

Abstract
BACKGROUND: Despite potential benefits of intrapulmonary percussive ventilation (IPV) in various respiratory diseases, the impact of setting parameters on the mechanical effects produced by IPV in the lungs is unknown. We hypothesized that changing the parameters on IPV would modulate these effects. This in vitro study aimed at comparing the changes in intrapulmonary effects resulting from changes in parameters in 3 portable IPV devices (IMP2, Impulsator, and Pegaso).
METHODS: Parameters were set in 72 combinations of frequency (90–250 cycles/min), inspiratory to expiratory (I/E) time ratio (from 1/2 to 3/1), and pressure (10–60 cm H2O). Four resulting effects were recorded on a test lung via a pneumotachometer: the expiratory to inspiratory flow ratio (E/I flow ratio), the PEEP, the ventilation, and the percussion. Percussion was assessed by the end-slope of the pressure curve. Analysis of variance was used for data analysis.
RESULTS: E/I flow ratio increased with increasing I/E time ratio (P < .001). The Pegaso produced the lowest E/I flow ratio. PEEP raised 6 cm H2O in both IMP2 and Impulsator, and 17 cm H2O in the Pegaso with increasing frequency (P < .01), pressure, and I/E time ratio (P < .001). In all devices, ventilation increased with increasing pressure and decreasing frequency (P < .001). Percussion increased with increasing frequency and decreasing I/E time ratio (P < .001), and with increasing pressure when I/E time ratio was 1/1 or less. The Pegaso provided the poorest percussion.
CONCLUSIONS: This study suggests that changing the parameters considerably modulates the mechanical effects produced by portable IPV devices in the lungs. Increasing frequency increased PEEP and percussion, but decreased ventilation. Increasing I/E time increased PEEP and E/I flow ratio, and decreased percussion. Finally, increasing pressure increased PEEP and ventilation. The Pegaso produced the highest PEEP, least percussion, and smallest change in E/I flow ratio.
Introduction
Intrapulmonary percussive ventilation (IPV) is a pneumatic device for providing chest physiotherapy. IPV is expected to loosen and mobilize secretions toward the upper airways in patients with restrictive and obstructive pulmonary diseases affected by severe endobronchial encumbrance. IPV delivers high-frequency ventilation into the lungs, in the form of intrapulmonary percussions. Percussions, ranging from 60 to 400 cycles/min, consist of small bursts of volume characterized by sharp peaks of pressure (Fig. 1). IPV may be delivered via a face mask, a mouthpiece, an endotracheal tube, or a tracheostomy. Recent reports have suggested that IPV facilitates airway clearance and improves homogeneity of ventilation in patients with cystic fibrosis,1–5 in patients with neuromuscular disorders with retention of mucus,6,7 in patients with atelectasis,8–10 in burned patients with inhalation injury,11–13 and in patients with COPD.14–17

Typical curve of pressure (A) and flow (B) with intrapulmonary percussive ventilation (IPV) devices (in casu IMP2 with frequency of 180 cycles/min, I/E time ratio of 2/1, and pressure of 10 cm H2O). The area under the flow-time curve for each breath represents the tidal volume.
Despite potential benefits related to the use of IPV therapy, the impact of setting parameters such as the ratio of inspiratory to expiratory time, the pressure, and the frequency on the mechanical effects produced by IPV devices is totally unknown. As a consequence, no evidence is available to advise caregivers on how to set parameters to conduct their therapies. We hypothesized that changing the settings on IPV would modulate these mechanical effects in the lungs. In this in vitro investigation, we aimed at measuring and quantifying changes in mechanical effects resulting from changes in parameter settings in portable IPV devices.
QUICK LOOK
Current knowledge
Intrapulmonary percussive ventilation (IPV) devices provide a method for secretion removal that includes both hyperinflation and internal percussion.
What this paper contributes to our knowledge
Changing the settings of IPV devices alters the mechanical effects in the lungs. Increasing the frequency results in an increase in PEEP and percussion, but decreased ventilation. Increasing the inspiratory-expiratory time ratio increases PEEP and expiratory-inspiratory flow ratio, and decreases percussion. Increasing the pressure increases PEEP and ventilation. Manipulation of IPV settings to maximize ventilation, secretion removal, and lung inflation is possible.
Methods
Three IPV devices equipped with their own internal compressors, the IMP2 (Breas, Mölnlycke, Sweden), the Impulsator (Percussionaire, Sandpoint, Idaho), and the Pegaso (Dima, Bologna, Italia), were compared. In order to standardize the setting of parameters in all devices, parameters were set following monitoring via a heated Fleisch no. 2 pneumotachometer (Metabo, Lausanne, Switzerland) placed in line between the IPV circuit and an adult test lung (SmartLung, IMT Medical, Buchs, Switzerland). The characteristics of the lung were set at the highest compliance (30 mL/ cm H2O) and lowest resistance (5 cm H2O/L/s) of the test lung. Volumes and timing of ventilation were obtained by integration of flow signals. Recorded data were computed in a data analyzer (MEC, Medical Electronic Construction, Brussels, Belgium).
Parameters on IPV
Parameters on IPV were successively combined in 3 conditions of frequency (90, 180, and 250 cycles/min); 4 conditions of inspiratory to expiratory (I/E) time ratio (1/2, 1/1, 2/1, and 3/1); and 6 conditions of pressure (10–60 cm H2O). At our request, the 50 cm H2O high pressure limit on the IMP2 was suppressed by the manufacturer to allow comparable pressures in all devices. This study allowed the comparison of 72 combinations recorded each during 30 seconds. The first 10 seconds were necessary to allow stability of the compressors and were therefore not considered for analysis.
Mechanical Effects In the Lung
As previously described,18 4 mechanical effects were compared: the ratio of expiratory to inspiratory flow (E/I flow ratio), the ventilation as assessed by the tidal volume (VT), the PEEP, and the percussion. The sharpness of percussion was assessed by the slope of the pressure curve, measured 60 ms prior to the peak of pressure. Higher slope values indicated steeper inclines, which in turn estimated sharper peaks of pressure curve. Data were analyzed during the first 20 cycles recorded between the 10th and the 30th second of recording. Figure 1 represents typical pressure (see Fig. 1A) and flow (see Fig. 1B) curve measurements.
Analysis
Analysis of variance (ANOVA) was used to assess the variation of the parameters in the 72 setting combinations in each device (1-way ANOVA) and to compare the 3 devices in the same combination (2-way ANOVA). Software (Medcalc, Mariakerke, Belgium) was used for statistical analysis. Significance was accepted at P < .05.
Results
Expiratory-Inspiratory Flow Ratio
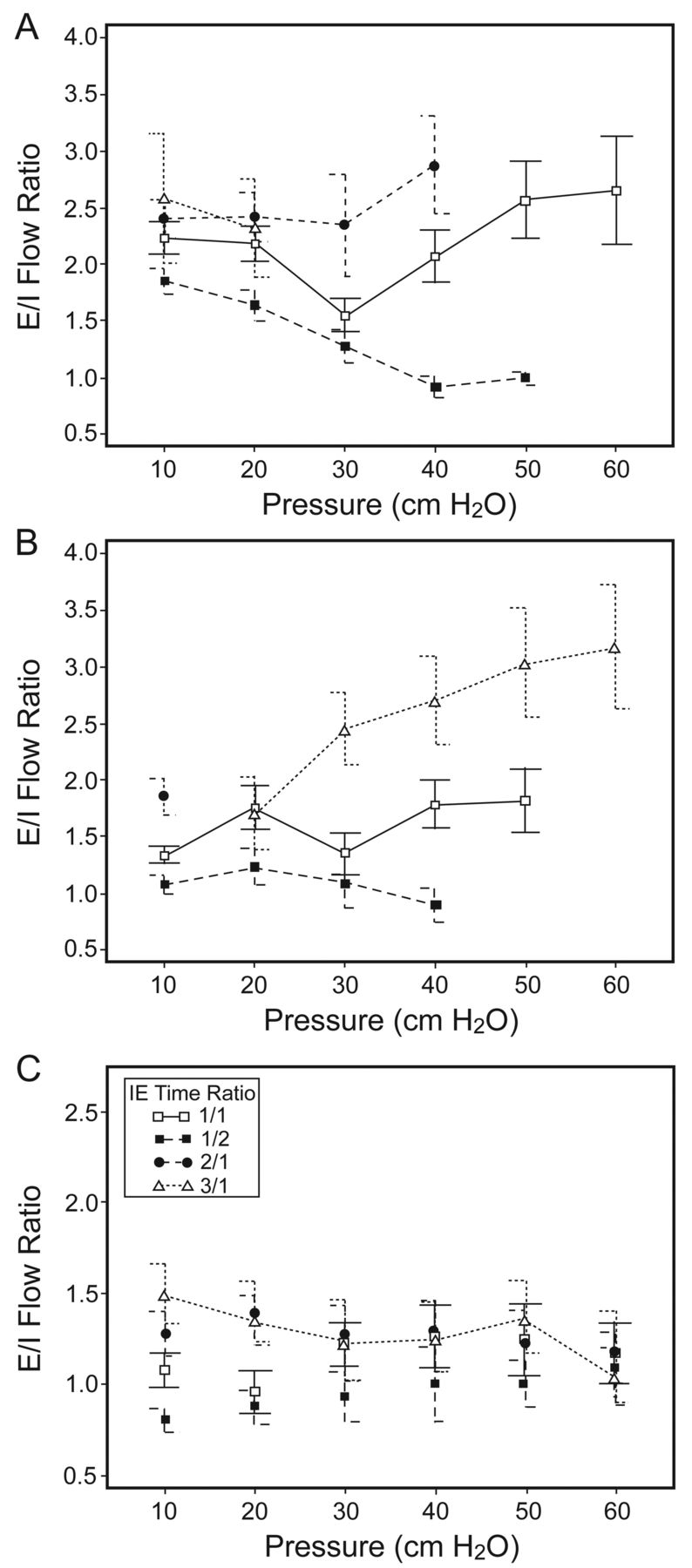
Due to the characteristics of its internal air compressor, the Impulsator provided a smaller range of I/E time ratio settings, as compared to other IPV devices, at frequencies set at 180 and 250 cycles/min. Figures 2 and 3 depict E/I flow ratios with frequencies at 90 and 250 cycles/min, respectively. In general, the E/I flow ratio increased with increasing I/E time ratio in the 3 devices (P < .001), but an exception was found with pressures ≥ 30 cm H2O and frequency at 90 cycles/min with the Pegaso. The highest E/I flow ratios were found with the IMP2. The lowest E/I flow ratios were found with the Pegaso. With frequencies at 90 cycles/min (with pressures ≤ 30 cm H2O), 180 cycles/min, and 250 cycles/min the Impulsator provided lower E/I flow ratios than the IPM2.

Changes in expiratory-inspiratory (E/I) flow ratio with increasing pressure at frequency of 90 cycles/min. A: IMP2. B: Impulsator. C: Pegaso.

Changes in expiratory-inspiratory (E/I) flow ratio with increasing pressure at frequency of 250 cycles/min. A: IMP2. B: Impulsator. C: Pegaso.
With the exception of I/E time ratio at 3/1 with a frequency at 90 cycles/min in the Impulsator (see Fig. 2B), increasing pressure did not change the E/I flow ratios. In the IMP2 solely, E/I flow ratios were higher at low (< 20 cm H2O) and high (> 40 cm H2O) pressures for a timing ratio of 1/1 in the 3 conditions of frequencies. As a general rule, changes in frequency did not affect E/I flow ratios.
PEEP
A PEEP was always present in the 3 IPV devices. However, IMP2 and Impulsator could not achieve the set pressure for some of the longer I/E ratios. Table 1 reports available PEEP values. The highest PEEP was found at the highest frequency, set at 250 cycles/min. PEEP increased with increasing pressure (P < .001) and frequency (P = .008) from 0.5 to 6 cm H2O in both IMP2 and Impulsator, and from 2.4 to 17 cm H2O with the Pegaso. Increasing I/E time ratio increased PEEP in the 3 conditions of frequency (P < .001). The influence of I/E time ratio on PEEP was larger with the Pegaso than with the other IPV devices.
PEEP With a Constant Frequency at 250 Cycles/Min and Increasing I/E Time Ratio and Pressure
Ventilation
As a general trend, increasing pressure significantly increased VT in all combinations of frequencies and I/E time ratios (P < .001). The largest VT, presented in Table 2, were found with the lowest frequencies in all devices (P < .001). At similar frequencies, inconsistent differences in VT were found among the devices. However, at a frequency of 90 cycles/min, VT was larger with the IMP2 and Impulsator than with the Pegaso with I/E time ratios from 1/2 to 2/1 and with pressures superior to 30 cm H2O. With a frequency of 180 cycles/min, VT ranged 110–210, 100–220, and 100–240 mL with the IMP2, Impulsator, and Pegaso, respectively. With a frequency of 250 cycles/min, VT was lower than 160 mL in the 3 devices. Finally, changes in I/E time ratio did not affect VT.
Tidal Volume With a Constant Frequency at 90 Cycles/Min and Increasing I/E Time Ratio and Pressure
Percussion
Typical pressure curves are shown at high (Fig. 4A) and low frequency (see Fig. 4B). In all devices, the slope of pressure increased with increasing frequency and decreasing I/E time ratio (P < .001). The higher slope values, presented in Table 3, were recorded at a frequency of 250 cycles/min. With decreasing E/I time ratio in the IMP2, Impulsator, and Pegaso, respectively, slopes ranged 7–180, 9–111, and 3–125 cm H2O/s with a frequency of 90 cycles/min, while slopes ranged 19–175, 15–119, and 7–133 cm H2O/s with a frequency of 180 cycles/min. By contrast with large I/E time ratios (≥ 2/1), the sharpness of the peaks of pressure increased with increasing pressure when I/E time ratios were small (≤ 1/1). Extensive slope data for the IMP2, Impulsator, and Pegaso are reported in the tables in the supplementary materials at http://www.rcjournal.com. As shown in Figure 4, the IMP2 was similar to the Impulsator in producing sharp slopes, while the Pegaso provided lesser degrees of slope sharpness. The impact of setting parameters on the mechanical effects produced by portable IPV devices is summarized in Table 4.

Typical pressure curves of the 3 intrapulmonary percussive ventilation devices at high and low frequency. A: Frequency of 250 cycles/min, inspiratory-expiratory (I/E) time ratio of 1/2. B: Frequency of 90 cycles/min, I/E time ratio of 1/1. Note that high frequency (A) shows sharper slopes of pressures than does low frequency (B) in the 3 devices.
Slopes of the Pressure Curve With a Frequency at 250 Cycles/Min and Increasing I/E Time Ratio and Pressure
Impact of Setting Parameters on the Mechanical Effects Produced by Intrapulmonary Percussive Ventilation in the Lungs
Discussion
This study aimed at determining the impact of setting parameters on 4 mechanical effects produced by IPV in a test lung. To our knowledge, this is the first study mapping mechanical effects of IPV devices.
Expiratory-Inspiratory Flow Ratio
The first finding of this study was that E/I flow ratio consistently increased with increasing I/E time ratio, in all circumstances and devices. This finding had previously never been demonstrated with IPV devices and should explain in part how IPV therapy potentially supports mucus clearance. The clinical interest of increasing expiratory flows is intuitively evident: effective mucus clearance is expected when the expiratory flows exceed the inspiratory flows by a certain amount.18
Previous in vitro and in vivo studies already demonstrated that increased expiratory flows induced by increased inspiratory time favor mucus clearance. Kim et al19 investigated in vitro flow models with mechanical ventilation, maintaining E/I flow ratios at 1.5/1, 2/1, and 3/1. They found that mucus transport speed linearly increased with increasing E/I flow ratio. In an in vivo study, Benjamin et al20 instilled mucus into the bronchi of mechanically ventilated anesthetized sheep. In this study, they compared inverse I/E time ratios (inspiratory greater than expiratory time) at 1.9/1 and 3/1 versus a conventional I/E time ratio set at 1/2.7. I/E time modes of 1.9/1 and 3/1 produced E/I flow ratios of 2.2/1 and 3/1, promoting transport of mucus, while the I/E time ratio of 1/2.7 did not clear mucus, with an unfavourable E/I flow ratio recorded at 1/1.6. The authors concluded that inverse time ratio ventilation might be useful in the management of excessive bronchial secretions in mechanically ventilated patients.
These findings are consistent with those of King et al.21 Again, expiratory flow bias (expiratory > inspiratory flow) was compared with inspiratory flow bias in anesthetized dogs receiving mechanical ventilation with high frequency oscillations at 13 Hz. They found that mucus clearance was 2.4 times higher with expiratory bias than with inspiratory bias. In another in vivo study on anesthetized sheep, Freitag et al22 evaluated whether high frequency oscillations with biased expiratory flow profile was capable of augmenting mucus clearance. They compared expiratory bias (E/I flow ratio of 2.9/1) with inspiratory bias oscillations (E/I flow ratio of 1/2.9). As in the previous studies, significant clearance was measured when expiratory flows were greater than inspiratory flows.
Interestingly, Volpe et al23 recently investigated the conditions of flow necessary to support the movement of airway secretions. In an in vitro study using photodensitometry to measure the center-of-mass displacement of mucus, they found that the minimal value of E/I flow ratio to move mucus toward the mouth was 1.3/1. Under the threshold value of 1.3/1, mucus was transported toward the peripheral airways. By contrast with the Pegaso, which did not reach the threshold value suggested by Volpe's group, the IMP2 and Impulsator were both able to provide an asymmetric flow ratio greater than 1.3/1, therefore potentially enabling mucus transport in the direction of the expiratory flow. In the present study, the best way to increase E/I flow ratios was found to be increasing the I/E time ratio. Unfortunately, IMP2 and Impulsator are not designed to work with long inspiratory times (ie, I/E time ratio of 2/1 or 3/1). We would advise the manufacturers to enlarge this technical possibility in the future. Interestingly, adequate E/I flow ratios were found at all pressures, including those pressures under 20 cm H2O. This is useful since low pressures are commonly used in clinical practice. In the cases where the therapeutic goal is to optimize the transport of mucus, caregivers using IPV devices should be advised to use low pressures and to prolong the inspiratory time, aiming at enlarging expiratory flows.
In addition to the possible role of asymmetric flow ratios in clearing excessive bronchial secretions, the present data should also explain in part why the deposition of medication via the nebulizer of the IPV was found to be poor with IPV devices.24 Adequate deposition would require quiet inspiration with slow expiration, rather than a breathing pattern of higher expiratory than inspiratory flows, such as presently found with IPV.
PEEP
PEEP was previously found in every technique of high-frequency assisted airway clearance.18 Present in all combinations of parameters in our study, PEEP increased with pressure and I/E time ratio. To our surprise, a huge and uncontrollable PEEP was found with the Pegaso, while it remained low with all other IPV devices.
In patients with obstructive disease, PEEP effect has been suggested as useful in stabilizing the bronchial tree, removing secretions,25 improving ventilation, and reducing trapped air.26 When produced by IPV, PEEP has been shown to reduce expiratory flow limitation and work of breathing in COPD patients.14,17 In subjects without flow limitation, IPV may increase the work of breathing. PEEP may cause substantial discomfort, worsen gas exchange, and decrease cardiac output. The use of Pegaso should therefore be avoided in weak patients at risk for developing hypercapnia or cardiac insufficiency.
Ventilation
An important expected finding, however, was that increasing pressure and decreasing frequencies increased ventilation, as assessed by increasing VT, while increasing I/E time ratio did not. This is consistent with Nava et al,14 who showed that low frequencies ventilated and unloaded respiratory muscles better than high frequencies. Patients with little or no breathing autonomy therefore should require low frequencies, which are able to ventilate the lungs with comfort.6 Similarly, low frequencies, high pressures, and long inspiratory times should be selected by caregivers when the therapeutic goal is to provide hyperinsufflations.27,28
Percussion
The last finding was that percussions increased with increasing frequency and decreasing I/E time ratio. This was found in all IPV devices. Percussions also increased with increasing pressure when I/E time ratio was 1/1 or less. Percussive ventilation has consistently been reported as an effective method to improve blood gas exchange.8,15,17,29,30 Caregivers should therefore increase frequency and pressure, and decrease I/E time ratio when they wish to promote percussion in IPV devices.
Differences Among Tested IPV Devices
The Pegaso provided the largest range of settings. In general, the IMP2 and Impulsator provided similar effects. The IMP2 was the best device in producing elevated E/I flow ratios, while the lowest E/I flow ratios were found with the Pegaso. The latter produced abnormally elevated PEEP, while the 2 other devices produced low ones. The Pegaso also provided lesser degrees of percussion than the other 2 devices.
Rationale for Choosing Appropriate Settings
According to the targeted therapeutic goals, this study suggests new ways of setting the output of portable IPV devices (see Table 4). When airway clearance is the primary goal of therapy, caregivers should be advised to prolong the inspiratory time, therefore increasing expiratory flows, potentially improving mucus transport. In this case, the choice of the frequency and pressure should not influence expiratory flows. When ventilatory support or hyperinflation is the primary goal of therapy, frequency should be decreased and pressure increased. The I/E time ratio should not influence ventilation. When percussive effect is the primary goal of therapy (ie, atelectasis, peripheral airway encumbrance, narrowed airways), percussion should be enhanced by increasing frequency, reducing I/E time ratio, and increasing pressure. Finally, when PEEP effect is the primary goal of therapy, frequency, I/E time ratio, and pressure should all be increased. In clinical practice, the therapeutic goals are often mixed. The subtlety of setting parameters is in obtaining the best compromise to optimize each of the best effects.
Limitations of the Study
As in any in vitro study, the present results cannot be transferred to humans without caution. Test lungs mimic human lungs imperfectly. The current study, however, offers a mapping of the effects on a test lung with normal and stable compliance and resistance. Future in vitro and in vivo studies are needed on lungs with altered characteristics of resistance and compliance typically representing the patients requiring this therapy.
Another limitation is that the test lung is totally passive. Indeed, IPV allows the subjects to breathe free in the circuit (an exception is the Pegaso, which offers resistance to expiration, as evidenced by elevated PEEP). It is known that spontaneous ventilation modulates the physical effects of IPV.14 During active expiration, percussions are more intense and expiratory flows are amplified. Future studies are recommended to investigate the physical effects of IPV in healthy subjects and in patients whose compliance and/or resistance are altered.
Conclusions
In this study, 4 physical effects produced by portable IPV devices were measured, following the setting of frequency, I/E time ratio, and pressure. The results suggest that changing the parameters considerably modulates the mechanical effects produced by portable IPV devices in the lungs. Increasing frequency increased PEEP and percussion but decreased ventilation. Increasing I/E time ratio increased PEEP and E/I flow ratio, and decreased percussion. Finally, increasing pressure increased PEEP and ventilation. It also increased percussion when associated with minimal I/E time. The IMP2 and Impulsator produced the best mechanical effects, while the Pegaso produced the worst ones, as suggested by elevated PEEP, poor percussion, and minimal E/I flow ratio.
Footnotes
- Correspondence: Michel Toussaint PhD, Ziekenhuis Inkendaal Rehabilitation Hospital, Inkendaalstraat 1, 1602 Vlezenbeek, Belgium, Brussels. E-mail: michel.toussaint{at}inkendaal.be.
Supplementary material related to this paper is available at http://www.rcjournal.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}