0–1.0, P = .002). Again, although this study cannot establish causality, the observation is important and may possibly be associated with the reduction of the number of VAPs.
The most important limitations of the study were its retrospective nature and the fact that it is a single center study. Another important limitation was that our database does not have metrics for severity, such as Acute Physiology and Chronic Health Evaluation (APACHE) score; however, we believe that PaO2/FIO2 will provide the clinician a measure of the hypoxemia present in the patients at the time of intubation.23 However, within its limitations, this study reports a strong process of implementation driven by a multidisciplinary group, over a specific period of time, with measurable and clinically important outcomes.
Conclusions
In this single center study, the use of the ventilator bundle was high. Significant reduction of the rate of VAP occurred after the oral care was done by RTs in patients receiving invasive mechanical ventilation.
Footnotes
- Correspondence: Alejandro C Arroliga MD, Division of Pulmonary and Critical Care, Scott and White Hospital, Texas A&M Health Science Center College of Medicine, 2401 S 31st Street, Temple TX 76508. E mail: aarroliga{at}swmail.sw.org.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 811
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}