

Abstract
BACKGROUND: Most heat-and-moisture exchangers (HMEs) for patients with tracheostomy and spontaneously breathing are small and have suction ports that allow some expiratory gas to escape, which loses water vapor held in the expired gas. Recently, a heated-and-humidified high-flow system for spontaneously breathing patients with tracheostomy was developed. Little is known, however, about the humidifying performance of HMEs or heated-and-humidified high-flow systems for spontaneous breathing patients with a tracheostomy.
OBJECTIVE: To investigate the humidifying performance of the HMEs and heated-and-humidified high-flow systems for spontaneously breathing patients with tracheostomy.
METHODS: Adult spontaneously breathing subjects with tracheostomy and were enrolled when their respiratory parameters and SpO2 were stable. We measured absolute humidity, relative humidity, and temperature by using a capacitance-type moisture sensor at the outlet of the tracheostomy tube. Heated-and-humidified high flow was delivered via the a humidifier and tracheostomy interface, and a selected HME. The subjects received heated-and-humidified high flow, after which an HME was used for humidification before switching back to a heated-and-humidified high-flow system.
RESULTS: Ten subjects (5 men, 5 women; mean ± SD age, 72 ± 12 y) were enrolled. The admission diagnoses were neurologic (5 subjects), respiratory failure (3), and cardiac arrest (2). The APACHE (Acute Physiology and Chronic Health Evaluation) II score was 24 (interquartile range, 20–27). Tracheostomy was performed on day 7 (interquartile range, 5–11 d) after endotracheal intubation, and the duration of mechanical ventilation was 10 d (interquartile range, 6–11 d). The temperature with the HME was 29.9 ± 1.0°C and, during heated-and-humidified high-flow use was 35.3 ± 0.8°C (P < .001). With both the HME and the heated-and-humidified high-flow system, the relative humidity reached 100%; the absolute humidity with HME was 30.2 ± 1.8 mg/L, and, with the heated-and-humidified high-flow system, was 40.3 ± 1.8 mg/L (P < .001).
CONCLUSIONS: In spontaneously breathing subjects with tracheostomy, an heated-and-humidified high-flow system achieved higher absolute humidity than did an HME.
Introduction
Tracheostomy has a number of advantages, including improved patient comfort, easier oral hygiene, and earlier discontinuation from mechanical ventilation.1 Normally, inspiratory gas is heated in the pharynx and trachea: humidity in the trachea has been measured in the range of 36 to 40 mg/L, and the optimal absolute humidity below the carina is 44 mg/L (100% relative humidity at 37°C).2 Because the upper airway is bypassed in patients who have a tracheostomy, warming and humidification of inspired gases are often inadequate. To prevent destruction of airway epithelium, inadequate airway secretion, and airway obstruction, humidification is necessary.2 For mechanically ventilated patients, the American Association for Respiratory Care recommends that absolute humidity of passive humidification be >30 mg/L and the absolute humidity of active humidification be between 33 and 44 mg/L.3 The optimal humidity spontaneously breathing for patients with tracheostomy remains unclear.
Humidifying devices are used to compensate for the bypassed functions of the upper airway. Heated humidifiers and heat-and-moisture exchangers (HMEs) are commonly used for patients on mechanical ventilation. When reporting the results of a recent bench study, Chikata et al4 found that a heated-and-humidified high-flow system achieved better humidification than did an HME. Little is known, however, about performance of heated-and-humidified high-flow and HME in spontaneous breathing of patients with tracheostomy. We, therefore, carried out a crossover study to investigate the humidification performance of an HME and a heated-and-humidified high-flow system in spontaneously breathing tracheostomized subjects.
QUICK LOOK
Current knowledge
Humidification for spontaneously breathing patients with tracheostomy is often poor. Heat-and-moisture exchangers (HMEs) are small and light but do not necessarily supply sufficient water vapor, especially when used with oxygen. Recently, a heated-and-humidified high-flow system for spontaneously breathing patients with tracheostomy was developed.
What this paper contributes to our knowledge
Inspiratory gas humidity was measured with an HME and a heated-and-humidified high-flow system in spontaneously breathing subjects with a tracheostomy. The heated-and-humidified high-flow system delivered higher humidity than the HME. In the present study, both the HME and heated-and-humidified high-flow system supplied absolute humidity at least higher than the American Association for Respiratory Care recommendations.
Methods
Study Design and Settings
We conducted a crossover study at Tokushima University Hospital. This study was approved by the clinical research ethics committee (approval 2033). At enrollment, written informed consent was obtained from the subjects or their legal representative.
Study Population
Adult spontaneously breathing subjects with tracheostomy without ventilatory support were consecutively enrolled. We excluded patients with the following: age < 18 y old; copious secretions that caused expulsion difficulties; severe respiratory or hemodynamic instability; had a requirement for >1 L/min of oxygen or FIO2 > 0.25.
Study Protocol
This study was undertaken to compare the performance of an HME (Trach-Vent+, Gibeck, Sweden; in the manufacturer's specifications: absolute humidity, 27.0 mg/L; dead space, 10 mL) and a heated-and-humidified high-flow device (MR850 and Optiflow tracheostomy interface, Fisher and Paykel Healthcare, Auckland, New Zealand) in spontaneously breathing subjects with tracheostomy. The HME was used with room air only or with added low-flow oxygen (1 L/min). A heated-and-humidified high-flow system delivers 40 L/min flow at FIO2 of 0.21 or 0.25. The heated humidifier system was set to deliver gas at a water chamber temperature of 37°C and end-inspiratory circuit temperature at 40°C. To lessen the time-series bias, the protocol for each subject comprised 3 phases, each lasted 60 min, in the following order: heated-and-humidified high flow, HME, and heated-and-humidified high flow (Fig. 1).
Time course of measurements. Subjects received heated and humidified high-flow (HHHF), after which a heat-and-moisture exchanger (HME) was used for humidification before switching back to HHHF system.
After each period, we measured the temperature and relative humidity of inspired gas by using a capacitance-type moisture sensor (Moiscope, Senko Medical, Tokyo, Japan) (response time, 3 s in the range of 40–100%) that was calibrated by using a cooler-heater water source (HHC-51, Senkoika, Tokyo, Japan). One-way valves prevented mixing of inspired and expired gases (Fig. 2). All signals from the hygrometer led to an analog-digital converter and were recorded at 50 Hz/channel with data-acquisition software (Windaq, Dataq Instruments, Akron, Ohio). Before taking internal measurements, we recorded the ambient temperature and humidity readings for 20 s. Once stabilized values were obtained for each parameter, inspired gas measurements were recorded for 1 min. Absolute humidity was calculated from the corresponding temperature and relative humidity.5 At the end of each phase, we collected readings for breathing frequency, SpO2, and hemodynamics (heart rate, systolic blood pressure, and mean blood pressure), and, for 1 min, measured tidal volume (VT) and end-tidal carbon dioxide (PETCO2) by using an S/5 Aespire (Dtex-Ohmeda, Helsinki, Finland).
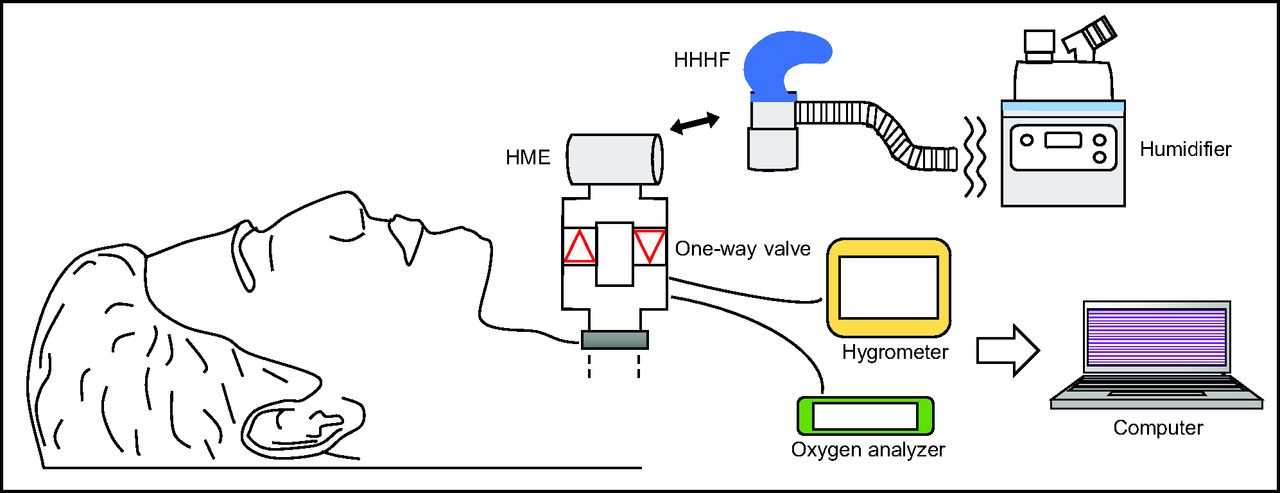
We measured the temperature and relative humidity of inspired gas by using a capacitance-type moisture sensor. One-way valves prevented mixing of inspired and expired gases. All signals from the hygrometer were sent to an analog-digital converter and recorded at 50 Hz/channel with data-acquisition software. HME = heat-and-moisture exchanger, HHHF = heated and humidified high-flow.
Statistical Analyses
Normally distributed data are shown as mean ± SD, whereas non-normally distributed data are presented as median (interquartile range [IQR]). We compared variables obtained during each study phase by using 1-way analysis of variance for repeated measures or the Friedman test. Post hoc correction for multiple comparisons was performed with the Dunnett comparison. Data analysis was conducted by using JMP statistical software version 13.1.0 (SAS Institute, Cary, North Carolina). All statistical tests were 2-tailed, and the chosen type-1 error rate was P < .05.
Results
We enrolled 10 subjects (5 men, 5 women; mean ± SD age, 72 ± 12 y). The admission diagnoses were neurologic (5 subjects), respiratory failure (3 subjects), and after cardiac arrest (2 subjects). The APACHE (Acute Physiology and Chronic Health Evaluation) II score was 24 (IQR, 20–27). All the subjects required mechanical ventilation before tracheostomy. Tracheostomy was performed at day 7 (IQR, 5–11 d) after endotracheal intubation, and the total duration of mechanical ventilation was 10 (IQR, 6–11) d. Six subjects did not require oxygen, and 4 required 1 L/min of oxygen at FIO2 of 0.25. The demographic data are presented in Table 1.
Subjects' Characteristics
No statistically significant differences were observed in ambient conditions (Table 2). Temperature with the phase 1 heated-and-humidified high flow system, phase 2 HME, and phase 3 heated-and-humidified high-flow system were 35.3 ± 0.8°C, 29.9 ± 1.0°C, and 35.5 ± 0.8°C, respectively (P < .001). Relative humidity reached 100% with both the HME and during heated-and-humidified high flow (P = .39). The mean ± SD absolute humidity with the HME was 30.2 ± 1.8 mg/L and, with heated-and-humidified high-flow, was 40.3 ± 1.8 mg/L (1st phase) and 40.6 ± 1.7 mg/L (2nd phase) (P < .001) (Fig. 3).
Effects of HME and HHHF
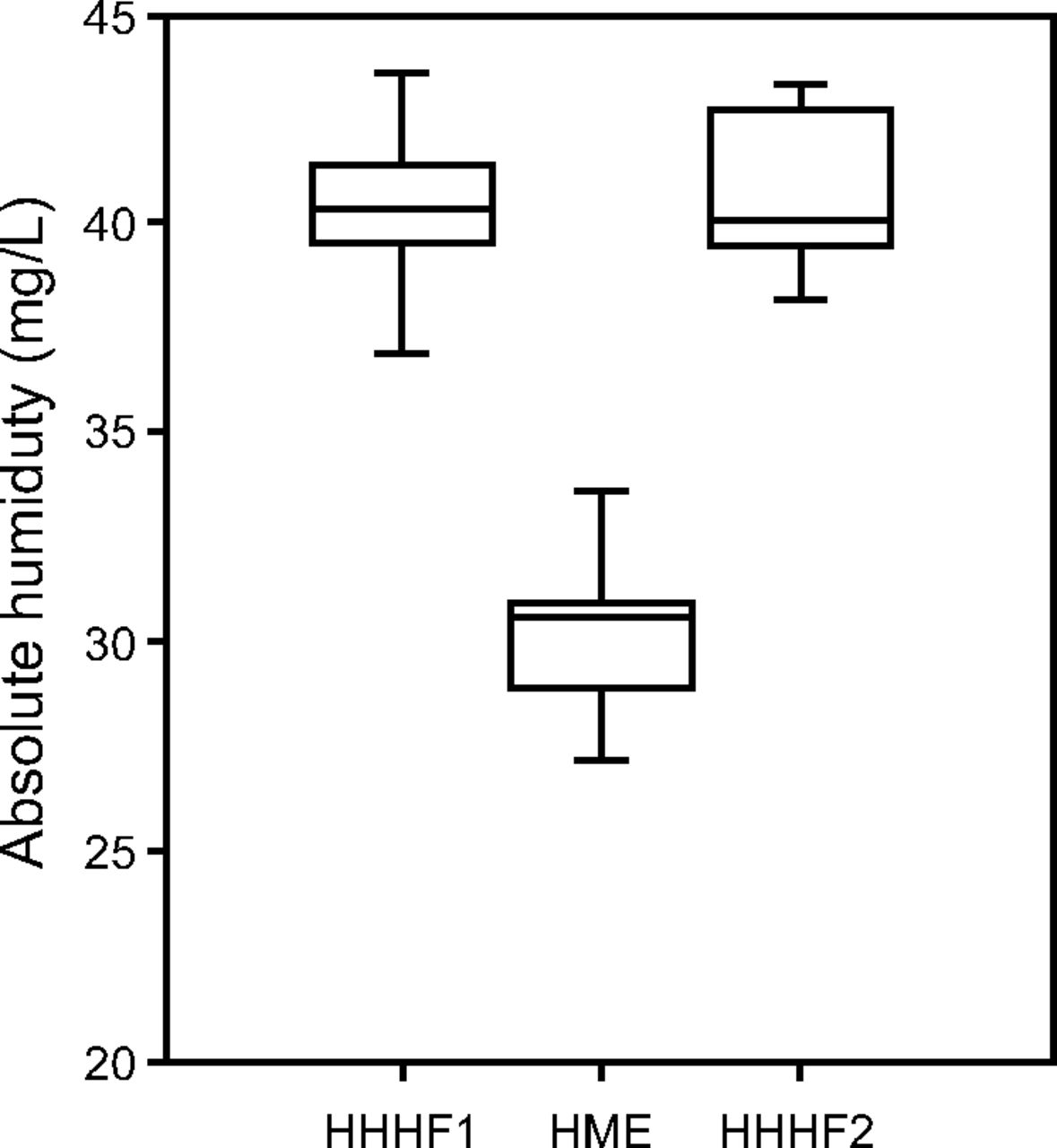
Absolute humidity during each period. Both devices supplied >30 mg/L of vapor, whereas the HHHF system supplied higher vapor. HHHF = heated and humidified high-flow, HHHF1 = HHHF (1st phase), HHHF2 = HHHF (2nd phase), HME = heat-and-moisture exchanger.
In phase 1 heated-and-humidified high flow, phase 2 HME, and phase 3 heated-and-humidified high flow, PETCO2 was 34.4 ± 3.7 mm Hg, 35.9 ± 3.9 mm Hg, and 34.2 ± 3.7 mm Hg, mean ± SD respectively (P = .01), and, for minute ventilation, was 6.2 ± 1.4 L/min, 7.3 ± 1.4 L/min, and 6.0 ± 1.2 L/min, mean ± SD respectively (P = .02). Heart rate, blood pressure, and SpO2 remained stable across the phases, and the percentage difference of VT and breathing frequency were close to 5%.
Discussion
In this study, we compared the humidification performance of an HME and a heated-and-humidified high-flow device in spontaneously breathing subjects with tracheostomy, and found that the absolute humidity was higher during heated-and-humidified high flow. Because the heated-and-humidified high flow system delivered >33 mg/L and the HME delivered >30 mg/L, both systems satisfied the American Association for Respiratory Care minimum humidification requirements for patients on mechanical ventilation.3
However, the International Organization for Standardization 81856 recommends an absolute humidity of >33 mg/L, which is also what Williams et al2 considered the minimum acceptable level of humidity for inspired gases. When comparing 11 HMEs in a bench study, Chikata et al4 found the highest absolute humidity was 30.7 mg/L with Trach-vent+. After measuring the absolute humidity of 48 HMEs used in mechanical ventilation, Lellouche et al7 reported the average absolute humidity as 27.5 ± 4.4 mg/L, and the highest as 31.9 ± 0.6 mg/L. Our current findings with the subjects with tracheostomy showed an HME that delivered comparable levels of absolute humidity as in these bench studies.4,7
In the present study, absolute humidity with the heated-and-humidified high-flow system was higher than in our previous bench study.4 Four factors may account for the discrepant results. In the bench study, the Airvo 2 delivered 37.7 mg/L of absolute humidity,4 but the absolute humidity in our subjects was 40.3 ± 1.8 mg/L, mean ± SD. This higher inspiratory absolute humidity may have resulted from the adaptability of subjects' breathing patterns. Humidification performance varies according to VT and breathing frequency. Low VT and, possibly, high breathing frequency increase absolute humidity.4 We found a lower VT (248 vs 300–500 mL) and higher breathing frequency (24 ± 6 vs 10–20 breaths/min) than in our bench study.4 The results may also differ owing to the use of 1-way valves to separate expiratory gas; however, we could not completely exclude the possibility of overestimation owing to admixture of water vapor from expired gases.
As discussed previously, it is difficult to measure humidification correctly.8 In addition, the environmental conditions differed. At <100% relative humidity, absolute humidity is dependent on inspiratory gas temperature. The Optiflow tracheostomy interface connected to the tracheostomy tube was exposed to the ambient temperature, and incoming heated air was cooled at the airway opening of the tracheal tube.9 In the study by Chikata et al,10 room temperature was lower than in the ICU (24.0°C vs 25.0°C), which possibly resulted in more heat loss. Finally, heated-and-humidified high-flow devices are different. Although the mechanisms are not disclosed, the MR850 humidifier and Airvo 2 have different temperature-control mechanisms; in practice, the Airvo 2 provides better humidification than did the MR850 humidifier.
Several mechanisms may account for the beneficial effects of heated-and-humidified high-flow therapy, such as lower PETCO2 and minute ventilation, reductions that might result from decreased lung dead space and better CO2 washout. Breathing frequency and VT slightly decreased without statistical significance (P = .06 and .08, respectively), which possibly indicated a little less work of breathing. There also are anatomic differences in the way the gas is delivered by the heated-and-humidified high-flow system and high-flow nasal cannula, which encroach on nasopharyngeal dead space. Heated-and-humidified high-flow system supports ventilation directly at the tracheal airway opening, and such proximity to the lung may enable more-effective lung inflation and escape of gas. However, the current investigation was not designed to investigate these effects, and the mechanisms have yet to be resolved.
The cost of the heated-and-humidified high-flow system and the HME should be taken into account. The cost of HMEs is approximately $2, and it needs to be changed every 48 h.11 However, the cost of a heated-and-humidified high-flow system is higher than an HME because high-flow systems need a tracheostomy interface, heated wire circuit, distilled water, and high-flow oxygen.11 However, for patients who are critically ill, the heated-and-humidified high-flow system is justified because it reduces complications related to inadequate humidity and the risk of re-intubation.12
In spontaneously breathing subjects with tracheostomy the absolute humidity was higher during heated-and-humidified high flow than with the HME. Humidification is needed in all patients who are critically ill and receiving ventilator support. Even so, the clinical benefits of different methods are still far from being demonstrated and remain to be elucidated. To avoid serious complications related to breathing dry gases, humidifiers should be chosen to provide adequate performance according to clinical conditions.
Limitations
Our study had several limitations. First of all, the sample size was small. Moreover, all the subjects had a stable respiratory status, and 4 of 10 subjects needed only low-flow oxygen. The absolute humidity would be lower in patients with high VT and high inspiratory flow. Our test protocols were also brief. When evaluating the humidifying performance of an HME and a heated-and-humidified high-flow system for spontaneously breathing subjects with tracheostomy, we found higher absolute humidity during heated-and-humidified high flow.
Footnotes
- Correspondence: Masaji Nishimura, Critical Care and Emergency Medicine, Tokushima University Graduate School, 3-18-15 Kuramoto, Tokushima, Japan 770-8503. E-mail: nmasaji{at}tokushima-u.ac.jp.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 233
- Copyright © 2019 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}