

Abstract
BACKGROUND: Selection of the PEEP associated with the best compliance of the respiratory system during decremental PEEP titration can be used for the treatment of patients suffering from ARDS. We describe changes in transpulmonary pressure (Ptp) and gas exchange during a decremental PEEP titration maneuver in subjects with pulmonary ARDS.
METHODS: Eleven subjects with early ARDS were included. After a recruitment maneuver they were ventilated in volume-controlled ventilation and PEEP was decreased from 30 to 0 cm H2O by steps of 3 cm H2O. Static airway pressure (Paw), esophageal pressure (Pes), Ptp (Paw – Pes), the ratio of dead space to tidal volume (VD/VT), and PaO2 were recorded at each step.
RESULTS: A linear correlation was found between Paw and Ptp. Expiratory Ptp became negative in all subjects when PEEP decreased below 8.9 ± 5.2 cm H2O. VD/VT was 0.67 ± 0.06 with 30 cm H2O of PEEP, and decreased 15.4 ± 8.5% during the maneuver, when PEEP and expiratory Ptp were 10.6 ± 4.1 cm H2O and 1.2 ± 2.8 cm H2O, respectively. VD/VT was significantly higher during ventilation at high (> 18 cm H2O), compared to low, inspiratory Ptp values (P < .001). PaO2 decreased when expiratory Ptp became negative (P < .001).
CONCLUSIONS: During decremental PEEP titration we sequentially observed high inspiratory Ptp that stressed lung tissue and increased VD/VT, and negative Ptp, indicating high risk of alveolar collapse, explaining worse oxygenation. PEEP selection based on Ptp and VD/VT in ARDS may help to avoid these situations.
Introduction
Mechanical ventilation (MV) in ARDS is usually performed with small tidal volume (VT) and moderate to high levels of PEEP. Several methods to individualize PEEP setting have been proposed to optimize lung mechanics and to improve gas exchange while reducing ventilator-induced lung injury, which has been related to the stress and the strain applied to the lungs during MV.1–8 Stress depends on the transpulmonary pressure (Ptp), which is the difference between alveolar pressure and pleural pressure, while strain refers to the relationship between tidal change and end-expiratory lung volumes.9 Cyclic opening and closing of alveolar units have also been related to ventilator-induced lung injury.10 PEEP level and resulting expiratory and inspiratory Ptp during MV may affect all these mechanisms of injury.
The PEEP associated with the best compliance of the respiratory system (CRS) can be easily found at the bedside during a decremental PEEP titration maneuver. This procedure has been proposed as a way to individualize PEEP setting.2 It may be possible to observe a change in Ptp and the ratio of dead space (VD) to VT when PEEP is progressively decreased from high to low levels. These behaviors have not been well described in clinical settings. The purpose of this study is to describe changes in Ptp and VD/VT during decremental PEEP titration performed in a group of subjects with ARDS due to severe pneumonia.
QUICK LOOK
Current knowledge
In patients with ARDS, PEEP selection can be based on respiratory mechanics, oxygenation, and/or hemodynamic criteria. The optimum PEEP and best method to set PEEP are controversial. One method includes using the best respiratory system compliance during decremental PEEP titration.
What this paper contributes to our knowledge
The recording of transpulmonary pressure instead of airway pressure and the ratio of dead space to tidal volume during a decremental PEEP trial appears to allow an individualized approach for optimal PEEP setting. Negative transpulmonary pressure was associated with hypoxemia suggesting lung collapse, whereas high transpulmonary pressure increased the ratio of dead space to tidal volume that may be related to alveolar overdistension.
Methods
This study was approved by our internal review board and was conducted in our 19 bed ICU at the Centro de Educación Médica e Investigaciones Clínicas in Buenos Aires, Argentina. Informed consent was obtained from all subjects' next of kin before inclusion.
Subjects and Procedures
Eleven consecutive patients suffering from ARDS, according to the American-European Consensus Conference on ARDS, due to severe pneumonia, were included within 72 hours of admission to the ICU, between May 2009 and May 2010.11 All subjects' hemodynamic condition was judged stable before procedures. They were ventilated with a Puritan Bennett 840 (Covidien, Mansfield, Massachusetts) or a Servo-i (Maquet, Wayne, New Jersey) ventilator in volume-controlled continuous mandatory ventilation, with a VT of 6 mL/kg of ideal body weight, FIO2 of 1.0, and breathing frequency between 25 and 30 breaths/min. A humidifier (MR850, Fisher & Paykel Healthcare, Auckland, New Zealand) was used for inspiratory gas conditioning in all cases. The subjects were in semi-recumbent position, with the head of the bed elevated at 30°, and sedated with midazolam and fentanyl. Neuromuscular blockade with atracurium was used as needed. Secretions were suctioned before the start of the study protocol. After a recruitment maneuver using CPAP of 40 cm H2O for 40 seconds, volume-controlled ventilation was resumed and PEEP was decreased from 30 to 0 cm H2O by steps of 3 cm H2O every 3 min (see Fig. 1). An inspiratory plateau airway pressure higher than 60 cm H2O, a reduction of SpO2 below 85%, a mean arterial pressure lower than 60 mm Hg, or a sudden change in cardiac rhythm were used as criteria for interrupting the decremental PEEP titration maneuver.
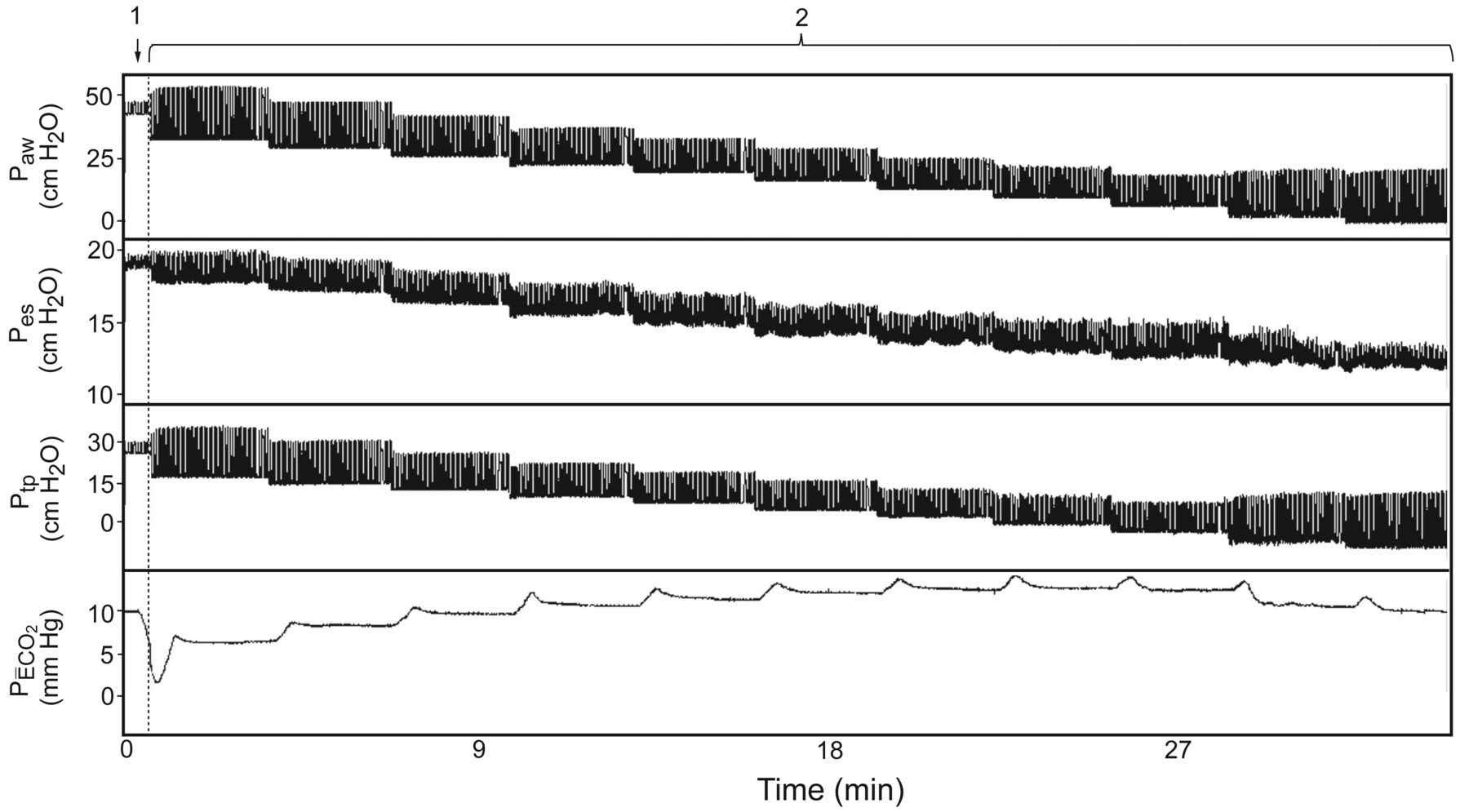
Study procedures. Tracings from subject 8, showing airway pressure (Paw), esophageal pressure (Pes), transpulmonary pressure (Ptp), and mixed expiratory PCO2 (PĒCO2). First a recruitment maneuver was performed, using a CPAP of 40 cm H2O for 40 seconds. Then volume-controlled ventilation was resumed and PEEP was decreased from 30 to 0 cm H2O by steps of 3 cm H2O every 3 min. See how the PĒCO2 signal stabilizes by the end of each PEEP step.
Measurements
Flow was measured with a pneumotachograph (TSD137G, ± 3000 mL/s, Biopac Systems, Goleta, California) at the Y-piece. Airway pressure (Paw) at the Y-piece, and esophageal pressure (Pes) obtained from a 7 cm long latex balloon inflated with 1 mL of air were recorded using transducers (TSD160D, ± 75 cm H2O, Biopac Systems, Goleta, California). The esophageal balloon position, between the middle and the distal third of the esophagus to minimize cardiac artifacts, was verified with a chest x-ray before measurements. Data acquisition and analysis were done with an MP100WSW system and AcqKnowledge 3.9.0 (Biopac Systems, Goleta, California), respectively. Inspiratory VT was integrated from the flow signal. Recordings were performed during the last minute of each step, using an expiratory and an inspiratory pause of 2 seconds, synchronized with the PR interval on electrocardiographic tracing to avoid cardiac artifacts on Pes (Fig. 2). Ptp was calculated as the difference between Paw and Pes. CRS, lung compliance (Clung), and chest wall compliance (CCW) were calculated using standard formulae, and VD/VT with the Bohr-Enghoff equation12:

Influence of cardiac artifact on esophageal pressure recording. Tracings from subject 5, showing airway pressure (Paw), transpulmonary pressure (Ptp), esophageal pressure (Pes), and electrocardiogram (ECG). Note that the Pes signal shows swings of 2–3 cm H2O, related to cardiac activity. To standardize the measurements, end-expiratory static pressure (arrow 1) and end-inspiratory static pressure (arrow 2) recordings were performed during PR intervals.
Statistical Analysis
Linear regression analysis between Paw and Ptp or Pes was performed. The PEEP value where expiratory Ptp became negative was interpolated from each subject's data, assuming that both variables have a linear relationship. To perform this interpolation we calculated for each subject the linear equation linking expiratory Ptp as the dependent variable and PEEP as the independent variable, using data points above and below the X axis. Finally, we calculated the PEEP value corresponding to an expiratory Ptp of 0. The best CRS PEEP was defined as the highest value of PEEP producing the higher CRS during the decremental titration maneuver.
Receiver operating characteristic curves were built to evaluate the performance of plateau inspiratory Paw for the detection of stressful ventilation (inspiratory Ptp higher than 25 cm H2O). The Paw associated with the greatest sensitivity and specificity was obtained. Additionally, the sensitivity and specificity of a Paw of 30 cm H2O for predicting a Ptp higher than 25 cm H2O were also calculated with standard formula.
Analysis of variance (ANOVA) for repeated measurements was performed to evaluate the effect of PEEP on compliances, VD/VT, and PaO2. To evaluate the effect of Ptp (grouped in intervals of 3 cm H2O) on these 2 variables, a 2-way ANOVA test was performed using each subject as a block to control interindividual variability, and Ptp as a random factor. Post hoc comparisons were made with the Bonferroni test. Continuous variables are expressed as mean ± SD. A P value less or equal to .05 was considered statistically significant. Statistics software (PASW 18.0.0, SPSS, Chicago, Illinois) was used.
Results
All subjects had ARDS due to community-acquired pneumonia, 5 secondary to H1N1 2009 influenza virus. Mean age and Acute Physiology and Chronic Health Evaluation II were 50 ± 19 years and 20 ± 9, respectively. In all cases chest x-rays showed diffuse pulmonary infiltrates. Baseline MV settings, gas exchange before recruitment maneuver, and outcomes are shown in Table 1. The maneuver could be completed in all cases without signs of major hemodynamic impairment or barotrauma.
Baseline Characteristics and Outcomes (n = 11)
Respiratory System Mechanics
During decremental PEEP titration, as PEEP decreased from 30 cm H2O, mean CRS initially increased until reaching a peak, and then decreased (ANOVA P < .001, Fig. 3). The best CRS PEEP was achieved with a mean PEEP of 10.4 ± 3.1 cm H2O (see Table 1). This behavior was also observed with Clung (see Fig. 3, ANOVA P < .001), while CCW was not significantly affected by PEEP (ANOVA P = .09).
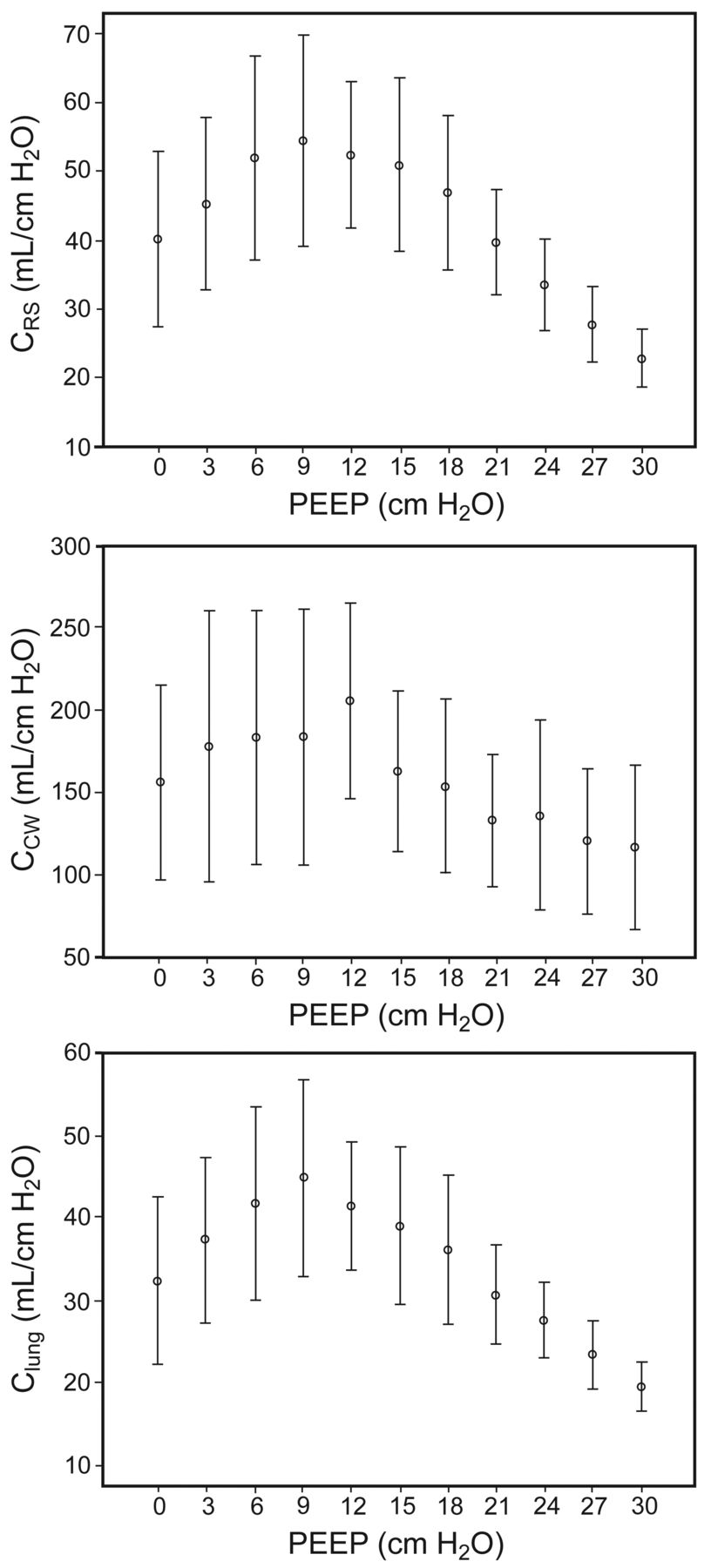
PEEP versus static compliance of the respiratory system (CRS), chest wall (CCW), and lung (Clung) during a decremental PEEP titration maneuver. CRS and Clung significantly improved as PEEP was decreased (P < .001), while CCW was not affected (P = .09). The error bars represent ± 1 standard deviation.
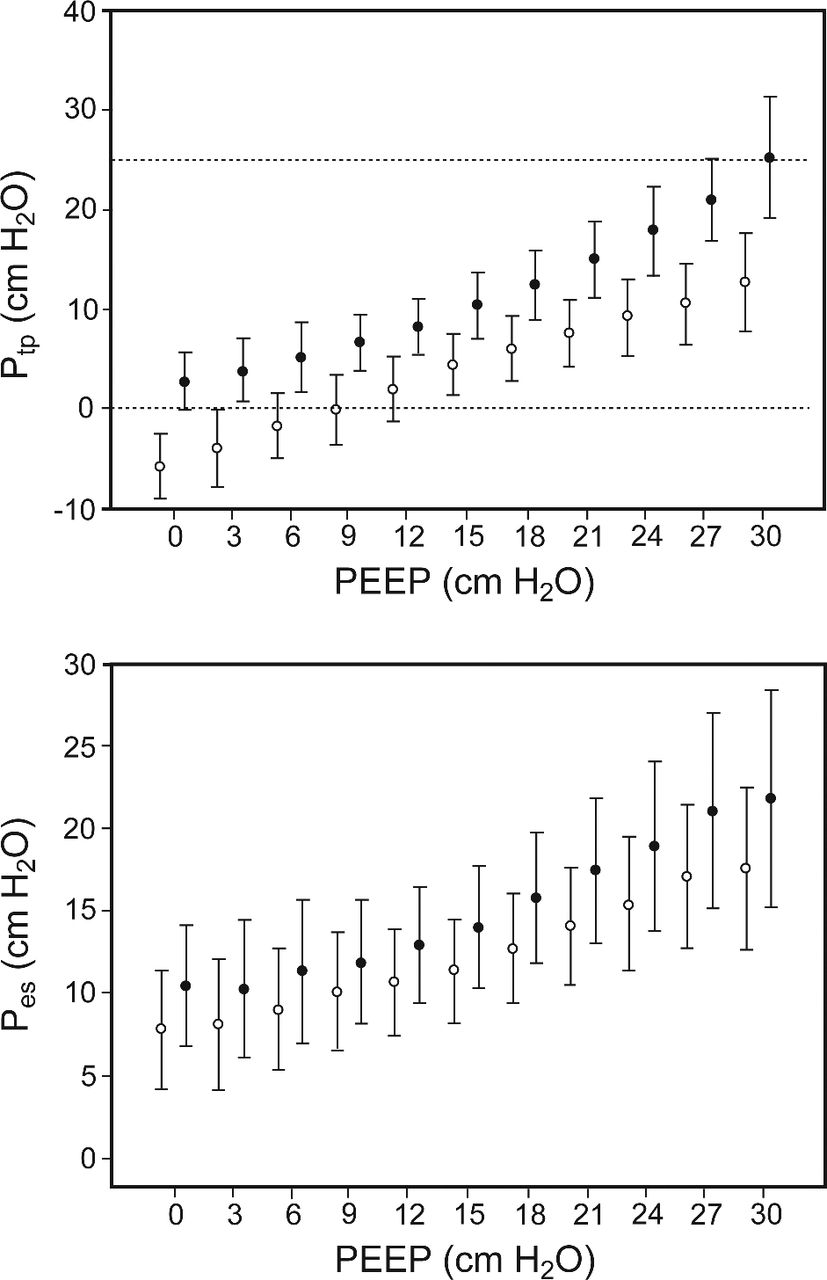
Figure 4 summarizes the effect on Ptp and Pes produced by PEEP reduction. A significant correlation was found between both inspiratory and expiratory Paw and Ptp (R2 = 0.76, P < .001, and R2 = 0.73, P < .001, respectively). Pes and Paw also showed a linear relationship both during expiration (R2 = 0.46, P < .001) and inspiration (R2 = 0.56, P < .001). As is shown in Table 2, the PEEP where expiratory Ptp equaled 0 could be interpolated in all subjects, with a mean value of 8.9 ± 5.2 cm H2O (range 0.9–20.1). This value was not significantly different, when compared to the best CRS PEEP (paired t test P = .35). Maximal individual recorded inspiratory and expiratory Ptp were 25.6 ± 5.9 cm H2O (range 14.4–33.2 cm H2O) and 13.0 ± 4.8 cm H2O, respectively. Inspiratory Paw was higher than 30 cm H2O in 41 out of 121 recordings (33.9%). In 8 (19.5%) of these 41 measurements, inspiratory Ptp was above 25 cm H2O. On the other hand, inspiratory Ptp was below that threshold in all cases when Paw was equal or lower than 30 cm H2O. Thus, a Paw higher than 30 cm H2O had a sensitivity of 1.0 and specificity of 0.71 for the detection of an inspiratory Ptp higher than 25 cm H2O. A Paw higher than 37.7 cm H2O showed the greatest combination of sensitivity (1.0) and specificity (0.86) for the detection of an inspiratory Ptp higher than 25 cm H2O (area under the receiver operating characteristic curve 0.93, P < .001).
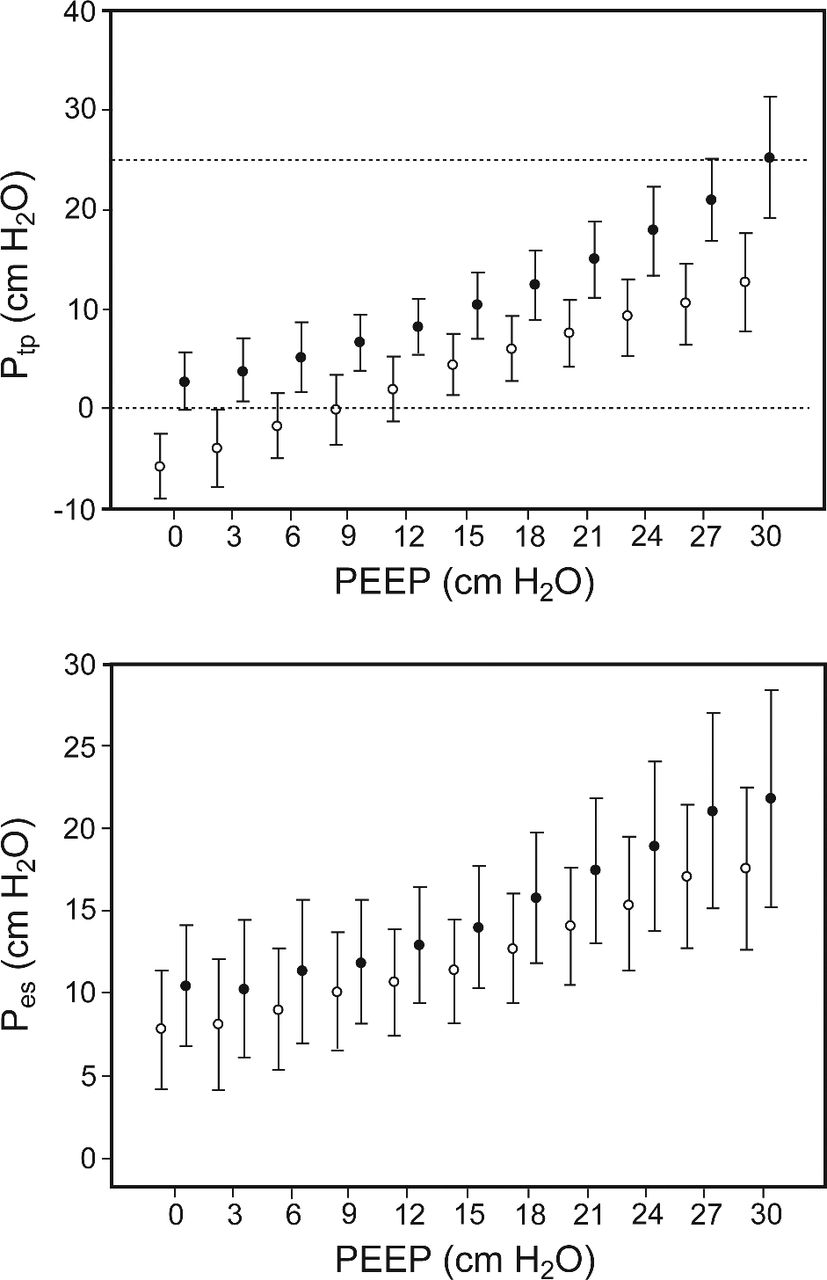
PEEP versus static transpulmonary pressure (Ptp) and esophageal pressure (Pes) during a decremental PEEP titration maneuver. Recordings were performed during inspiration (shaded circles) and expiration (white circles). The error bars represent ± 1 standard deviation.
PEEP Corresponding to the Best Compliance of the Respiratory System During Decremental PEEP Titration, PEEP Value Interpolated at Expiratory Transpulmonary Pressure Equal to Zero, Ratio of Dead Space to Tidal Volume, and PaO2 With a PEEP of 30 cm H2O Following Recruitment Maneuver
Gas Exchange
During the decremental maneuver, as PEEP was reduced from 30 to 0 cm H2O, PaCO2 progressively decreased from 57.4 ± 10.6 to 52.9 ± 7.6 mm Hg, respectively (ANOVA P < .001). VD/VT was 0.67 ± 0.06 during ventilation with 30 cm H2O of PEEP (see Table 2). From that value, VD/VT decreased to 15.4 ± 8.5% during the stepwise reduction of PEEP (ANOVA P < .001, Fig. 5A). This peak reduction of VD/VT was observed with a PEEP of 10.6 ± 4.1 cm H2O, which was associated with a Ptp of 1.2 ± 2.8 cm H2O and 7.6 ± 2.8 cm H2O during expiration and inspiration, respectively. VD/VT was also affected by expiratory and inspiratory Ptp (ANOVA P < .001, see Figs. 5B and 5C). Compared to lower inspiratory Ptp intervals, when this pressure was higher than 18 cm H2O, VD/VT was significantly increased (Bonferroni test).

Mean ratio of dead space (VD) to tidal volume (VT) versus PEEP and transpulmonary pressure (Ptp) during decremental PEEP titration maneuvers. VD/VT significantly changed when PEEP was decreased from 30 cm H2O (P < .001). Ptp is grouped in 3 cm H2O intervals. VD/VT was significantly affected by both inspiratory and expiratory Ptp (both P < .001). The error bars represent ± 1 standard deviation. Post hoc comparison P < .05 for multiple comparisons with a PEEP of 30 cm H2O (*), and for multiple comparisons with a PEEP of 12 cm H2O (†). Post hoc comparison P < .05 for multiple comparisons with the 3.01–6.00 cm H2O expiratory Ptp interval (‡), and for multiple comparisons with the 9.01–12.00 cm H2O inspiratory Ptp interval (§).
PaO2 was 225.7 ± 108.8 mm Hg with a PEEP of 30 cm H2O, and it changed as PEEP was reduced to 0 cm H2O (see Table 2 and Fig. 6A, ANOVA P = .02). Post hoc comparisons between PEEP levels disclosed no significant differences. Figures 6B and 6C illustrate how expiratory and inspiratory Ptp also exerted changes in PaO2 (ANOVA P < .001). Post hoc comparison between intervals showed that those including negative expiratory Ptp were associated with lower PaO2.

Mean PaO2 versus PEEP and transpulmonary pressure (Ptp) during decremental PEEP titration maneuvers. PaO2 significantly changed during PEEP decrease (P < .02). Ptp is grouped in 3 cm H2O intervals. PaO2 was significantly affected by both inspiratory and expiratory Ptp (both P < .001). The error bars represent ± 1 standard deviation. Post hoc comparison P < .05 for multiple comparisons with expiratory Ptp intervals higher than 3 cm H2O (*), and with inspiratory Ptp intervals higher than 9 cm H2O (†).
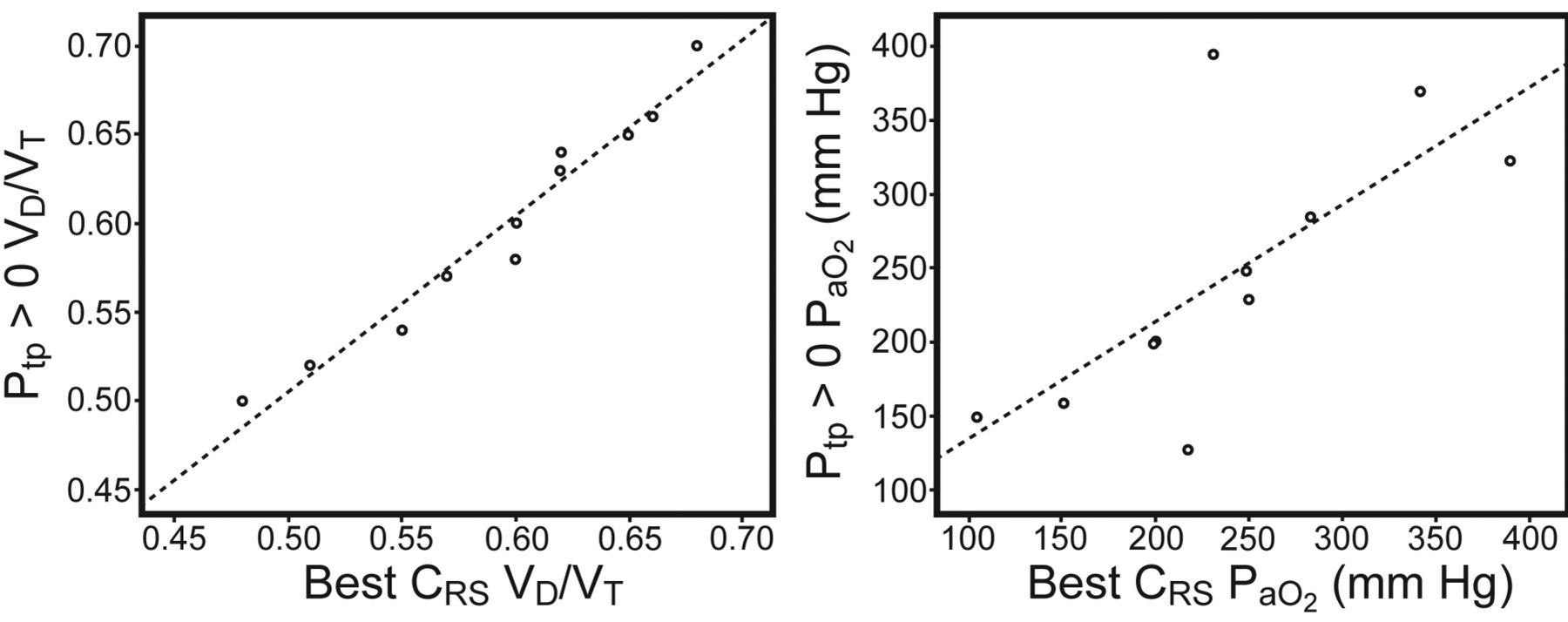
As shown in Figure 7, VD/VT observed during ventilation with the best CRS PEEP showed an excellent correlation with values recorded with the minimal PEEP required to obtain a positive expiratory Ptp (R2 = 0.96, P < .001). Comparison of PaO2 between these 2 PEEP values showed a good correlation (R2 = 0.51, P = .14).
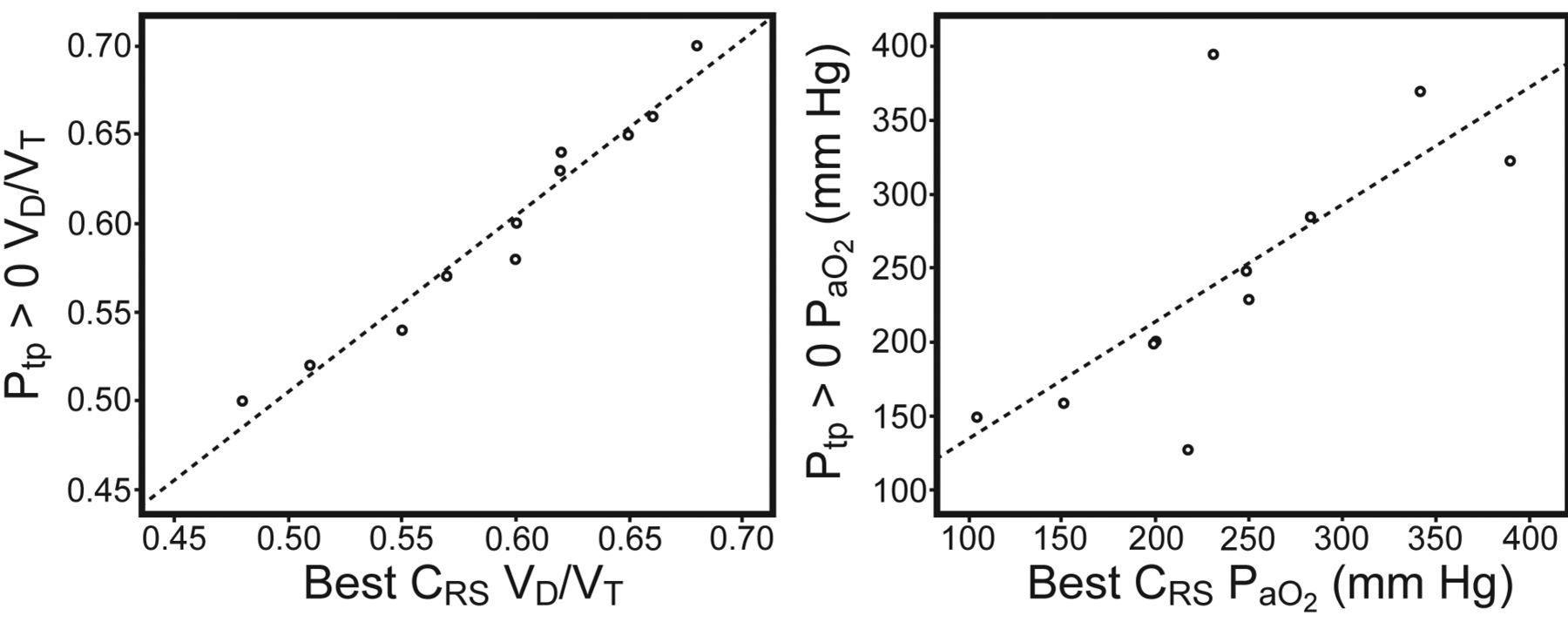
A: Ratio of dead space (VD) to tidal volume (VT) with the PEEP corresponding to the best compliance of the respiratory system (best CRS) versus that with the minimal PEEP required to obtain a positive expiratory transpulmonary pressure (Ptp) > 0. B: PaO2 with the PEEP corresponding to the best compliance of the respiratory system (best CRS) versus that with the minimal PEEP required to obtain a positive expiratory Ptp > 0..
Discussion
This study describes the behavior of Ptp, VD/VT, and PaO2 during a decremental PEEP titration maneuver performed to detect the PEEP level resulting in the best CRS. Our main findings are:
All subjects showed negative expiratory Ptp at some point of the decremental PEEP titration maneuver.
An upper inspiratory plateau Paw limit of 30 cm H2O was not an accurate predictor of potentially injurious high Ptp following a recruitment maneuver.
Gas exchange was affected by Ptp during decremental PEEP titration. VD/VT was mainly increased during ventilation with high inspiratory Ptp, whereas PaO2 decreased when expiratory Ptp became negative.
Setting PEEP to get the best CRS has been used as a way to optimize cardiopulmonary function since early ARDS studies.5 We performed a decremental PEEP maneuver using high expiratory and inspiratory Paw in order to enhance the likelihood of lung recruitment, as it has been previously suggested.13 CRS and Clung were both affected by PEEP in this group of pulmonary ARDS subjects, suggesting that our subjects had recruitable lung units, as has been described in tomographic studies.14 The greatest improvements were observed with moderate levels of PEEP (mean of 10 cm H2O) during the maneuver. On the other hand, PEEP did not significantly affect CCW. This has been previously reported in patients with pulmonary and extrapulmonary ARDS.8
Effect of Decremental PEEP Titration on Transpulmonary Pressure
During the decremental maneuver all of our subjects exhibited negative Ptp, which was calculated as the difference between Paw and Pes. Traditionally, Pes has been used as a surrogate of pleural pressure in respiratory physiology, although disagreements between both measurements have been recognized.15 Factors such as lung volume, compression by the mediastinum, and pleural recording site may explain these differences.15,16 To overcome this problem, authors have suggested performing a correction in Ptp calculation, adding an arbitrary value of cm H2O based on changes observed in Pes after body position modification in healthy subjects.16,17 We did not perform such correction in our calculations because, to our knowledge, there are not enough data about this point in ARDS patients, and we considered that our esophageal recording might estimate pleural pressure between the middle to the more dependent lung regions, as has been suggested in an experimental ARDS model.18 As expected, during the decremental PEEP titration maneuver, inspiratory and expiratory Paw and Ptp showed good correlation. Expiratory Ptp became negative when PEEP was decreased below 1 to 20 cm H2O (average 9 cm H2O). Negative Ptp has been previously described in ARDS patients despite the application of high PEEP, and this has been associated with low CCW.17,19 The observation of negative Ptp probably represents a miscalculation, because Pes might reflect pleural pressure at a given point surrounding dependent lung regions, while Paw only stresses opened alveolar units. The vertical pressure gradient between pleural pressure surrounding these ventilated units and Pes seems to be a function of interposed lung weight.18,20 In other words, when low PEEP is applied, alveoli and small airway may close, at least during exhalation, causing alveolar gas trapping and/or atelectasis. Under these circumstances the static Paw may not reflect the true alveolar pressure. Indeed the high Pes could be more representative of the end-expiration alveolar pressure in these poorly ventilated units. These considerations may explain why PEEP interpolated at expiratory Ptp 0 was highly variable among our subjects and hardly predictable without other tools such as chest computed tomography scans.18,20 These values were not significantly different from the best CRS PEEP. However, our data suggest that ventilating with the best CRS PEEP based on a decremental PEEP titration maneuver may not always avoid the risk of lung collapse and the tidal cyclic opening and closing of lung units, because some patients will have negative Ptp, as was observed in 4 cases of our series (see Table 2).
Traditionally, static Paw has been used as a surrogate of stress applied to alveolar units. Excessive stress on lung tissue during MV has been implicated in capillary and alveolar barrier disruption (stress failure) and in enhancing systemic inflammation.21,22 From a mechanistic point of view, alveolar transmural pressure (static airway minus pleural pressure) is a more accurate stress parameter than airway opening pressure itself. Nevertheless, keeping static plateau inspiratory Paw below 30 cm H2O during ARDS ventilation has been recommended to avoid ventilator-induced lung injury, and this threshold has been evaluated as an objective for PEEP titration, aiming to increase recruitment.3,4,23 Ptp may be a more accurate predictor of the real alveolar transmural pressure because it is not influenced by chest wall mechanics.17,24 In fact, although the sensitivity for the detection of an inspiratory Ptp higher than 25 cm H2O (which represents the expected value at total lung capacity in subjects with normal lungs) of an inspiratory Paw greater than 30 cm H2O was 1.0, its specificity was only 0.71. Moreover, in this series a Paw equal to or higher than 37.7 cm H2O was identified as the best cutoff value for predicting an inspiratory Ptp exceeding 25 cm H2O. Taken together these results strongly suggest measuring Pes and calculating Ptp for setting MV in patients at risk of having decreased CCW, including patients with pulmonary ARDS.
Gas Exchange Variations During Decremental PEEP Titration
VD/VT is increased in ARDS patients and has prognostic value because it reflects microvascular disruption and ventilation inhomogeneity. It has been suggested that different PEEP levels do not affect VD/VT of lung injured subjects.25 According to our data, after a recruitment maneuver, VD/VT decreased during decremental PEEP titration, indicating that very high PEEP levels may overstress alveolar units and jeopardize lung perfusion. Another explanation, suggested by a previous study, is that high inspiratory Paw may only increase airway VD/VT partition measured by volumetric capnography.26 In contrast with our observations, in this study involving acute lung injury patients where PEEP was increased from 0 to 15 cm H2O, respiratory system mechanics and PaO2 were not improved by PEEP, indicating that there was no lung recruitment. An experimental study using a highly recruitable animal model and volumetric capnography found that alveolar VD/VT may be improved by moderate to high levels of PEEP.27
However, in our study the highest VD/VT values were observed when inspiratory Ptp exceeded 18 cm H2O, suggesting that high Ptp may enhance ventilation-perfusion mismatching. PaO2 was also affected by variations of PEEP and expiratory Ptp during a decremental titration maneuver. Comparisons between PEEP levels were not significantly different in post hoc analysis. This finding may be explained by the short equilibration time (3 min) between PEEP steps during the maneuver. However, PaO2 significantly decreased when expiratory Ptp became negative, probably due to alveolar unit collapse and increased shunt fraction. This observation linking negative expiratory Ptp (and not specific PEEP levels) and worse oxygen exchange may be considered when evaluating the potential for recruitment of lung units.14,20,28 Additionally, our findings also indicate that expiratory Ptp may be used for PEEP titration, as has been suggested by Talmor et al.6 Nevertheless, in this scenario, quantification of VD/VT may add to the identification of an excessive pressure setting.
VD/VT recorded with the best CRS PEEP was highly correlated with its value during ventilation, with the minimal PEEP producing a positive expiratory Ptp. PaO2 also showed a good correlation between these 2 PEEP values. These observations suggest that PEEP titration during a decremental maneuver may provide short-term gas exchange comparable to a strategy aiming to get a positive expiratory Ptp. However, as has been stated above, best CRS PEEP produced negative expiratory Ptp in some patients. The latter may explain why gas exchange benefits obtained with the best CRS approach are not always sustained in the long term.29
This study has some limitations. Our subjects had diffuse ARDS due to severe pneumonia, so these findings should not be generalized to other ARDS etiologies. Second, the occlusion maneuver has been recommended to evaluate the accuracy of Pes recordings.30 We did not perform this validation. This test was originally described to verify the quality of Pes measurements in spontaneously breathing subjects.31 A modified maneuver has been validated in sedated patients with normal lungs, and also in COPD and ARDS patients.32–34 One potential pitfall of this occlusion test in a heavily sedated ARDS patient would be produced by inadvertent airway position of the esophageal catheter. We had observed (unpublished data) this problem in one case before initiating the present study. Thus, we routinely verified the position of the catheter with a chest-x-ray to avoid that issue. Third, PEEP steps during the maneuver lasted 3 min. This short time might have been insufficient to reach a steady state in gas exchange variables.35 Fourth, VD/VT was calculated using mixed PĒCO2, measured from a mixing chamber, instead of using volumetric capnography. Both methods provided similar results when comparing physiological VD/VT in ARDS patients.36 However, volumetric capnography also allows partitioning of VD/VT into its airway and alveolar components. These parameters may be of interest for the understanding of the relationship between lung mechanics and dead-space ventilation. Finally, measurements were performed during derecruitment, so mechanical behavior was actually influenced by previous recruitment history. Even in the absence of solid evidence, recruitment maneuvers are usually performed to improve gas exchange and to increase Clung.29 Thus, both expiratory and inspiratory Ptp values observed in our study may be lower than those expected during an incremental PEEP titration maneuver.2
Conclusions
In this study describing mechanics and gas exchange during decremental PEEP titration in pulmonary ARDS, we observed that PaO2 decreased with negative expiratory Ptp, indicating lung collapse. On the other hand, a higher VD/VT was observed with high inspiratory Ptp, possibly related to alveolar overdistention. Although the best compliance PEEP selection approach may be useful in some cases, accurately predicting these Ptp lower and upper limits is difficult when only airway measurements are considered. Keeping MV within these boundaries may be of clinical interest in order to reduce ventilator-induced lung injury in ARDS patients. Further studies focused on clinical outcome are required to demonstrate the impact of a more individualized ventilator setting protocol guided by a multimodal monitoring strategy including esophageal pressure and VD/VT measurements.
Footnotes
- Correspondence: Pablo O Rodriguez MD, Servicio de Terapia Intensiva, CEMIC, Avenida Las Heras 2900, C1425ASS, Buenos Aires, Argentina. E-mail: prodriguez{at}cemic.edu.ar.
Dr Rodriguez presented a version of this paper at the annual congress of the Sociedad Argentina de Terapia Intensiva, held September 30 through October 3, 2010, in Mar del Plata, Argentina, and at the European Society of Intensive Care Medicine Annual Congress held October 1–5, 2011, in Berlin, Germany.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 886
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}