

Abstract
BACKGROUND: Inspiratory rise time and cycling criteria are important settings in pressure support ventilation. The purpose of this study was to investigate the impact of minimum and maximum rise time and inspiratory cycling criteria settings on 6 new generation ventilators. Our hypothesis was there would be a difference in the exhaled tidal volume, inspiratory time, and peak flow among 6 different ventilators, based on change in rise time and cycling criteria.
METHODS: The research utilized a breathing simulator and 4 different ventilator models. All mechanical ventilators were set to a spontaneous mode of ventilation with settings of pressure support 8 cm H2O and PEEP of 5 cm H2O. A minimum and maximum setting for rise time and cycling criteria were examined. Exhaled tidal volume, inspiratory time, and peak flow measurements were recorded for each simulation.
RESULTS: Significant (P < .001) differences were found when comparing minimum and maximum rise time and minimum and maximum cycling criteria for each ventilator.
CONCLUSIONS: Significant differences in exhaled tidal volume, inspiratory time, and peak flow were observed by adjusting rise time and cycling criteria. This research demonstrates that during pressure support ventilation strategy, adjustments in rise time and/or cycling criteria can produce changes in inspiratory parameters. Obviously, this finding has important implications for practitioners who utilize a similar pressure support strategy when conducting a ventilator wean. Additionally, this study outlines major differences among ventilator manufacturers when considering inspiratory rise time and cycling criteria.
Introduction
Rise time is defined as the time with which airway pressure builds toward a preset maximum value.1 A rapid rise time value will allow instantaneous delivery of flow at the start of the breath, resulting in an immediate rise in pressure to the pre-set level.2 Conversely, a slow rise time inhibits initial flow delivery, thus delaying the pressure rise to the pre-set level.2 Rise time adjustments can directly and indirectly impact other parameters of mechanical ventilation.2
The cycling criteria control allows the clinician to adjust the termination of a pressure support breath based on the peak inspiratory flow.3 Simply stated, the cycling criteria determine the terminal portion of the inspiratory flow at which point the ventilator will cycle a pressure support breath into the expiratory phase. The cycling criteria are functional only during a pressure support breath. Our review of the literature shows that there is limited research comparing the effect of rise and cycling criteria adjustments on breath delivery during pressure support.
This study was designed to investigate the effects of rise time and cycling criteria setting adjustments on 6 contemporary ventilators. Specifically, we wanted to report the changes that occur in exhaled tidal volume (VT), inspiratory time (TI), and peak flow after making an adjustment in rise time and cycling criteria. The research highlights the impact of the minimum and maximum rise time and cycling criteria settings on the above spontaneous parameters and how the changes vary among 6 different ventilators. This paper is intended to build upon previous research on rise time and cycling criteria and thus provide the reader with additional information on the impact of making rise time and cycling criteria adjustments. Our null hypotheses was that there would be no differences in mean exhaled VT, TI, or peak flow, either within or between these ventilators at the various rise time and cycling settings.
QUICK LOOK
Current knowledge
The inspiratory rise time and cycling criterion during pressure support ventilation impact tidal volume, inspiratory time, peak inspiratory flow, and patient comfort. In patient studies the impact of the rise time and cycling criterion has varied with the type of pulmonary dysfunction: obstructive versus restrictive.
What this paper contributes to our knowledge
In this lung model study of 6 ventilators and one set of breathing parameters, the minimum and maximum rise time and cycling criterion significantly affected tidal volume, inspiratory time, and peak flow. Faster rise times were associated with shorter inspiratory times and larger tidal volumes, for a given cycling criterion. Higher cycling criteria were associated with shorter inspiratory times and smaller tidal volumes.
Methods
Lung Model and Ventilators
A breathing simulator (ASL 5000, Ingmar Medical, Pittsburgh, Pennsylvania) provided the breathing frequency and recorded all monitored parameters. A manual script was designed using a one-compartment lung model with a compliance of 80 mL/cm H2O and a resistance of 5 cm H2O/L/s. Compliance and resistance settings were based on typical normal values, as described in the available literature.4,5 The manual script allowed for a set breathing frequency of 12 breaths/min, inspiratory pressure triggering of −5 cm H2O for each breath, and an inspiratory trigger duration of 50 ms. The breathing simulator was heated to 37°C prior to each simulation. The breathing simulator is composed of a single cylinder piston with a total volume of 3 L and a default, uncompensated residual volume of 0.5 L.
All ventilators were placed in a spontaneous mode of ventilation with pressure support set at 8 cm H2O and PEEP/CPAP set at 5 cm H2O. The pressure support and PEEP/CPAP settings were specifically chosen based on recommendations for reducing the work of spontaneous breathing for mechanically ventilated patients.6
Various rise time (eg, minimum and maximum) and cycling criteria (eg, minimum and maximum) settings were examined on 6 ventilators: Evita XL (Dräger, Lübeck, Germany), Servo-i (Maquet, Wayne, New Jersey), and V500 (Dräger, Lübeck, Germany), Puritan Bennett 840 (PB840, Covidien, Mansfield, Massachusetts), Avea (CareFusion, San Diego, California), Esprit (Respironics, Murrysville, Pennsylvania), and LTV 1200 (Respironics, Murrysville, Pennsylvania). The minimum and maximum rise time and cycling criteria setting ranges were chosen because all 6 ventilators categorized the settings differently, thus making it impossible to establish identical intermediate settings among the ventilators. When possible, minimum and maximum rise time settings were combined with minimum and maximum cycling criteria settings. We were able to achieve this protocol for the Servo-i, Avea, Esprit, and LTV 1200. A cycling criteria of 25% was automatically fixed for our version of the Evita XL (ie, version 7.0); therefore, the settings assessed were minimum rise time with 25% cycling criteria, and maximum rise time with 25% cycling criteria. The breathing simulator was unable to produce a valid volume measurement when the rise time and cycling criteria were both set to maximum for the PB840. Therefore, the PB840 protocol was as follows: minimum rise time and minimum cycling criteria, maximum rise time and minimum cycling criteria, minimum rise time and maximum cycling criteria, and maximum rise time and sub-maximum (eg, 55%) cycling criteria. See Table 1 for the rise time and cycling criteria settings for each ventilator.
Rise Time and Cycling Criteria Settings
Prior to each trial, all ventilators were required to pass manufacturer recommended ventilator calibrations and circuit leak tests. Additionally, the same nonheated wire circuit (Hudson RCI, Research Triangle Park, North Carolina) was used for each trial on each ventilator. No in-line humidifiers were utilized during the study. Prior to collecting any data we initiated 12 stabilization breaths for each ventilator setting trial. Following the stabilization breaths, exhaled VT, TI, and peak flow measurements were recorded for 200 spontaneous breaths at each rise time and cycling criteria setting combination for the 4 ventilators. All exhaled VT, TI, and peak flow, and data for all trials were generated within the breathing simulator. Measurement results were then transferred from the breathing simulator to a spreadsheet (Excel, Microsoft, Redmond, Washington).
Statistical Analysis
We compared breath-by-breath analysis for minimum and maximum rise time and cycling criteria setting combinations within and between ventilator brands using one-way analysis of variance, and conducted post-hoc analysis with the Tukey test when necessary. To generate the difference between minimum and maximum mean values we used a paired t test. A P < .05 was considered statistically significant for all analyses. We used statistics software (SPSS, SPSS, Chicago, Illinois) for all data analysis.
Results
Table 1 reports the minimum and maximum rise time and cycling criteria settings available on the Avea, Evita XL, PB840, Esprit, LTV 1200, and Servo-i ventilators. Tables 2⇓–4 report the TI, exhaled VT, and peak flow changes that occurred for each rise time/cycling criteria combination. Data are expressed as mean ± standard deviation. Analysis of variance revealed significant differences for TI (P < .001), exhaled VT (P < .001), and peak flow (P < .001) on all 6 ventilators. Post hoc analysis using the Tukey test revealed significant differences between the means (P < .001) for most of the rise time/cycling criteria combinations across all 6 ventilators. Table 2 reports TI results in seconds for the rise time/cycling criteria combinations. Most rise time/cycling criteria combinations produced significant changes in TI, with few exceptions. The PB840 settings maximum-submaximum produced nonsignificant changes in TI, when compared to the Servo-i maximum-maximum (P > .99) and the LTV minimum-maximum (P > .99) settings. Other nonsignificant rise time/cycling criteria combinations reported on Table 2 include results between Esprit maximum-maximum and Esprit minimum-maximum (P = .98), between Servo-i maximum-maximum and LTV minimum-maximum (P = .94), and between Avea maximum-minimum and LTV maximum-minimum (P > .99).
Inspiratory Time at Pressure Support of 8 cm H2O*
Exhaled Tidal Volume at Pressure Support of 8 cm H2O*
Peak Flow at Pressure Support of 8 cm H2O*
Exhaled volume (mL) results are shown on Table 3. The Avea failed to produce significant changes in exhaled volume when comparing its maximum-maximum rise time/cycling criteria settings and its minimum-maximum settings (P = .98). The PB840 minimum-minimum settings produced nonsignificant changes in exhaled volume, when compared to the PB840 maximum-minimum (P > .99), Servo-i minimum-minimum (P > .99), Servo-i maximum-minimum (P > .99), and Esprit maximum-minimum settings (P = .55). The PB840 maximum-minimum settings also produced nonsignificant exhaled volume changes, when compared to the Servo-i maximum-minimum (P > .99) and Servo-i minimum-minimum settings (P = .72), and the Esprit maximum-minimum setting (P > .99). The Servo-i had nonsignificant results when comparing exhaled volume changes for its maximum-minimum setting and the Esprit maximum-minimum settings (P > .99). Other nonsignificant combinations include the comparison between Servo-i minimum-minimum settings and Esprit minimum-minimum (P = .75), and the combinations between the Esprit maximum-maximum and LTV minimum-minimum settings (P = .91).
Table 4 displays peak flow results for rise time and cycling criteria combinations for each ventilator. Although most settings adjustments produced significant changes in peak flow, there were a few results that were nonsignificant. The maximum-maximum rise time/cycling criteria setting for the Avea and the minimum-maximum and the minimum-minimum rise time/cycling criteria setting for the PB840 returned nonsignificant (P > .99 and P = .10, respectively) values for peak flow. Additionally, the minimum-minimum PB840 settings and the PB840 minimum-maximum settings were nonsignificant (P = .06) when reporting peak flow. Other nonsignificant combinations include the Servo-i minimum-minimum and Servo-i minimum-maximum (P = .26), and the combination of the Esprit minimum-minimum and the LTV maximum-maximum (P = .72).
Further assessment of Tables 2⇑–4 provides information on spontaneous parameter changes when holding constant the rise time or the cycling criteria. For example, when rise time was set to minimum for the PB840, a change in cycling criteria, from maximum to minimum, produced a change in exhaled VT of approximately 256 mL. This same scenario for the Servo-i produced a change in exhaled VT of approximately 156 mL, and for the Avea approximately 63 mL. We could not make a similar comparison for our Evita XL. Tables 2⇑–4 demonstrate that an adjustment in cycling criteria, from minimum to maximum, appears to have a bigger impact on exhaled VT and TI, versus making an adjustment in rise time from minimum to maximum. The opposite is true for peak flow.
Table 5 reports the mean differences between the lowest value and the highest value for TI, exhaled VT, and peak flow, based on the rise time/cycling criteria, combinations. These values were generated through paired t tests of the peak and trough mean values. The Esprit demonstrated the largest difference between minimum mean value and maximum mean value for exhaled VT. The Avea demonstrated the lowest difference in TI and peak flow when comparing the minimum mean value with the maximum mean value. The exhaled VT difference for the Avea was second lowest to the Evita XL. The Evita XL produced the biggest difference in peak flow and the second biggest change in TI, yet demonstrated the smallest change in exhaled VT.
Differences Between Mean Minimum and Mean Maximum Inspiratory Time, Exhaled Tidal Volume, and Peak Flow*
Table 6 reports the comparison of 2 pressure support levels for the Esprit ventilator. We found multiple nonsignificant differences when comparing TI at the 2 pressure support levels. For example, there was no significant difference between a pressure support of 7 cm H2O and a pressure support of 8 cm H2O for TI when comparing the maximum-maximum settings on the Esprit ventilator. This proved consistent with all rise time/cycling criteria combinations when assessing TI changes. The 2 pressure support levels demonstrated greater statistical significance when comparing VT and peak flow changes. The minimum-maximum combination for rise time/cycling criteria produced the only nonsignificant difference when assessing VT change. All rise time/cycling criteria combinations produced significant differences when assessing peak flow change between the 2 pressure support levels.
Inspiratory Time, Exhaled Tidal Volume, and Peak Flow of the Esprit Ventilator*
For all ventilators tested, the lowest TI value occurred at the maximum-maximum rise time/cycling criteria combination. For the Avea, PB840, and Servo-i the highest TI occurred at the minimum-minimum rise time/cycling criteria combination. A minimum-minimum rise time/cycling criteria combination was not available for the Evita XL. The Avea, PB840, and Servo-i generated the highest mean exhaled VT with the maximum-minimum rise time/cycling criteria combination. The Evita XL, PB840, and Servo-i generated the highest peak flow with the maximum-maximum rise time/cycling criteria combination. In contrast, the highest peak flow occurred at the maximum-minimum rise time/cycling criteria combination for the Avea.
Discussion
The primary aim of this study was to compare the differences in spontaneous parameters for each rise time/cycling criteria combination across 6 critical ventilators. For example, we wanted to compare the exhaled VT generated from a minimum-minimum rise time/cycling criteria combination on one ventilator to the exhaled VT generated from a maximum-maximum rise time/cycling criteria combination on the same ventilator. In addition, we wanted to compare the exhaled VT generated from a minimum-minimum rise time/cycling criteria combination on one ventilator to the exhaled VT generated from a minimum-minimum rise time/cycling criteria combination on the remaining ventilators. We examined the exhaled VT, TI, and peak flow changes that occurred with minimum and maximum rise time and cycling criteria settings, utilizing a test lung to simulate spontaneous breaths. As hypothesized, the results indicate statistically significant differences for most spontaneous parameters recorded with the above mentioned rise time/cycling criteria combinations. Equally, the results indicate statistically significant differences in most spontaneous parameters recorded for most rise time/cycling criteria setting combinations when comparing ventilators.
A secondary aim of this study was to communicate the differences between rise time and cycling criteria settings across 6 critical ventilators. Understandably, each manufacturer has developed rise time and cycling criteria settings to fit their particular ventilator and engineering specifications. Directionality and incremental settings for rise time and cycling criteria instrumentation vary substantially from ventilator to ventilator. For our study we described a minimum rise time as the slowest rise, measured in seconds, to the set inspiratory pressure level once the breath was initiated. When examining the rise time settings on each ventilator analyzed, the rise time settings may offer some confusion. For example, the minimum rise time setting for the Avea is 9, and the maximum rise time setting is 1. Conversely, the PB840 utilizes the smaller value of 1% as its minimum setting and the larger value of 100% as its maximum.
Rise Time
Although it may seem intuitive to the advanced critical care practitioner that changes in rise time and cycling criteria will cause variations in spontaneous parameters, there is no full text investigation comparing the possible changes on a variety of mechanical ventilators. Previous research has aimed to discuss the effects of rise time and cycling criteria, but has limited the dissemination to abstract form. Sollars et al7 published an abstract that examined the effects of rise time on peak flow, peak inspiratory pressure, and VT. The abstract revealed that faster inspiratory rise times increase peak flow and VT in patients utilizing pressure control ventilation. Although the reports appear similar to our research, they failed to outline the range of changes in these parameters that may occur on the ventilator. Additionally, the research was limited to 3 ventilators that were utilized during our research. Other abstracts published reported effects of rise time on volume delivery with patients in changing compliance, which is outside the focus of this paper.8 We chose to utilize one set compliance level so that variations in spontaneous parameters were due solely to changes in rise time and cycling criteria.
We demonstrated that rise time adjustments can directly impact spontaneous inspiratory parameters (eg, TI, peak flow, and exhaled VT) on a pressure supported breath, thus building upon the work of previous authors. A maximum rise time setting achieved a larger exhaled VT, compared to the minimum rise time setting, for the PB840, Servo-i, and Avea when cycling criteria was set to minimum. Thus, a rapid ascent to a set inspiratory pressure will result in a larger volume, compared to a slower ascent to the same pressure, when using a lung simulator. We recorded the peak flow and TI with all rise time/cycling criteria combinations and thus can verify the impact of both parameters on VT. A maximum rise time setting achieved a larger peak flow for the PB840, Servo-i, and Avea, compared to the minimum rise time setting, when rise time was set to minimum.
The explanation for a change in flow relates directly to the rise time setting. A maximum rise time setting allows for a faster initial flow, compared to the minimum setting. The TI with the maximum rise time setting decreased slightly, compared to the TI with the minimum rise time setting, for all 6 ventilators. During pressure support, inspiration will end once the peak flow degrades to a level determined by the cycling criteria. When rise time is set to a maximum level, the flow degrade will begin more quickly during the inspiratory phase, compared to a minimum rise time setting. Figure 1 demonstrates this phenomenon. Therefore, when rise time was set to minimum, the flow degrade was delayed due to the slow rise in the peak flow, and thus the TI extended slightly, compared to the TI with the maximum rise time setting.
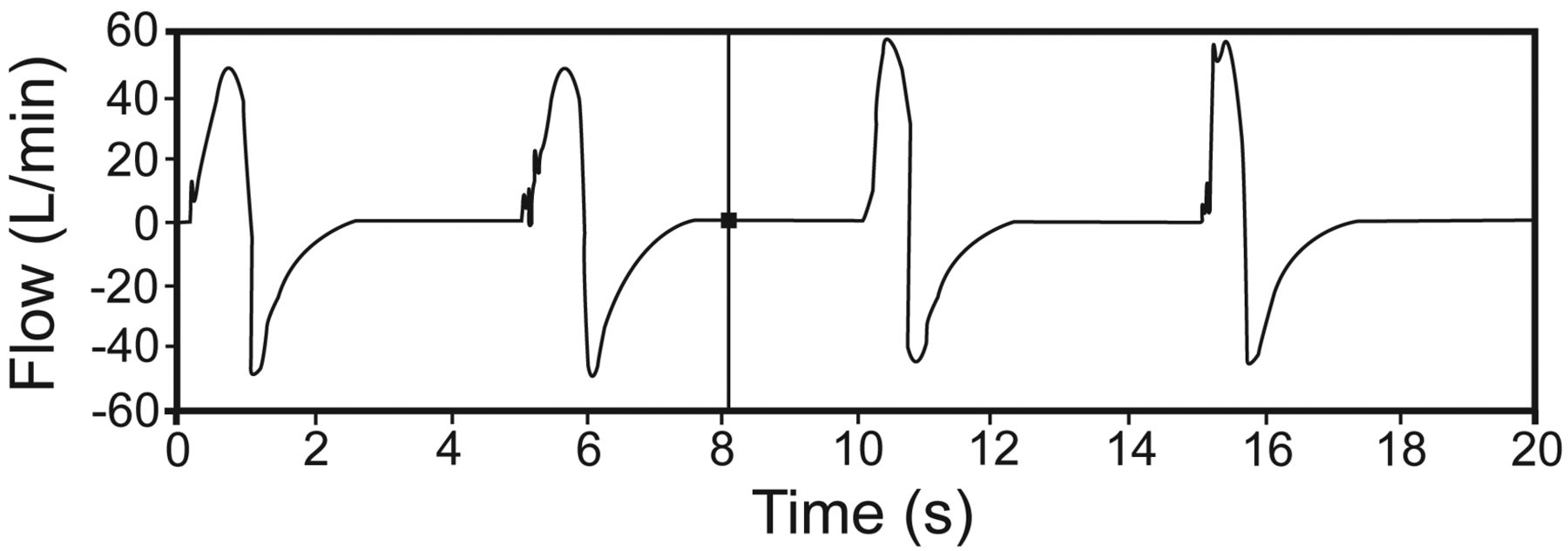
The changes in peak flow and inspiratory time between a minimum rise time (first 2 breaths) and a maximum rise time (last 2 breaths), with the Servo-i ventilator. The cycling criteria was set to maximum for all 4 breaths. The peak flow is lower and the inspiratory time is longer in the first 2 breaths, compared to the last 2 breaths.
Some of the ventilators we examined showed exhaled VT changes of up to 70 mL by simply increasing the rise time setting from its minimum setting to its maximum, without making any change in cycling criteria. The addition of a cycling criteria adjustment and rise time adjustment created exhaled VT changes in excess of 200 mL in 2 of the ventilators we tested. Changes in VT ultimately result in changes in minute ventilation, and could potentially impact decisions regarding a ventilator wean outcome. We believe the findings addressed above offer valuable information to the bedside clinician when contemplating the decision to adjust rise time.
Inspiratory Cycling Criteria
Various reports have discussed cycling criteria but addressed it only from a patient-ventilator asynchrony point of view.9,10 In a paper by Gentile, the effects cycling criteria have on premature cycling, intrinsic PEEP, trigger delay, and inspiratory effort were outlined.9 Gentile also reports the various cycling criteria names and settings from ventilator to ventilator, despite failing to provide the full range of cycling criteria on the PB840 (ie, 1–80%), and the upgraded cycling criteria parameters name and range on the Evita XL (inspiratory termination 5–70%). Tokioka et al11 demonstrated cycling criteria effects on work of breathing. In their research of 8 patients, increasing cycling criteria from 1% to 45% was shown to increase a patient's work of breathing by causing an increase in a patient's breathing frequency and a decrease in volume.11 Although their research produced results similar to our research, we chose to demonstrate the full range of changes that occur when adjusting cycling criteria from its minimal to maximal settings. We felt it is important to outline the entire scope of ranges that occur in exhaled VT, TI, and peak flow when changing rise time and cycling criteria from minimal to maximal settings.
We found a decrease in exhaled VT as cycling criteria was adjusted from minimum to maximum on each ventilator. Intuitively, we anticipated the maximum cycling criteria setting would correspond with the lowest VT. This proved correct on all 6 ventilators tested. A maximum setting for cycling criteria results in a flow cycle that is much closer to the peak flow level, versus a minimum cycling criteria setting. Figures 1 and 2 demonstrate this point. The end result of the maximum cycling criteria setting is a shorter TI and a lower VT. An interesting finding was the position for the lowest exhaled VT across the 6 ventilators when cycling criteria and rise time were considered. The PB840 and the Avea generated the lowest exhaled VT with a maximum cycling criteria and a minimum rise time. Conversely, the Evita XL and the Servo-i generated the lowest exhaled VT with a maximum cycling criteria and maximum rise time. This was an interesting discovery if we assume the cycling criteria setting functions exactly as defined above between each ventilator analyzed. We also anticipated finding the highest exhaled VT with a minimum cycling criteria setting and a maximum rise time setting. This proved correct for the PB840, Avea, and Servo-i ventilators. Since our Evita XL ventilator did not have the latest upgrade for cycling criteria, we could not make this comparison.

The changes in peak flow and inspiratory time between a minimum rise time (first 2 breaths) and a maximum rise time (last 2 breaths), with the Servo-i ventilator. The cycling criteria was set to minimum for all 4 breaths. The peak flow is lower and the inspiratory time is longer in the first 2 breaths, compared to the last 2 breaths.
A maximum cycling criteria setting suggests that inspiratory flow will terminate more quickly, thus producing less time in inspiration. In our opinion, knowledge related to the range of ventilator changes that occur by adjusting cycling criteria is critical to understanding optimal patient ventilation. Cycling criteria settings (also called inspiratory termination criteria, flow cycle percent, and expiratory sensitivity) vary greatly among ventilator manufacturers. The lack of uniform settings and various terminologies utilized by ventilator manufacturers to describe cycling criteria on the ventilator control panel could potentially confuse the bedside practitioner required to be proficient across multiple ventilators. When combining our findings with the research of other authors, the adjustment of cycling criteria and rise time could potentially impact breathing frequency, work of breathing, trigger timing, and patient-ventilator synchrony.11–15
We also changed the pressure support setting to compare the effects of rise time and cycling criteria on the 3 spontaneous parameters. We utilized the Esprit for this comparison. A pressure support change from 8 cm H2O to 7 cm H2O did not have a statistically significant impact on TI. This is understandable, since a change in the pressure setting should not impact the TI. A decrease in exhaled VT was expected with the decrease in pressure support; however, the magnitude of the change was unexpected. We did not see a consistent volume change across the rise time/cycling criteria combinations. The maximum-minimum rise time/cycling criteria combination produced a bigger change in exhaled VT, versus the minimum-minimum combination. The changes we found further demonstrate the impact rise time and cycling criteria have on VT. The peak flow changes were also statistically significant and much more consistent across the rise time/cycling criteria combinations. Since we were using a test lung, we did not expect to see big changes in peak flow with a change in pressure support, since inspiratory flow is partially determined by the patient during pressure-based modes. The reduction in peak flow associated with the decrease in pressure support is probably a result of the lower pressure setting.
We demonstrated the impact that rise time and cycling criteria have on spontaneous parameters during pressure support ventilation using a test lung. We find this information to be important for a number of reasons. First, it provides the bedside clinician with specific knowledge related to the usefulness of these parameters. The clinician has the ability to impact all 3 spontaneous parameters (ie, exhaled VT, TI, peak flow) when using pressure support. All 3 parameters are obviously important. For example, improvements in the frequency/VT during spontaneous breathing trials may occur without increasing pressure support. Adjusting rise time toward the maximum setting and cycling criteria toward the minimum setting may produce the biggest VT and potentially a lower frequency/VT ratio. TI is not a direct setting during pressure support ventilation.
Several of the ventilators produced TI over 1.5 seconds when cycling criteria was set to minimum. In the event that a patient prefers a shorter TI, the cycling criteria can be adjusted toward maximum to produce a shorter TI. Second, to the bedside clinician, medical educator, and student this information provides specific numbers to demonstrate the impact of adjusting rise time and cycling criteria. The names of these 2 controls (ie, rise time and cycling criteria) describe their immediate function and lend no information on the parameters they impact. The results from this study offer additional description of the benefits of adjustment of the rise time and cycling criteria. Third, each manufacturer programs a default value for rise time and cycling criteria at ventilator start-up. It is likely that many bedside clinicians overlook these controls, with the assumption that the default is the ideal setting. We hope the results of this study encourage the bedside clinician to make adjustments in rise time and cycling criteria, with the understanding that spontaneous parameters can change based on the rise time and cycling criteria settings.
Limitations
Although statistically significant differences (P < .05) in the reported parameters occurred when making minimum and maximum rise time and cycling criteria setting changes, the differences may or may not represent clinically important changes. The study was conducted in a ventilator lab using a breathing simulator; therefore, the clinical importance of a change in spontaneous parameter due to a change in rise time and/or cycling criteria requires evaluation on actual patients.
Another limitation of this study pertains to the pressure support setting we selected. We based our decision on available literature demonstrating a pressure support of 8 cm H2O as a viable level for intubated patients breathing spontaneously. We wanted to show the impact of cycling criteria and rise time changes when used in conjunction with an acceptable pressure support level. We demonstrated that a different pressure support setting would generate different minimum and maximum monitored values with the Esprit ventilator. However, we were unable to assess the impact of a lower pressure support setting with the other ventilators included in this study.
Additionally, we were unable to obtain upgraded software for the Evita XL that allows for a variable cycling criteria, versus the fixed cycling criteria utilized in this research. Financial restrictions prohibited the purchase of upgraded software and hardware for this study. The upgraded 7.02 Evita XL software labels cycling criteria as inspiratory termination and offers a range of 5–70%.
Finally, we chose not to report work of breathing as part of this research project. Previous research has suggested that incremental adjustment of rise time and cycling criteria can prevent an increase in airway pressure at end inspiration, and may reduce inspiratory work load and provide better synchrony between the ventilator and the patient.1,16,17 The direction of our research was to outline the range of changes that occur with minimal and maximal rise time and cycling criteria settings. Further research will need to be conducted to report the changes in work of breathing with minimal and maximal rise time and cycling criteria settings.
Conclusions
We chose to examine the minimal and maximal rise time and cycling criteria settings as a way to demonstrate the full potential of each setting on the spontaneous parameters reported above (ie, exhaled VT, TI, peak flow). We reported the exhaled VT, TI, peak flow changes following a rise time and cycling criteria adjustment as a way to compare 6 critical care ventilators using a test lung. We believe there is a need for additional research in this area, due to its direct translational value to the bedside clinician. Future research to determine the impact of rise time and cycling criteria on spontaneously breathing patients in pressure support mode is warranted.
Footnotes
- Correspondence: Joshua F Gonzales MHA RRT-NPS, Department of Respiratory Care, Texas State University–San Marcos, 601 University Drive, San Marcos TX 78666. E-mail: jg61{at}txstate.edu.
Mr Gonzales presented a version of this paper at the International Conference of the American Thoracic Society, held May 13–18, 2011, in Denver, Colorado.
The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}