

Abstract
BACKGROUND: Muscle atrophy and deconditioning are common complications in patients on prolonged mechanical ventilation (PMV). There are few studies that reviewed the effects of electrical muscle stimulation in this population. The purpose of this study was to examine the effects of electrical muscle stimulation on muscle function and hospitalization outcomes in subjects with PMV.
METHODS: Subjects on mechanical ventilation for ≥21 d were randomly assigned to the electrical muscle stimulation group (n = 16) or the control group (n = 17). The electrical muscle stimulation group received daily muscle electrical stimulation for 30 min/session for 10 d. The measurement of muscle strength (by medical research council [MRC] scale), leg circumference, and physical functional status (by Functional Independence Measure [FIM] scores) were performed before and after completion of the study. The length of stay in respiratory care center of subjects were recorded.
RESULTS: After electrical muscle stimulation, there was no difference in pulmonary function between the electrical muscle stimulation and control groups. Significantly increased in MRC points was found in the electrical muscle stimulation group after intervention (2 [1-7] points vs 2 [1-3.5] points, respectively, P = .034). No difference in MRC points was found between baseline and post-measurement in the control group (1[1-2] points vs 1[1-2.5] points, respectively, P > .99). At the end of the study, leg circumference in control group significantly decreased when compared with baseline (47.5 ± 8.3 cm vs 44.6 ± 5.7 cm, respectively, P = .004) and remained unchanged in the EMS group. However, no significant differences were found between the electrical muscle stimulation and control groups. There was no difference in physical functional status and hospital stay between the electrical muscle stimulation and control groups.
CONCLUSIONS: Electrical muscle stimulation enhanced muscle strength in subjects who received PMV. Electrical muscle stimulation can be considered a preventive strategy for muscle weakness in patients who receive PMV. (ClinicalTrials.gov registration NCT02227810.)
- electrical stimulation
- muscle weakness
- critical illness
- hospitalization outcomes
- mechanical ventilation
- physical function
Introduction
Invasive ventilation is a necessary treatment for patients with respiratory failure in ICUs. As patients recover from acute illness, some may experience weaning difficulties and require prolonged mechanical ventilation (PMV). Patients who require PMV are often transferred to subacute care units, such as respiratory care centers, for continued care and further weaning. According to the National Association for Medical Direction of Respiratory Care in the United States, it is estimated that, by 2020, there will be 600,000 cases per year of PMV in the United States, defined as at least 6 h of mechanical ventilation per day for >21 consecutive days,1 at a cost of approximately $50 billion.2 Improving the weaning rate and hospitalization outcomes for patients who receive PMV has become increasingly important.3
Various complications can occur during PMV and affect patient outcomes. Scheinhorn et al4 reported that 98.7% of subjects were bedridden on admission to weaning centers and that 69% of subjects were still bedridden on discharge. Even 12 months after discharge, only 19% of subjects who received PMV were fully active during daily life.4 Prolonged bed rest can reduce knee extensor strength by approximately 0.6% per day and muscle mass by 0.4% per day.5 Individuals who receive PMV are commonly immobilized and experience complications, including muscle wasting, pneumonia, atelectasis, and deconditioning. Muscle weakness and general deconditioning were reported to be associated with poor hospitalization outcomes, such as increased service use, longer hospital length of stay, and higher mortality rates.6 Moreover, skeletal muscle dysfunction is a major source of exercise intolerance and impaired capability to perform activities of daily living. Muscle-strengthening interventions can break this negative cycle and improve patients' prognosis.
There is compelling evidence that pulmonary rehabilitation can improve functional capacity and daily independence in patients with chronic pulmonary dysfunction.7 Muscle-strengthening exercises, a component of pulmonary rehabilitation programs, can help patients translate gains in muscle strength into physical capacity. The enhancement in muscle strength was associated with improvement of hospitalization outcomes by shortening the number of days from bed to chair and by reducing the risks of complications that arise from long-term confinement to the bed.8 However, patients who receive PMV may be too fragile to initiate exercise, given their severely impaired cardiopulmonary function and muscle weakness. Consequently, there is growing interest in the use of nonvolitional assistive technologies that facilitate early exercise, for example, electrical muscle stimulation.
Electrical muscle stimulation involves applying a series of stimuli to skeletal muscle, primarily to trigger muscle contraction,9 and it can be used for the recovery of muscle mass and muscle strength after prolonged immobilization.10 Electrical muscle stimulation may also improve circulation and exercise capacity in both chronic heart failure and COPD populations.11 Electrical muscle stimulation is reported to enhance growth factors of localized muscle, and this may also act as an anabolic stimulus to the respiratory muscle through the circulation system.12 However, the effects of electrical muscle stimulation on the PMV population remain unclear. Our primary aim was to evaluate the potential effects of electrical muscle stimulation on muscle function and physical function in subjects with PMV. We also evaluated the effects of electrical muscle stimulation on secondary measures of hospitalization outcomes.
QUICK LOOK
Current knowledge
As the population of prolonged mechanical ventilation (PMV) increases with decreased ICU mortality, there will be a growing number of survivors at risk of deconditioning and muscle wasting. Comprehensive pulmonary rehabilitation plays an important role in improving patients' muscle strength and functional independence. However, patients with PMV are often too fragile to collaborate in active exercise or muscle training.
What this paper contributes to our knowledge
This study showed that the subjects who received PMV had significant reductions in leg circumference after 2 weeks of hospitalization. A 2-week daily electrical muscle stimulation program resulted in the prevention of muscle atrophy and an increase of muscle strength in the subjects with PMV. The results were comparable with those of subjects in the ICU.
Methods
This prospective study was performed in a 24-bed respiratory care center at Chang Gung Memorial Hospital, Taiwan. Patients in the respiratory care center receive medical care related to treatment of their primary disease, underlying causes of respiratory failure, ventilator support, ventilator weaning, and pulmonary rehabilitation. Inclusion criteria for this study were as follows: (1) age ≧ 20 y; (2) mechanical ventilation for > 6 h/d for > 21 d; (3) failure to be weaned in the ICU; and (4) medical stability (arterial blood gas pH = 7.35–7.45, PaO2 ≧ 60 mm Hg at 40% FIO2, absence of signs and symptoms of infection, and hemodynamic stability). Exclusion criteria were cancer, acute lung or systemic infection, hemodynamic instability, previous or ongoing neuromuscular disease (eg, myasthenia gravis, Guillain–Barré disease), or conditions that could interfere with evaluation of strength, skin lesions, or obesity (body mass index of >35 kg/m2). The study was approved by the hospital's institutional review board and registered with clinicaltrials.gov (NCT02227810). The study was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from the subjects or their relatives before inclusion.
Electrical Muscle Stimulation Intervention
The electrical muscle stimulation intervention involved two 30-min electrical muscle stimulation sessions per day, 5 d/wk for 2 wk. During each session, rectangular electrodes were placed on motor points of the vastus lateralis and rectus femoris of both legs. Electrical muscle stimulation was performed by using a commercial stimulator (Omnistm 500, ZMI, Taipei, Taiwan) with biphasic waves at a simulation frequency of 50 Hz and pulse width of 400 μs, cycling 2 s on and 4 s off. Electrical muscle stimulation intensity was gradually increased until a visible muscle contraction was observed. The subjects in the control group received similar electrode placement and intervention duration, except that the stimulator power was off.
Study Procedure
This study followed a prospective and randomized design. Before subject recruitment, sequential sealed envelopes were prepared by an independent investigator (CYH), with one chosen randomly by another investigator for each subject. The subjects were then assigned to an electrical muscle stimulation group or a control group according to the label in the envelope. Age, sex, body weight, height, and diagnosis at respiratory care center admission were recorded for each subject. Disease severity was assessed within 24 h of respiratory care center admission by using the APACHE (Acute Physiology and Chronic Health Evaluation) II score. The subjects assigned to the electrical muscle stimulation group received daily electrical muscle stimulation starting from the day after completion of baseline data collection. The subjects in the control group received similar medical treatment except for the electrical muscle stimulation therapy.
Primary and Secondary Outcomes
Primary outcomes, which included pulmonary function, muscle function, and physical function, were measured on the day before the intervention (day 0) and the day after completion of the intervention (day 11). After completing the intervention program, the subjects were followed up until they were discharged from the respiratory care center. Secondary outcomes were defined as the subject's hospitalization outcomes, which included survival status, weaning outcomes, duration of ventilation in the respiratory care center, and respiratory care center length of stay.
Primary Outcomes Measurement
Pulmonary Function Measurement.
The subjects were required to maintain the semi-Fowler position during measurement of weaning profiles. During measurement, subjects' endotracheal or tracheostomy tubes were temporarily disconnected from the ventilator and connected to a spirometer (Respiradyne II, Sherwood, St. Louis, Missouri). Once the subjects were stable, the investigator (HSF) activated the spirometer and measured minute volume and breathing frequency. To measure the mouth's maximum inspiratory pressure, the investigator connected the endotracheal or tracheostomy tube with a T tube and placed a manometer (Boehringer Ingelheim, Norristown, Pennsylvania) to one end of the T tube by using a nipple adapter and a 1-way valve. After the inspiratory port was manually occluded, the investigator coached the subject to inhale actively against the occluded airway during breathing cycles for 20 to 25 s; the most negative value was recorded as the maximum inspiratory pressure.
Muscle Function Measurement.
Muscle function was assessed by skin-fold thickness, leg circumference, and quadriceps muscle strength. To measure skin-fold thickness, the investigator pinched the skin at the middle of the bilateral thigh and pulled the skin fold away from the underlying muscle; therefore, only skin and fat tissue were held. Lange calipers (Cambridge Scientific Industries, Cambridge, Maryland) were used to measure the skin-fold thickness (in mm). Two measurements were recorded and averaged. Leg circumference was measured at the level of the middle thigh. Quadriceps muscle strength, an indicator of knee extension, was assessed according to modified procedures of manual muscle testing. In brief, the subjects maintained a semi-Fowler position with the knee bent and were asked to perform a knee extension. The strength was scored according to the Medical Research Council (MRC) scoring system (Table 1).12 These scores are widely used to evaluate ICU-acquired paresis.13,14
Medical Research Council Scale Score
Physical Functional Status Measurement.
Physical functional status was assessed before and after the study period by using the Functional Independence Measure. The subjects were scored from totally dependent to completely independent, with lower scores representing greater disability. The reliability and validity of these questionnaires have been demonstrated.13
Secondary Outcomes Measurement
Respiratory Care Center (RCC) Hospitalization Outcomes.
RCC hospitalization outcomes were followed up until the subjects were discharged from the respiratory care center to ward or home. Survival status, weaning outcomes, duration of ventilation in the respiratory care center, and respiratory care center stay were recorded from the subjects' medical records. Weaning off the mechanical ventilator was considered successful if the subject was continuously free of the mechanical ventilator for >5 consecutive days.
Statistical Analysis
The main outcome was taken as quadriceps muscle power measured in the subjects on the day after completion of electrical muscle stimulation. The sample size was calculated according to a previous study,12 with assuming an SD of ±1 and an α error of .05, a sample size of 11 subjects would have 90% power to detect an increase of 1 MRC scale point on one of the stimulated muscles compared with baseline. When allowing for 10–20% in-hospital mortality and 30–40% dropouts, the sample size was increased to 19 subjects. Analysis was conducted by using SPSS v.17 (SPSS, Chicago, Illinois). The normality of distribution was examined by using the Shapiro-Wilk test.
The results were expressed as the mean ± SD for nominal distributions, and as median and interquartile range (25th-75th percentiles) for nonparametric distributions. Baseline characteristics, pre-intervention and post-intervention measurements, and continuous-variable hospitalization outcomes of the electrical muscle stimulation group and the control group were compared by using an unpaired Student t test or Mann–Whitney U test in case of nonparametric distribution. A paired t test or Wilcoxon signed-rank test was used to examine intervention effects on pulmonary function and muscle function within groups. Pearson and Spearman correlation coefficients were used to examine the relationship between baseline variables and parametric or nonparametric distributions, respectively. A chi-square test was used to analyze differences in the frequency distributions of mechanical ventilator weaning and survival rates between the groups. P < .05 indicated statistical significance.
Results
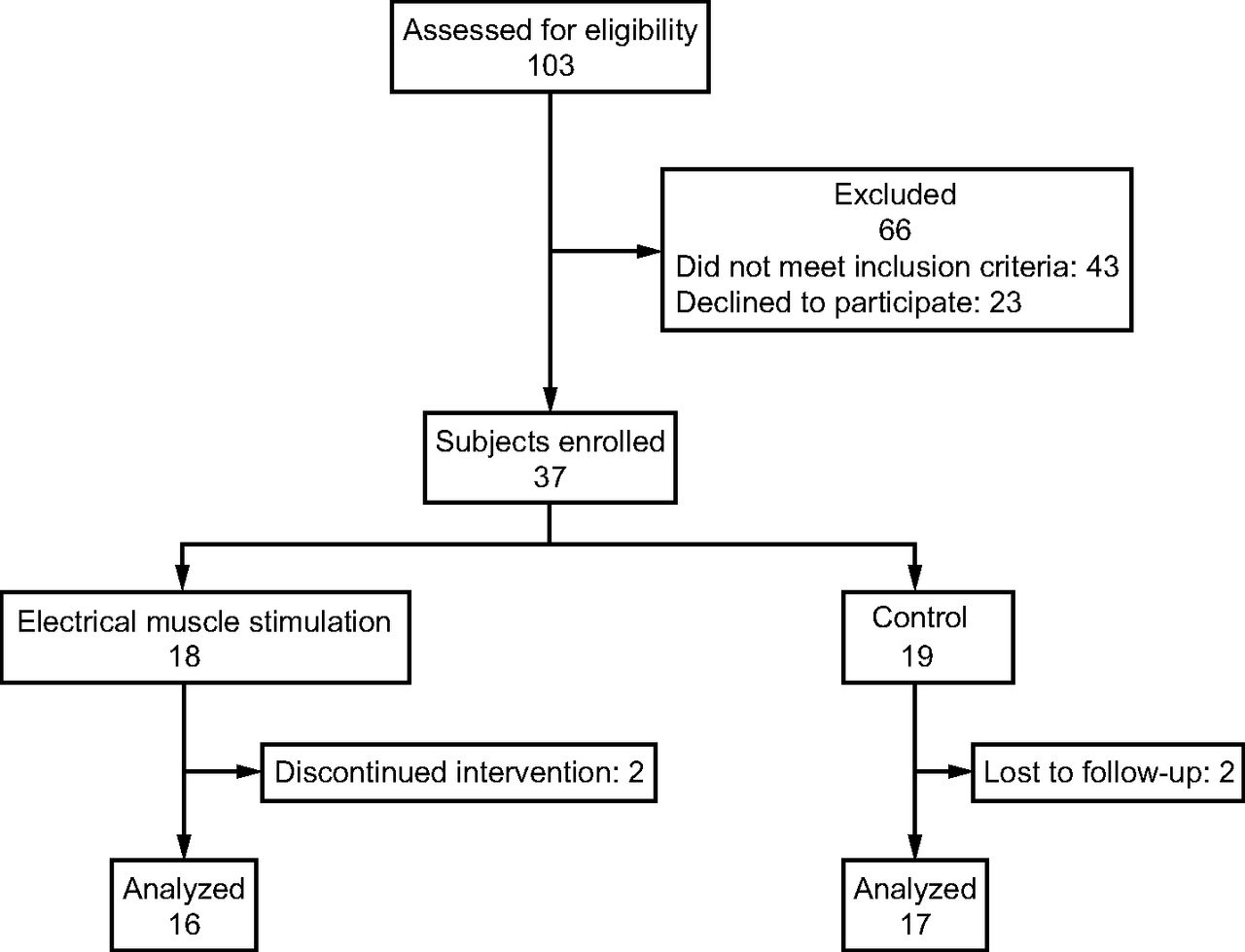
From August 2012 to July 2013, a total of 103 consecutive eligible patients were screened (Fig. 1). Sixty-six patients were excluded because they did not meet inclusion criteria (n = 43) or declined to participate (n = 23). Thus, 37 subjects were randomized into the electrical muscle stimulation group (n = 18) and the control group (n = 19). During the study period, 2 subjects in each group had acute pulmonary infection and dropped out of the study, which left 16 (electrical muscle stimulation group) and 17 (control group) for analysis.
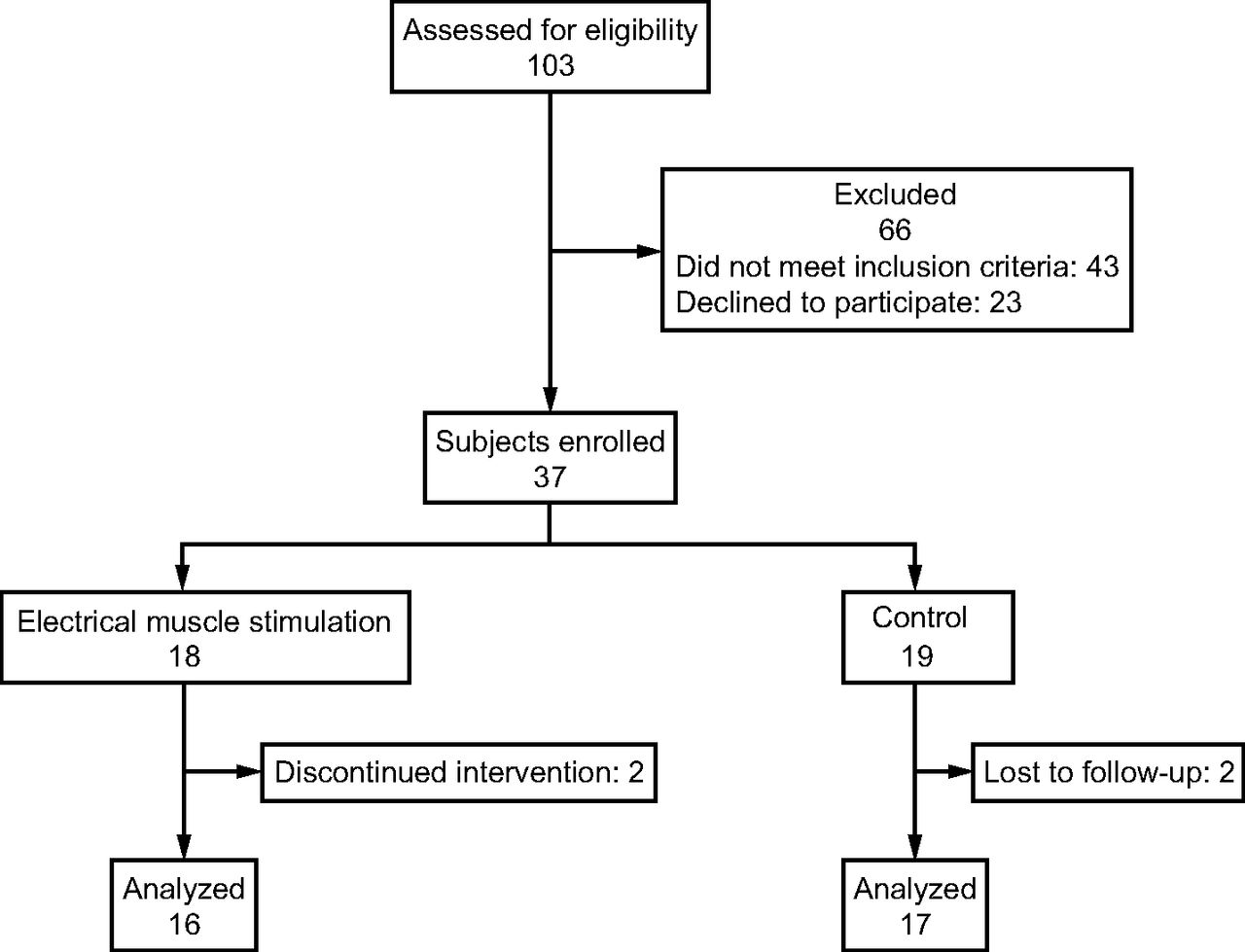
Flow chart.
Demographic Characteristics
A summary of the demographic and clinical characteristics of the subjects is presented in Table 2. Problems at admission to the respiratory care center were mostly diseases that involved the respiratory system. No significant differences existed between the electrical muscle stimulation and control groups in terms of age (mean ± SD, 77.7 ± 14.3 vs 73.8 ± 17.8 years, respectively, P = .49), BMI (mean ± SD, 22.9 ± 5.6 vs 23.1 ± 3.9 kg/m2, respectively, P = .71), severity (APACHE II score mean ± SD, 20.8 ± 7.4 vs 20.3 ± 6.3, respectively, P = .82), or diagnosis. In baseline measurements, muscle strength was significantly associated with Functional Independence Measure scores (r = 0.79, P = .001). The subjects who had higher muscle strength were associated with higher independence in daily activities. A significant inverse relationship also existed between muscle strength and APACHE scores (r = −0.41, P = .031) at baseline.
Baseline Characteristics of Study Participants
Comparisons of Primary Outcomes Between the Electrical Muscle Stimulation and Control Groups
In the measurements of pulmonary function, no significant difference existed in both pre-intervention and post-intervention measurements between the electrical muscle stimulation and control groups (Table 3). In the measurements of muscle function, no significant differences in skin-fold thickness or leg circumference were revealed between the groups in pre-intervention and post-intervention measurements. The muscle strength was assessed by MRC scale. Subjects were scored from “0 point - no muscular contraction”, “1 point -Barely detectable trace of contraction”, “2 points -active movement with elimination of gravity”, “3 points -active movement against gravity”, “4 points - active movement against gravity and some resistance”, “5 points -active movement against gravity and full resistance”.12 The MRC points of right quadriceps muscle in the electrical stimulation muscle group were significantly higher than those in the control group after the intervention (median [IQR], 2[1-4] points vs 1[1-2] points, respectively, P = .024). The MRC points of left quadriceps muscle in the electrical muscle stimulation group increased by a median of 0.5 points (IQR, 0–1 points) from the enrollment to the end of the program, which were significantly higher than those in the control group (median [IQR], 0 [0-0] points) (P = .046) (Table 5). Physical functional status was assessed by using Functional Independence Measure scores. No significant differences were found in pre- or post-measurements of Functional Independence Measure scores between the electrical muscle stimulation and control groups.
Comparisons of Pulmonary Function in Electrical Muscle Stimulation and Control Groups
Comparisons of Quadriceps Skin-Fold Thickness, Leg Circumference, and Quadriceps Muscle Power in the Electrical Muscle Stimulation and Control Groups
Comparison of Changes of Muscle Function Between the Groups
Comparisons of Primary Outcomes Between Pre-intervention and Post-intervention Measurements in Electrical Muscle Stimulation and Control groups
After electrical muscle stimulation, the subjects demonstrated an increase in tidal volume (from 190 [170-220] mL to 210 [170-245] mL; P = .07) and maximum inspiratory pressure (from 35.0 ± 9.6 cm H2O to 38.3 ± 15.1 cm H2O; P = .33). However, the difference did not reach statistic significantly (P > .05). In the control group, tidal volume decreased, from 205 (150-250) mL to 180 (170-215) mL (P = .69), and maximum inspiratory pressure decreased from 36.0 ± 14.9 cm H2O to 35.0 ± 17.7 cm H2O (P = .35).
The results regarding muscle function at the pre- and post-measurements in the 2 groups are listed in Table 4. The subjects in the electrical muscle stimulation group demonstrated a higher left quadriceps MRC points after the intervention when compared with those in their pre-intervention measurements (median [IQR], 2 [1-4] points) vs 2 [1-3.5] points, respectively, P = .034 (Table 4). No significant difference in muscle strength between pre-intervention and post-intervention measurements was found in the control group. In the electrical muscle stimulation group, the left-side leg circumference remained similar, from 39.7 ± 5.6 cm to 38.8 ± 5.1 cm (P = .38). The electrical muscle stimulation group also had a significantly lower skinfold thickness of left quadriceps muscle after completion the program (median [IQR],10.5 [6.8–15.8] mm vs 10.0 [5.8–14] mm; P = .034). In the control group, the left leg circumference decreased, from 47.5 ± 8.3 cm to 44.6 ± 5.7 cm (P = .004). No change was found in skin-fold thickness in the subjects in the control group (from 13.0 [6-19] to 14.5 [8.5-19.3] cm; P = .92). In the measurement of physical function, the Functional Independence Measure scores increased, from 29.0 ± 14.5 to 32.0 ± 18.6 (P = .12) in the electrical muscle stimulation group. In the control group, the Functional Independence Measure scores decreased, from 25.6 ± 7.9 to 25.2 ± 14.5 (P = .65).
Comparisons of Secondary Outcomes Between the Groups
For weaning outcomes, neither the weaning rate (56.3% vs 47.0%, P = .72) nor the mortality rate (18.8% vs 11.8%, P = .67) was significantly different between the electrical muscle stimulation and control groups. There was no difference in respiratory care center length of stay (median [IQR], 25 [18-49] d vs 24 [18-47] d; P = .74) and the duration of ventilation in the respiratory care center (median [IQR], 21.5[11-42.8] d vs 20 [12.5-43] d; P = .89) between the electrical muscle stimulation and control groups (Table 6).
Comparison of Hospitalization Outcomes Between the Groups
Discussion
This study examined the effects of electrical stimulation on the muscle function and hospitalization outcomes in the subjects who received PMV. We discovered that the electrical muscle stimulation program improved muscle function in the subjects who received PMV by increasing muscle strength, but no significant improvement was revealed in pulmonary function or hospitalization outcomes. The subjects in the control group had significant reductions in leg circumference (from 47.5 cm to 44.6 cm, P = .004). This indicated that the subjects who received PMV were at risk of muscle atrophy. Prolonged bed rest leads to decreased muscle protein synthesis, increased muscle catabolism, and decreased muscle mass, particularly in the lower extremities,15,16 and interactions among critical illness, invasive ventilation, and immobility may lead to further muscle function impairment.
The majority of the subjects in the present study were diagnosed with pneumonia, often associated with elevated inflammatory mediators, cytokines, an abnormal metabolic state, and increased oxidative stress. These factors induce changes in microvascular permeability, and increased glucose uptake and subsequent reactive oxygen species generation may result in decreased oxygen and nutrient delivery to muscles, protein catabolism upregulation, and muscle-fiber structure alteration.17,18 In our study, the subjects in the electrical muscle stimulation group demonstrated a significant increase in muscle strength, whereas no change was found in the control group. In addition, the subjects had a reduction in skin-fold thickness without changes in leg circumference after receiving electrical muscle stimulation.
Electrical muscle stimulation creates passive (nonvolitional) contraction of skeletal muscles through the use of low-voltage electrical impulses delivered by using surface electrodes through the skin to the underlying muscles,19 which may enhance muscle-fiber recruitment and reduce atrophy due to immobility or critical illness.20 Previous studies reported that the application of high-frequency neuromuscular electrical stimulation caused muscle contraction and resulted in an increase in the size and cross-sectional area of muscle fibers in healthy individuals21 and subjects in the ICU.22 Vieira et al23 also reported an increase in fat-free mass in subjects with COPD. Our study findings were consistent with previous findings,20–22 which indicated the potential role of electrical muscle stimulation in improving muscle function in PMV populations.
Studies reported that exercise training can increase peripheral muscle function and exercise tolerance, thereby improving physical function.7,8,24 electrical muscle stimulation can, not only improve muscle function, but also provide systemic effects that are similar to exercise. Gerovasili et al25 reported that electrical muscle stimulation in subjects who are critically ill induced an acute systemic effect on microcirculation, and Perez et al26 demonstrated that electrical muscle stimulation in healthy individuals improved oxygen-uptake kinetics and work efficiency. Central command and activation of the metaboreflex during electrical muscle stimulation may even increase sympathetic discharge and contribute to changes in heart rate, systolic blood pressure, blood volume, and cardiac output, which thereby affect skeletal muscle metabolism in a systemic manner that may include respiratory muscles. However, in the present study, no significant differences in physical function were found between the groups. The primary reason for this discrepancy may relate to differences in subject characteristics and electrical muscle stimulation protocol. In a previous study, subjects with moderate-to-severe COPD but capable of ambulation demonstrated significant improvements in muscle strength and 6-min walking test distance after a 6-wk home-based electrical muscle stimulation program.27 In this study, the subjects who received PMV who had been bedridden for >21 d demonstrated more-severe impairment in pulmonary muscle function than subjects in previous studies. Electrical muscle stimulation duration, which was shorter in our study than reported elsewhere, may also have a role in determining its effects. Our 2-wk electrical muscle stimulation session may have been too short to induce sufficient muscle strength to achieve significant improvement in physical function. In a study that involved subjects with COPD who were bedridden and received mechanical ventilation, 4 wk of electrical muscle stimulation resulted in an increase in muscle strength and the capability to transfer from bed to chair.28 Whether a longer duration would produce greater improvement in physical function requires further study.
Muscle strength and muscle mass have been reported to be negatively correlated with the stay in the hospital.29–31 The greater the muscle strength that patients regain during their hospitalization, the shorter the days they stay in the hospital.29–31 In our study, we also found that the subjects who had greater muscle strength were associated with greater independence in daily activities. The increase in MRC scale has been reported to be associated with changes of mortality rate.32 For each 1 unit increase in muscle strength, there was a 5% relative decrease in the odds of mortality.32 In our study, electrical muscle stimulation induced more improvement in the MRC scale score than that found in the control group. In addition, leg circumference was significantly decreased in the control group, whereas no changes in leg circumference were found in the electrical muscle stimulation group. The above-mentioned data indicated that the application of electrical muscle stimulation prevents the progression of muscle dysfunction in patients with PMV. However, no significant difference was found in hospitalization outcomes.
This study had several limitations. First, because muscle strength was the primary outcome in this study, the sample size was calculated based on detecting a difference in the MRC scale score. However, this sample size may have been insufficient to reveal a between-group difference in other outcomes, for example, hospitalization. In addition, we did observe a slight but significant reduction in the limb circumference of the control group, which may indicate that subjects with PMV had a high risk of muscle atrophy. Future studies with larger sample sizes are required to confirm this finding and the effects of electrical stimulation on hospitalization outcomes. Second, the timing and total duration of our study may have been confounding factors that attenuated the results. In a previous study of subjects in the ICU, electrical muscle stimulation sessions were initiated early (on the second day of admission) to prevent possible complications associated with being bedridden and were continued until the subjects were discharged from the ICU.23
However, to ensure subject safety in our study and electrical muscle stimulation session consistency, we began electrical muscle stimulation when the subjects were hemodynamically stable, and it was performed for only 10 d. The delay may have predisposed the subjects to a higher risk of deconditioning and muscle wasting; therefore, they may have required longer interventions to produce significant improvement. Also, we did not include any mechanistic evaluation of the effects of electrical muscle stimulation, electrophysiologic measures of muscle function, or histologic muscle evaluations, which might have produced more objective results.33 Although it has been widely used for evaluating muscle strength, the MRC scale remains a subjective measure and has been questioned for its interobserver variability. However, in our study, muscle strength was assessed by a single-blinded observer, and potential interobserver variability was reduced by performing muscle strength comparisons among subjects. Nevertheless, from a clinical perspective, the MRC scale is a convenient and useful measure in an respiratory care center setting.
To the best of our knowledge, this was the first study that examined the effects of electrical muscle stimulation on subjects who received PMV. Electrical muscle stimulation is a simple, noninvasive method of muscle strengthening that is well tolerated, without adverse effects, as previously described. It produces effects similar to exercise and does not require cooperation from patients. Electrical muscle stimulation could be easily implemented in patients who receive PMV without major interference to the routine care in respiratory care centers and with no apparent increase to staff work load. Because a previous study observed slight skin injury in some subjects,34 electrical muscle stimulation should be performed with care by trained personnel.
The strength of our study was that all the subjects received the same number of electrical muscle stimulation sessions before primary outcome measurements; thus, interference due to different electrical muscle stimulation sessions could be ruled out. In other studies, subjects received electrical muscle stimulation sessions until discharge from the clinical setting; consequently, electrical muscle stimulation duration and time to primary outcome varied among subjects and may have affected the objectiveness of outcome comparisons.27,30 We further ensured objectiveness by using a control group and concealed treatment allocation, and we blinded the caregivers.
Conclusions
In this randomized trial with a blinded outcome assessment, electrical muscle stimulation increased muscle strength in the subjects who received PMV, but it was ineffective in improving physical function and hospitalization outcomes. Because our trial involved only 2 weeks of electrical muscle stimulation sessions, the beneficial effects may have been underestimated. electrical muscle stimulation was well tolerated and seemed to be promising as a preventive strategy for muscle weakness in subjects receiving PMV. Future interventional studies should be conducted to examine whether earlier or longer duration electrical muscle stimulation provides more favorable outcomes.
Footnotes
- Correspondence: Chung-Chi Huang MD, Department of Respiratory Care, College of Medicine, Chang Gung University, 259 Wen-Hwa 1st Rd, Gweishan, Taoyuan City, Taiwan 33302. E-mail: cch4848{at}adm.cgmh.org.tw.
This study was supported by Chang Gung Memorial Hospital (CMRPD1C0331).
The authors have disclosed no conflicts of interest.
- Copyright © 2019 by Daedalus Enterprises





{kind=link}