

Abstract
BACKGROUND: There is a growing interest in the role of comorbid anxiety in patients with COPD. Comorbid anxiety has a major impact on physical functioning, health-related quality of life, and healthcare utilization. However, the prevalence of clinical anxiety, particularly specific anxiety diagnoses, in patients with COPD remains unclear.
OBJECTIVE: We performed a systematic review of studies that report the prevalence of clinical anxiety and specific anxiety disorders in patients with COPD.
METHODS: We searched for articles in CINAHL, EMBASE, MEDLINE, and PsycINFO, from 1966 to January 31, 2012, with a focus on studies that utilized clinical interviews for a robust psychiatric diagnosis in patients with COPD.
RESULTS: Of 410 studies identified, 10 met the inclusion criteria for review. The studies had small to modest sample sizes (n = 20–204) and included mainly male COPD subjects (71% male). The prevalence of clinical anxiety ranged from 10–55% among in-patients and 13–46% among out-patients with COPD. The reported prevalence of specific anxiety disorders ranged considerably, and included generalized anxiety disorder (6–33%), panic disorder (with and without agoraphobia) (0–41%), specific phobia (10–27%), and social phobia (5–11%). Women were significantly more likely to have a clinical anxiety disorder, particularly specific phobia and panic disorder.
CONCLUSIONS: There is a high prevalence of clinical anxiety in patients with COPD. Social phobia and specific phobia appear to be particularly prevalent, yet they have received little attention within existing literature. Further research into effective management and screening for clinical anxiety disorders is warranted.
Introduction
There is a growing and justified interest in the role of comorbid psychological disease in patients with chronic illness. Until recently, there has been little focus on the role of psychiatric disorders in patients with respiratory disease, particularly COPD. However, emerging evidence suggests that the impact of comorbid anxiety and depression on patients with COPD may have a major bearing upon physical functioning, quality of life, and healthcare utilization.1–3
Comorbid anxiety and depression are more common in patients with COPD than with other chronic conditions (eg, osteoarthritis) and other respiratory diseases such as pulmonary tuberculosis (TB).4,5 This may be due to a number of factors, including more severe symptoms and restriction in daily activities, higher frequency of hospitalizations, and the progressive disabling nature of the disease. Anxiety and depression have been identified as the most common psychiatric comorbidities in those with COPD, and recent clinical guidelines both from the National Clinical Guideline Centre6 and the Global Initiative for Chronic Obstructive Lung Disease7 have highlighted the importance of the effective screening and management of both conditions. Over the last few decades, COPD research has been particularly concerned about the prevalence and impact of comorbid depression, and recent findings suggest that clinical depression is better recognized by physicians than is clinical anxiety.8,9 However, in recent years there has been a rising interest in the role of anxiety disorders and the complex interactions that exist between anxiety and respiratory symptoms, particularly those associated with panic.4
Previous reviews have explored the prevalence and management of comorbid anxiety in patients with COPD, based on clinically relevant symptoms, but these have only briefly considered the specific types of psychiatric anxiety disorders and their impact.10 Although there are a number of studies that report the prevalence of anxiety symptoms, the vast majority of these studies do not provide a clinical diagnosis. Rather, they utilize self-report measures, which give an indication of clinically relevant anxiety symptoms. Studies8,10 have utilized a variety of instruments to screen for anxiety in patients with COPD. The Hospital Anxiety Depression scale has been widely used to assess anxiety in patients with COPD.11 However, there are often inconsistencies in the cutoff scores used to determine clinically relevant anxiety symptoms.12,13 Scale items may also overlap with the somatic symptoms of COPD, potentially leading to overestimate or misdiagnosis of anxiety, which can be avoided with a robust clinical interview. Screening tools offer a measure of psychological distress rather than a specific psychiatric diagnosis.4 This is particularly important for an anxiety diagnosis, where a wide spectrum of anxiety disorders exist. We hypothesize that anxiety disorders are common in patients with COPD.
The aim of this systematic review is to synthesize the available literature in order to estimate the prevalence of clinical anxiety and specific anxiety disorders in patients with COPD.
Methods
Search Strategy
We searched the following databases AMED, CINAHL, EMBASE, MEDLINE, and PsycINFO, using the search terms: chronic obstructive pulmonary disease AND (exp anxiety OR exp anxiety disorders OR anx$.mp OR panic OR agoraphobia OR generalized anxiety disorder OR post-traumatic stress disorder OR phobia). The databases were searched from their inception, 1966, to January 31, 2012. We also reviewed the reference lists of selected studies to retrieve any articles that might have been missed. Authors of selected trials were contacted if any further information was required. The first author (TGW) conducted citation identification and study selection, and this was double checked by a second author (AMY).
Selection Criteria
Studies were included if they were prospective, had diagnosed anxiety disorders from a clinical interview using a recognized psychiatric format (eg, Diagnostic and Statistical Manual of Mental Disorders-IV [DSM-IV]14 or previous versions of DSM, or International Classification of Diseases, 10th Revision [ICD-10]15), and were published in English.
Data Collection and Appraisal
Each author independently extracted data for demographics, diagnosis methods, and prevalence rates of anxiety disorders, using a data abstraction sheet. Differences were resolved through consensus.
Results
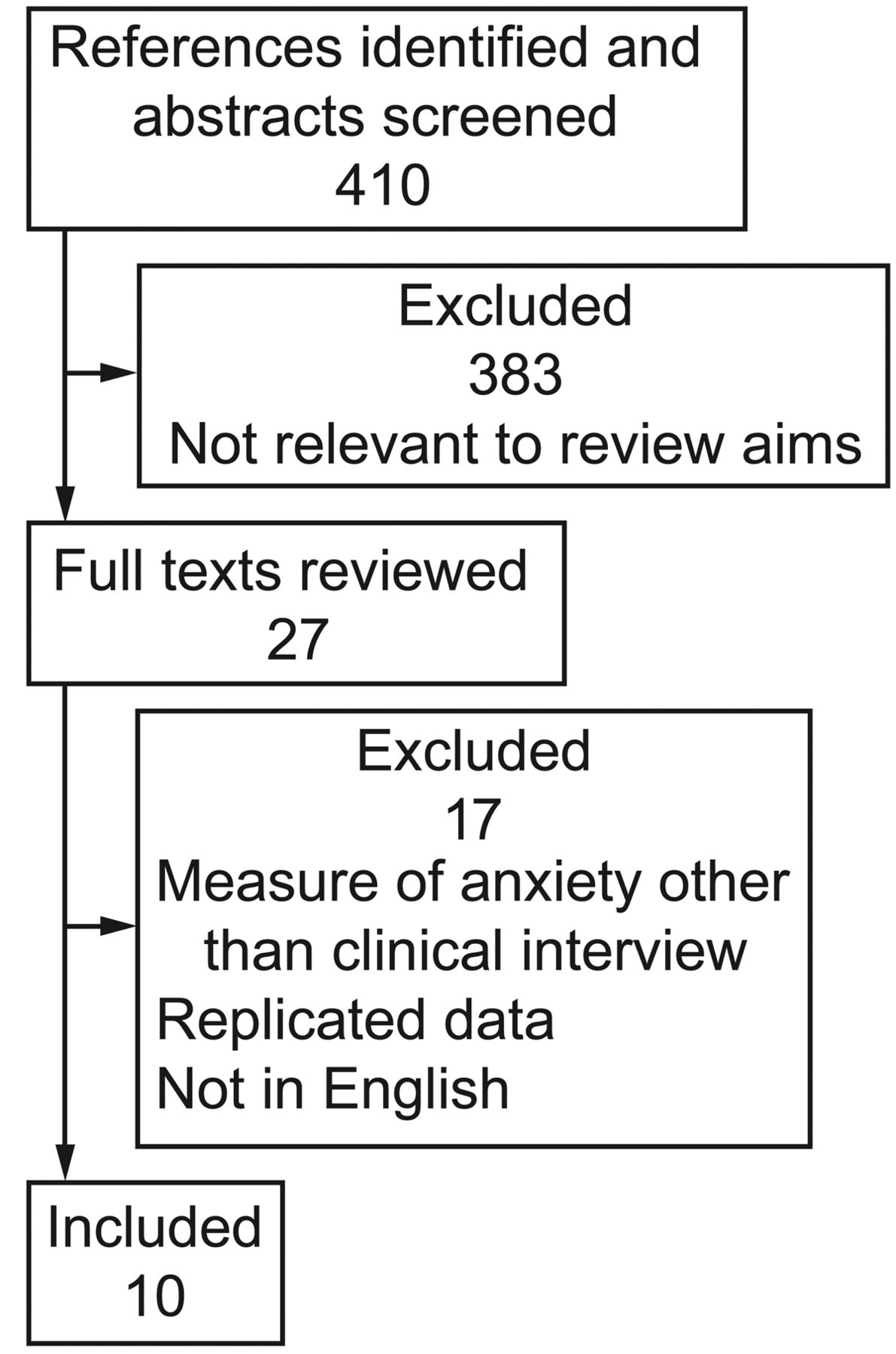
Of the 410 studies that were found and screened, 27 were identified as being potentially relevant for inclusion. Of those studies initially selected, only 10 met the inclusion criteria.3–5,8,16–21 Key information from included studies is detailed in Table 1. The main reasons for study exclusion were that studies did not use a clinical interview, replicated existing data, or were not published in English. The Figure illustrates the selection process.
Demographics and Characteristics of Included Studies

Flow chart of literature search.
Study Subjects
A total of 691 subjects were included in this review. The studies had small to modest sample sizes, which ranged from 20–204 subjects. Sample sizes in studies of out-patients were generally larger than those of in-patient populations. The sample size for in-patient studies ranged from 20–50 (mean 35) subjects, while out-patient studies ranged from 50–204 (mean 130) subjects. The reporting of COPD severity (eg, mild, moderate) was poor and inconsistent, and therefore it is difficult to assess the homogeneity of COPD patients.
The majority of subjects in the selected studies were male (71%). One study5 had an entirely male sample, and 2 other studies had a substantial proportion of male subjects that exceeded 80%.8,16 Of the 10 studies, just 2 had samples that were close to a 1:1 male-female ratio.3,20
Diagnostic Criteria for Anxiety Disorders
The majority of studies (7 of 10) used a DSM diagnosis for clinical anxiety, which varied slightly, depending on which version of the DSM criteria was available at that time. Most studies utilized a structured diagnostic clinical interview for psychiatric assessment, but the type of interview varied considerably. Four studies utilized an unstructured clinical interview.11,16,19,21
Clinical Anxiety Disorder
A total of 8 studies were found that reported the prevalence of clinical anxiety disorder (Table 2). The prevalence of clinical anxiety ranged from 10–55% (median 17%) in all subject samples. Four studies examined the prevalence of clinical anxiety in in-patients, which varied from 10–55%.4,5,16,21 There were 4 studies that reported the prevalence of clinical anxiety in out-patient samples, and prevalence ranged from 13–46%.3,18–20
Prevalence of Clinical Anxiety and Depression in Patients With COPD
Specific Anxiety Diagnoses
A total of 7 studies reported the prevalence of specific anxiety disorders, but there was inconsistency in reporting, with most studies reporting the prevalence of only selective anxiety diagnoses. In addition, one study reported the breakdown of specific anxiety disorders among a sample of out-patients who had been pre-screened for an anxiety or depressive disorder.8 As such, these findings have been presented separately (Table 3).
Prevalence of Specific Anxiety Disorders
Generalized Anxiety Disorder
Five studies were identified that reported the prevalence of generalized anxiety disorder (GAD). Prevalence ranged from 6–33% (median 16%) in all studies. Among in-patients the prevalence of GAD ranged from 10–33%, while out-patient prevalence was 6–19%. In the study that pre-screened patients for clinical anxiety and/or depression the prevalence of GAD was found to be 19%.8
Panic Disorder With and Without Agoraphobia
The prevalence of panic disorder (PD) (with and without agoraphobia) was 0–41% (median 21%) in the 7 studies that reported this specific anxiety disorder. The prevalence of PD (with and without agoraphobia) among in-patients ranged from 0–41%, while in out-patient samples the prevalence ranged from 8–21%. Among pre-screened COPD patients the prevalence was found to be 6%.8
Specific Phobia
One in-patient study4 and one out-patient study20 found the incidence of specific phobia to be 10% and 27%, respectively. In those pre-screened for anxiety or depression, specific phobia was diagnosed in 13% of COPD patients.8
Social Phobia
The prevalence of social phobia was reported in 2 studies, and was found to be 5% among in-patients and 11% among out-patient samples.4,20 Among pre-screened out-patients with COPD, the incidence of social phobia was 2%.8
Other Anxiety Disorders
There were 2 studies that reported the prevalence of other anxiety disorders, including obsessive-compulsive disorder and post-traumatic stress disorder.20,21 A single center out-patient study reported the prevalence of obsessive-compulsive disorder to be 2%.20 A similarly low incidence of post-traumatic stress disorder was reported in out-patient20 (1%) and in-patient21 (2%) samples. In contrast, post-traumatic stress disorder had a prevalence of 7% among pre-screened out-patients.8 This study also found that 12% of patients had an unspecified anxiety disorder.
Comparisons With Other Populations
In addition to reporting prevalence rates in COPD samples, 4 studies included comparison groups that comprised a mix of healthy controls and other disease groups (Table 4). One study compared subjects with COPD to 3 groups of subjects with varying types of respiratory TB, including those with recently diagnosed TB, defaulted TB, and multi-drug resistant TB.5 The prevalence of clinical anxiety was considerably lower among those subjects with recently diagnosed TB and defaulted TB, but in the multi-drug resistant TB group the prevalence was similar to those with COPD (15% vs 16%). There was no significant difference between the prevalence of anxiety in all TB groups, when compared with subjects with COPD. Another study that compared COPD subjects to hypertensive subjects and healthy controls found an identical prevalence of clinical anxiety (10%) among the 2 subject groups, but a considerably lower prevalence (3%) among a matched group without chronic disease.16 A significantly lower prevalence of anxiety disorder was found among a matched clinical control group consisting of subjects with chronic orthopedic disease when they were compared to subjects with COPD (20% vs 55%, P < .05).4 Finally, one study compared subjects with COPD to their spouses and found similar rates of anxiety disorders, including PD and GAD (13% vs 11%).19
Prevalence of Clinical Anxiety in Comparison Populations
Sex Differences
One study reported the differences in anxiety prevalence between males and females.20 Women were significantly more likely to have elevated anxiety disorder than men (56% vs 35%, P = .04). In particular, women were significantly more likely to have specific phobia (34% vs 17%, P = .04) and PD (29% vs 9%, P < .01) than their male counterparts.
Clinical Depression
Eight studies reported the prevalence of depressive disorders (see Table 2), which ranged from 0–42% (median 17%). Four studies examined the prevalence of clinical anxiety in in-patients, which varied from 0–40%.4,5,16,21 In addition, 4 studies reported the prevalence of clinical anxiety in out-patient samples and prevalence ranged from 6–42%.3,18–20
Discussion
To our knowledge, this is the first systematic review to specifically address the prevalence of clinical anxiety disorders in patients with COPD. The findings indicate the prevalence of clinical anxiety is high in both in-patient and out-patient COPD populations. This echoes findings from previous reviews that primarily focus upon data obtained from self-report screening tools.10,22 We excluded any studies reporting a non-clinical diagnosis (ie, those not utilizing a clinical interview, eg, based on DSM criteria) and found a prevalence of clinical anxiety of 10–55%, considerably higher than that found in the general population (4.1%).23 The prevalence of clinical anxiety in subjects with COPD was also significantly higher than in those with TB and chronic orthopedic diseases. Specific anxiety diagnoses, including GAD, PD (with and without agoraphobia), specific phobia, and social phobia, are relatively common and occur at a greater rate in subjects with COPD, compared with the general population.24,25
This review has several limitations. The findings from this review may be limited by the fact that studies were included only if they were published in English. In addition, there is the possibility that we may have missed studies during our literature search. However, we believe that our search strategy was robust and that we present an accurate account of the current evidence. The prevalence of clinical anxiety ranges markedly, but it is not clear exactly why this might be. There are a number of factors that may have caused such diverse reporting of anxiety prevalence.
First, it is possible that the samples varied in terms of their demographics and disease severity. Many of the included studies were not specific about the diagnostic criteria and severity of COPD among their samples, and it is therefore feasible that this review included a relatively heterogeneous sample of patients. In addition, the inconsistency in reporting means that it is difficult to pool estimates about the prevalence according to the classification of COPD severity.
Second, the sample sizes of included studies were generally small. This might be due to the difficulty in recruiting COPD patients to undergo a psychiatric interview. Furthermore, structured clinical interviews are also time consuming and can be conducted only by trained clinicians.
Third, a number of different psychiatric classification systems and interview schedules have been utilized. This might lead to inconsistency in the interpretation of symptoms and diagnosis. However, although there is an element of subjectivity of clinical experience in the diagnosis of a psychiatric disorder (as there is in any medical diagnosis), there is some evidence to suggest that trained clinicians undertaking clinical interviews, especially structured clinical interviews (eg, the Structured Clinical Interview of the DSM) demonstrate a high level of inter-rater reliability.26 Some studies failed to use a standardized structured interview, and it is therefore difficult to directly compare these results to other prevalence studies.
Finally, many of the studies included predominantly male samples. The lowest prevalence of comorbid anxiety disorders was found in studies that had predominately male samples (62–100% male in studies reporting the lowest prevalence).5,16,18,19 Women have a higher incidence of anxiety than men among the general population.27 This also appears to be true among women with COPD, who are > 1.5 times more likely to have a clinical anxiety disorder than their male counterparts.20
The heterogeneity of the studies included in this review limits the generalizability of our findings. The majority of studies did not have control groups, and therefore it is difficult to directly compare the prevalence of anxiety in subjects with COPD to healthy controls or other clinical samples. One study from Nigeria compared subjects with COPD to healthy controls and found that the prevalence of anxiety disorders was significantly greater in subjects with COPD (P < .05).16
This review found similarly high levels of anxiety in both in-patient and out-patient samples, and suggests that such a high incidence cannot be explained solely by the presence of an exacerbation-related hospitalization. Rather, anxiety in patients with COPD is most likely to be a chronic and disease-related phenomenon.4 Our findings also reveal the high prevalence of specific anxiety disorders, including PD (with and without agoraphobia) and phobic anxiety disorders. PD has been highlighted elsewhere as being particularly common in patients with COPD.4
It is not clear why there is an elevated prevalence of anxiety in patients with COPD. One theory asserts that the dyspnea-anxiety relationship may play an important role in the development of anxiety disorders such as PD. Recent brain imaging studies support the idea that there may be a shared etiology between anxiety and dyspnea. Studies indicate that the affective dimension of dyspnea (characterized by distress and unpleasantness) are processed in the same areas of the brain that process fear, anxiety, and pain.28–30 Other theories, such as Clark's cognitive model of panic,31 have focused upon psychological rather than physiological explanations. Clark's model proposes that panic and anxiety result from the catastrophic misinterpretation of certain bodily sensations such as dyspnea.32 Somatic symptoms of anxiety (ie, dyspnea) may be similar to those associated with COPD, and patients with catastrophic thoughts about such symptoms may have an elevated risk of anxiety. In addition, there is an overlap between anxiety and depressive symptoms in patients with COPD, which may increase the prevalence of patients with “anxious depression” as reported in other chronic diseases.33–35 There have been reports that patients with both anxiety and depression are more likely to exhibit far higher level of suicidal ideation and chronic depressive symptoms, compared to patients with depression or anxiety alone.33–35 Further work is needed in patients with COPD.
In contrast to PD and GAD, there has been little discussion of phobic anxiety disorders within the COPD literature. Results from this review suggest that the prevalence of social phobia in patients with COPD ranges from 5–11%. This is significantly higher than that found in the general elderly population (1–2%).22 Social phobia is characterized by inappropriate anxiety experienced in situations in which a person is observed and could be criticized.36 The relationships between social phobia and COPD have yet to be explored, but it is possible that the increased prevalence of this disorder is due to increased self-consciousness and embarrassment. A recent study exploring the experiences of COPD patients with anxiety indicates that patients may feel embarrassed by their breathlessness, and also by somatic anxiety symptoms such as excessive sweating and urinary incontinence.37 Other studies have also reported that patients with COPD may feel embarrassed in social environments, particularly if they have overt signs of their respiratory disease (eg, ambulatory oxygen).38
The prevalence of specific phobia is also high in this patient group. Laurin and co-workers reported that 27% of COPD patients had specific phobia, making it the most common anxiety disorder among their sample.20 This prevalence is significantly higher than that found in the general elderly population (3–10%).24 Vögele and von Leupoldt4 found that among the COPD patients (n = 20) they interviewed, a higher proportion were experiencing situational-type specific phobia, compared with patients (n = 20) without COPD. This anxiety disorder has close links to PD with agoraphobia, and may be due to fear of a specific situation36 (eg, being without medication or being short of breath). It is possible that the high levels of specific phobia in this population are related to the exposure and subsequent fear of unpleasant situations. This is supported by observations from a qualitative study of patients' experiences, which suggests that COPD patients frequently avoid situations such as leaving the house without medication or activities that are likely to cause breathlessness.37
There is a need for further research into the management of clinical anxiety and the management of specific anxiety disorders. There is some evidence to suggest that pulmonary rehabilitation can reduce anxiety symptoms in patients with COPD.39 The efficacy of treating COPD patients with comorbid anxiety using antidepressant drug therapy is inconclusive.40 It is also suggested that psychotherapy, including cognitive behavioral therapy, may reduce symptoms of anxiety, panic attacks, and the number of hospital admissions,41–43 but recent clinical guidelines have concluded that the evidence base is inconclusive in this area.6 Future research is needed that incorporates robust clinical diagnosis alongside self-report measures as outcome measures, so that the efficacy of interventions on specific anxiety disorders can be explored in more detail. Specifically designed pharmacologic and non-pharmacologic interventions to treat anxiety disorders are worthy of consideration. In addition, further work is needed to examine the factors that contribute to elevated levels of anxiety disorders in patients with COPD.
Conclusions
This review of gold standard studies, which diagnosed anxiety disorders from a clinical interview using a recognized psychiatric format, concludes that clinical anxiety disorders are highly prevalent in patients with COPD. Perhaps more important is the finding that specific anxiety disorders, including phobias, which have had little mention within the COPD literature, are relatively common. Therefore, clinicians should be particularly vigilant in identifying patients who might be suffering from a clinical anxiety disorder, particularly phobic disorders. Recent estimates suggest that fewer than half of patients with clinical anxiety are identified and followed-up by healthcare providers.44 In view of the findings from this review, it is important to note the ability of screening tools in detecting suspected clinical anxiety disorders. At present there are no instruments available that have been specifically designed to screen for clinical anxiety in patients with COPD. Existing instruments may be limited by their ability to recognize anxiety in populations with somatic disease. For example, commonly used screening tools, such as the Beck Anxiety Inventory and Hospital Anxiety Depression scale, contain items that load strongly onto somatic factors.45,46 Therefore, caution should be exercised in the use of screening tools for anxiety symptoms to identify potential anxiety disorders.
Footnotes
- Correspondence: Abebaw Mengistu Yohannes PhD, Research Institute for Health and Social Change, Department of Health Professions, Manchester Metropolitan University, Elizabeth Gaskell Campus, Hathersage Road, Manchester M13 0JA United Kingdom. E-mail: A.yohannes{at}mmu.ac.uk.
The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}