

Abstract
BACKGROUND: Endotracheal intubation is a common procedure performed by respiratory therapists (RTs). The purpose of this study was to describe current RT intubation practices in North Carolina through the use of a survey instrument.
METHODS: A survey was developed by the authors using REDCap. The survey was sent via email to all licensed RTs in North Carolina. Information collected included respondent demographics, intubation practices (including training and skill maintenance), and attitudes about RT intubation practices.
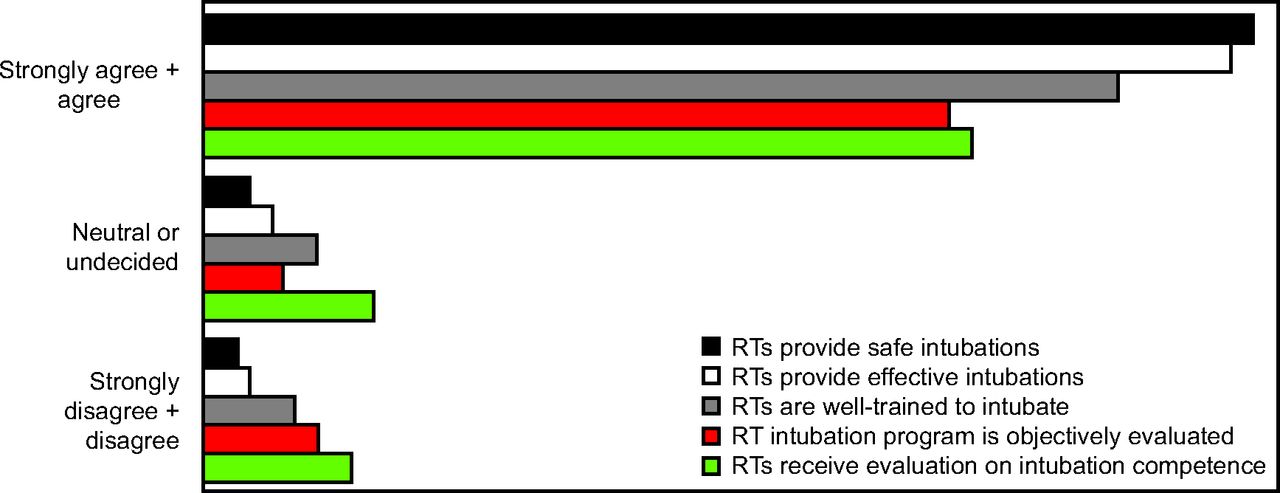
RESULTS: Of the 411 respondents, 68% intubated at their facility, representing 81 unique institutions. RTs who performed intubation were more likely to be from community hospitals and less likely to be from level 1 trauma centers. Respondents reported intubating adult (91%), pediatric (61%), and neonatal (65%) patients. The most common areas in which RTs reported performing intubation were the adult ICU (80%), emergency department (76%), outside the operating room for emergencies (76%), neonatal ICU (43%), the delivery room (45%), and pediatric ICU (25%). The median (interquartile range) number of supervised intubations required to be considered competent was 5 (3–5). The most common numbers of intubations required to be considered competent were 5 (32%), 3 (26%), 10 (16%), 2 (4%), and 0 (3%). The perceived number of intubations to achieve competence was 6 (range 5–10) and did not differ based on years of experience. Most respondents believed their RT intubation program was safe (93%) and effective (91%), and that RTs were well-trained (81%), that their intubation skills were objectively evaluated (66%), and that RTs receive sufficient feedback on performance (68%).
CONCLUSIONS: RTs in North Carolina frequently performed intubation and had high confidence in their programs. Further studies are needed to establish standardized training for endotracheal intubation, document success rates for intubations, and evaluate the use of video laryngoscopy by RTs.
- intubation
- airway management
- respiratory care practitioner
- respiratory therapist
- airway training
- endotracheal intubation
Introduction
Endotracheal intubation is a common procedure used to facilitate invasive mechanical ventilation, protect the airway, prepare patients for inter- or intrahospital transfer, and to facilitate invasive or painful procedures. Emergency intubation is often required for patients outside the ICU as a result of sudden or gradual physiologic deterioration. Emergency intubation is one of, if not the most, hazardous procedure a patient can undergo in the ICU and is associated with high complication rates, including severe hypoxemia, cardiac arrest, hemodynamic deterioration, aspiration, brain injury, and death.1 Intubation by respiratory therapists (RTs) has been described in a variety of settings, with a recent survey indicating that approximately 50% of respiratory therapy departments provide intubation.2-7
Historical data suggest that RTs provide a safe and effective intubation service, with the largest case series of 833 intubations noting a success rate of 95% with a complication rate of 12%.6 A neonatal case series also noted a success rate of 95%.5 RTs have a relatively high success rate of 90% when acting as a back-up when resident physicians failed to complete the procedure.7 RT success rates are similar to published case series among emergency medicine residents,8 critical care providers,9,10 and pre-hospital providers.11 It is difficult to compare the published RT data due to differences in reported outcomes because recent studies have focused largely on first-attempt success rate in contrast to RT studies, which focused on overall success rate.12-14 Importantly, available data published to date have been single-center case series of varying size and quality.
The most recent publication describing RT intubation clinical practice is from the year 2000, which predates the use of video laryngoscopy and the widespread adoption of noninvasive ventilation (NIV) and high-flow nasal cannula (HFNC). In particular, the number of intubations available for RTs has likely decreased due to an increasing number of intubations being performed by other clinicians, including emergency medicine providers, critical care physician trainees, and advanced practice providers. In addition, increasing use of NIV and HFNC has significantly decreased the number of patients who require intubation for respiratory failure.15-17 With fewer opportunities for RTs to develop and maintain their intubation skills, it is important to identify the amount of training and skill maintenance required for RTs. The primary purpose of this study is to describe current RT intubation practices in the state of North Carolina through the use of a survey instrument. A secondary purpose was to identify potential areas for quality improvement and to identify best practices throughout the state.
QUICK LOOK
Current knowledge
Endotracheal intubation is common procedure performed by respiratory therapists (RTs). Available studies to date have been single-center case series of varying size and quality. The primary purpose of this study was to describe current RT intubation practices in North Carolina. A secondary purpose was to identify potential areas for quality improvement and to identify best practices throughout the state.
What this paper contributes to our knowledge
RTs frequently performed intubation in North Carolina. The median number of intubations required to be certified was 5, with 76% of respondents reporting that ≤ 5 were required for certification. The vast majority of respondents indicated a high level of confidence in their intubation program. There were variances between RTs’ perceived competency requirements and the published competency requirements from other clinicians in the literature. Prospective, multicenter studies are needed to further evaluate RT intubation practice.
Methods
We developed a survey instrument in REDCap (Research Electronic Data Capture tools, hosted at Duke University Medical Center) after a literature search of RT intubation practices. The survey was sent to members of our department’s research committee and medical directors for review, and changes were made as appropriate. After receiving an exemption from the Duke University Medical Center Institutional Review Board, the survey was sent via email to all RTs with a license to practice in North Carolina. The email addresses of all licensed RTs as of February 8, 2019, were provided by the North Carolina Respiratory Care Board. The survey was kept open for 3 weeks, and no reminder emails were sent. Following questions on respondent and hospital demographics, the survey branched and ascertained whether RTs provided intubation at their facility. All respondents answered questions about intubation practices. Managers and directors of facilities where RTs intubated were asked additional questions about quality assurance strategies, success rate, first-attempt success rate and complication rate. The complete survey is included in the supplementary materials at http://www.rcjournal.com.
To evaluate training methods, one response from each center was used to reduce bias resulting from a large number of responses from a few centers. When there were multiple or conflicting responses, the response from the director/manager, clinical specialist/educator, clinical supervisor, or staff therapist were chosen in the order listed. Due to the high level of experience reported, we a priori divided respondents into < 2 y of experience, 2–5 y of experience, 6–9 y of experience, 10–20 y of experience, and > 20 y of experience to evaluate whether the perceived number of intubations needed to be considered competent differed based on experience. If there were only multiple responses from staff RTs, the respondent with the most experience was chosen. Statistical analyses were descriptive with comparisons between hospital demographics for RTs who intubate and those who do not. Agreement for number of intubations required to develop and maintain competency was evaluated. Data were analyzed using SPSS 25 (IBM, Armonk, New York). Continuous data were compared with nonparametric testing, and the chi-square test was used for categorical data. Statistical significance was set at α = 0.05.
Results
The survey was sent to a total of 4,817 licensed RTs; 101 emails were returned as being undeliverable, for a total of 4,716 potential respondents. The response rate was 9% (411 of 4,716). Twenty-two respondents were from outside of NC and were excluded. Of the remaining respondents, 264 (68%) provided intubation at their facility, representing 81 unique institutions. Further, 66% (81 of 123) of individual centers reported intubating. The number of responses from each institution ranged from 1 to 24. These institutions had a median (range) of 316 (100–900) beds, a median (interquartile range [IQR]) of 30 (15–80) RTs on staff, and were predominantly community facilities (206, 53%); academic facilities (62, 16%), level 1 trauma centers (89, 23%), tertiary (54, 14%) and quaternary (4, 1%). RTs who intubated were more likely to be from community hospitals (53% vs 36%, P= .001) and less likely (23% vs 35%, P= .01) to be from level 1 trauma centers. Respondent demographics are summarized in Table 1.
Respondent Demographics
There were responses from 81 unique institutions. Respondents defined an intubation attempt as an endotracheal tube passed through the mouth (48, 60%) or as a laryngoscope or any other device in the oropharynx (28, 34%); other/not answered responses totaled 5 (6%). Respondents reported that RTs at their institutions intubated adult (74, 91%), pediatric (49, 61%), and neonatal (53, 65%) patients. The most common areas in which RTs reported intubating were the adult ICU (65, 80%), the emergency department (62, 76%), the neonatal ICU (35, 43%), outside the operating room for emergencies (62, 76%), the delivery room (36, 45%), the pediatric ICU (20, 25%), and other (13, 16%). Reported training methods among institutions were classroom training (41, 51%), written materials (31, 38%), written test (22, 27%), skill demonstration in a simulation setting (69, 85%), and supervised intubations (58, 71%). Classroom training took a median of 4 (IQR 2–6) h and was taught predominantly by RTs. Topics across institutions covered included anatomy and physiology (62, 77%), pharmacology (46, 57%), positioning and pre-intubation preparation (73, 90%), difficult intubation predictors (63, 78%), equipment (70, 87%), techniques for direct laryngoscopy (64, 79%), techniques for video laryngoscopy (51, 63%), videos of intubations (27, 33%), and other (5, 6%).
Supervised intubations were performed in the operating room (43, 53%), ICU (55, 68%), emergency department (47, 58%), delivery room (23, 28%), and other (19, 24%). During training, RTs were observed by physicians (63, 78%), an RT supervisor or educator (45, 56%), advanced practice provider (27, 33%), physician and RT supervisor (12, 15%), or non-specified (9, 11%). The qualifications for intubation training were no minimum years of experience (67, 83%), demonstrated competency in basic airway management (73, 90%), Advanced Cardiac Life Support (ACLS) (66, 82%), Pediatric Advanced Life Support (48, 59%), Neonatal Resuscitation Program (50, 62%), baccalaureate degree (0, 0%), and advanced credentials, defined as Neonatal/Pediatric Specialist or Adult Critical Care Specialist (8, 10%). For institutions that required a minimum amount of experience, the median amount of experience was 3 (IQR 2–4) y. Annual competency was determined by automatic recertification if they completed a minimum number of intubations (51, 63%), pass a written test (11, 14%), classroom retraining (10, 12%), observed competency in the operating room (15, 19%), observed competency outside of the operating room (16, 20%), or observed competency in a simulation setting (24, 30%); other annual competency responses include “once RTs are certified they do not require recertification” (11, 14%) and other (3, 4%).
The median number of intubations required to be declared competent was 5 (IQR 3–5). The most common number of intubations required were 5 (32%), 3 (26%), 10 (16%), 2 (4%), and 0 (3%). Results are summarized in Figure 1. There were no differences in the reported or perceived number of intubations required when results were analyzed by years of experience. Results are summarized in Table 2.

Survey responses for the number of intubations required for competency at their institution. Note that the vast majority required ≤ 10 intubations.
Number of Intubations for Competence
Seven managers/directors answered questions about their quality assurance processes in place, with 4 (57%) having active QA processes in place. All reported defining an intubation attempt as an endotracheal tube passed through the mouth. Reported overall success rates were 100%, 94%, 91%, and 94%. First-attempt success rates were reported as 97%, 89%, 88%, and 92%, respectively. All 4 centers represented used chart review, and 3 (75%) required a quality assurance form to be filled out after each intubation. Respective complication rates were not reported, 5%, 1%, and not reported. Additional results are summarized in the supplementary materials at http://www.rcjournal.com. Attitudes about intubation practices are summarized in Figure 2.

Results of Likert scale of perception of respiratory therapist (RT) intubation programs.
Discussion
In this survey of RTs in North Carolina, 68% of RT respondents reported providing intubation, representing 81 unique institutions. Respondents who intubated were more likely to be from community hospitals, and these institutions were similar in size to centers that did not intubate. The median number of intubations required to be certified was 5, with 76% reporting that ≤ 5 were required for certification. A minimum level of experience was the exception, with 86% of respondents indicating there was no minimum amount of experience required prior to intubation training. A majority of respondents defined an intubation attempt as an endotracheal tube introduced in the mouth. The vast majority of respondents indicated a high level of confidence in their intubation program.
Intubation is a high-risk, low-volume procedure that requires substantial training and skill maintenance to perform safely.18,19 The survey yielded variable competency programs for intubation programs throughout the state. Training methods varied, with 27% of institutions requiring a written test and 38% providing written materials. Bishop et al20 reported that a high score on a written test was highly correlated with skill demonstration, whereas the number of intubations performed each year was not. Completing a minimum number of intubations was the most common recertification method reported by our respondents. The median reported number per year was 3, or an average of one intubation every 4 months. Only 51% of respondents reported that classroom training was part of their training. For those who did have classroom training, the median length was only 4 h, and didactic topics (eg, pharmacology, video laryngoscopy) were not reported to be consistently covered.
Although the specific number of intubations required to gain competence is currently unknown, available data suggest that the number of intubations required to achieve competence for direct laryngoscopy may be as high as 150 intubations.21 A systematic review found that at least 50 intubations were required by learners using direct laryngoscopy in the operating room before a success rate of 90% was achieved.21 Although that study did not include RTs, the majority of learners in the reported studies were novices, and the results are likely applicable to RT learners. In comparison, during training, Bucher et al22 reported that emergency medicine residents averaged 29 intubations per year (with one resident performing 157 intubations in 1 y), which is much higher than the number of intubation opportunities provided to RTs. Je et al23 reported that 74 intubations were needed for emergency medicine residents to achieve proficiency. A study of pediatric critical care fellows found approximately 51 intubations were required to achieve competence.10 Studies evaluating the number of intubations needed for competency have largely been performed in the operating room under controlled circumstances for both paramedic and medical students, but those studies did not include RTs.21 The number of intubations required for RTs to achieve competence is currently unknown; the largest case series to date required 10 supervised intubations and 8 h of classroom training, thresholds few of our respondents met.6 Importantly, this study predated the use of video laryngoscopy and did not perform subgroup analysis evaluating the safety of RTs providing intubation in trauma, children, neonates, or other specialty situations. This is a critical area for future research to ensure RTs who perform intubations have received adequate training and skill maintenance.
RTs reported frequently intubating during emergencies outside of the operating room. During emergencies, best practice suggests that only adequately trained personnel intubate, regardless of specialty.24 Only 9% of our respondents reported that the most experienced person performed intubations; however, 57% reported that any airway-certified RT made the first intubation attempt. Since our respondents indicated a high level of confidence in their RT intubation programs, it appears that the majority of respondents believed they had a competent person make the first attempt. Because time to intubation and the amount of time that chest compressions are interrupted both decrease with increasing intubation experience, having the most experienced personnel intubate should be strongly considered, although it may not be always be feasible due to a host of circumstances.25
RT intubation success rate and first-attempt success rate during chest compressions have not been published to date. Video laryngoscopy has also been described because it may improve first-attempt success rate, although this relationship is unclear and its use has not been studied in RTs.12,14,26,27 Given that 63% of respondents reported covering video laryngoscopy during their training, it appears that video laryngoscopy may not be widely utilized by RTs. We did not ask about video laryngoscopy use or other equipment specifically, in the interest of keeping the survey at a manageable length.
An important aspect of future studies is consensus on what constitutes an intubation attempt. For example, 48% of our respondents defined an attempt as an endotracheal tube being passed through the mouth. This is in direct contrast with published data that states a laryngoscope or other tool in the oropharynx defines an intubation attempt.8,9,12,21,26,27 To design future studies, agreement on what constitutes an attempt and controlling for individual training and experience are critical aspects to ensure a successful trial. Further data evaluating RT intubation practices are needed to identify quality improvement targets, optimize training methods, and provide higher-quality evidence supporting the role of RTs in providing intubation. Quality assurance and continuous quality improvement efforts are a critical part of any airway management program. We had responses from 7 managers, of whom only 4 had quality assurance processes in place. Combined with results from our prior data, in which only 57% of departments were engaging in quality assurance processes, there is a great opportunity for RTs to apply quality improvement methodology to intubation practice.4 Given the low number of responses from manager/directors, the rigor of current quality assurance processes could not be evaluated. A curriculum of twice monthly high-fidelity simulation in small groups as described by Mosier et al18 has the potential to be used as a model because they reported a significant improvement in critical care fellows intubation success rates. Importantly, over time they increased fellows’ first-attempt success rate to 90%.18
There are many limitations to our study. The respondents likely had special interest in intubation. The response rate was low, although respondents represented 81 unique institutions. As with all surveys, some questions may not have been worded clearly. There was a low number of manager/director responses, making comparison of success rates and complication rates across centers difficult. This study outlines intubation practices utilized in only a single state; a larger study is needed to determine RT intubation practices across the United States and internationally. This survey could potentially be used as a guide for future and larger studies.
Conclusions
RTs in North Carolina frequently provide intubation and report high confidence in their programs. There were variances between RTs’ perceived competency requirements and the published competency requirements from other clinicians in the literature. Prospective, multicenter studies are needed to establish the number of intubations required to achieve competence, to establish the safety of RTs intubating during cardiac arrests or other emergencies outside the ICU, to evaluate the use of video laryngoscopy, and to elucidate optimal training methods.
Footnotes
- Correspondence: Andrew G Miller MSc RRT RRT-ACCS RRT-NPS, Duke University Medical Center, 2301 Erwin Rd Durham, NC 27710. E-mail: andrew.g.miller{at}duke.edu
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}