

Abstract
BACKGROUND: Prone position (PP) has been widely used in the COVID-19 pandemic for ARDS management. However, the optimal length of a PP session is still controversial. This study aimed to evaluate the effects of prolonged versus standard PP duration in subjects with ARDS due to COVID-19.
METHODS: This was a single-center, randomized controlled, parallel, and open pilot trial including adult subjects diagnosed with severe ARDS due to COVID-19 receiving invasive mechanical ventilation that met criteria for PP between March–September 2021. Subjects were randomized to the intervention group of prolonged PP (48 h) versus the standard of care PP (∼16 h). The primary outcome variable for the trial was ventilator-free days (VFDs) to day 28.
RESULTS: We enrolled 60 subjects. VFDs were not significantly different in the standard PP group (18 [interquartile range [IQR] 0–23] VFDs vs 7.5 [IQR 0–19.0] VFDs; difference, −10.5 (95% CI −3.5 to 19.0, P = .08). Prolonged PP was associated with longer time to successful extubation in survivors (13.00 [IQR 8.75–26.00] d vs 8.00 [IQR 5.00–10.25] d; difference, 5 [95% CI 0–15], P = .001). Prolonged PP was also significantly associated with longer ICU stay (18.5 [IQR 11.8–25.3] d vs 11.50 [IQR 7.75–25.00] d, P = .050) and extended administration of neuromuscular blockers (12.50 [IQR 5.75–20.00] d vs 5.0 [IQR 2.0–14.5] d, P = .005). Prolonged PP was associated with significant muscular impairment according to lower Medical Research Council values (59.6 [IQR 59.1–60.0] vs 56.5 [IQR 54.1–58.9], P = .02).
CONCLUSIONS: Among subjects with severe ARDS due to COVID-19, there was no difference in 28-d VFDs between prolonged and standard PP strategy. However, prolonged PP was associated with a longer ICU stay, increased use of neuromuscular blockers, and greater muscular impairment. This suggests that prolonged PP is not superior to the current recommended standard of care.
Introduction
COVID-19 is an infectious disease that may cause viral pneumonia and respiratory failure.1 Patients with SARS-CoV-2 can develop ARDS, a syndrome defined by hypoxemic respiratory failure with bilateral infiltrates.2 Prone position (PP) has been part of respiratory management of moderate-to-severe ARDS for several years.3 Early application of PP in ARDS has been associated with an increase in oxygenation by improving ventilation/perfusion ratios4,-,7 compared to the supine position (SP). Additionally PP prevents ventilator-induced lung injury by reducing the overdistention of aerated non-dependent zones while allowing recruitment of gravity-dependent atelectasis.5,8,-,10 Two meta-analyses11-12 and the PROSEVA trial7 demonstrated the beneficial impact on mortality of PP in subjects with moderate-to-severe ARDS. Hence, PP plays a key role in the management of ARDS.13,14 Albeit, according to epidemiologic studies PP is used in < 20% of patients suffering from severe ARDS.15,16 Reports during the COVID-19 pandemic have shown an exponential adoption of PP, with a rate of use as high as 70%.17,18 However, the best moment to apply this ventilatory strategy and the optimum duration have not yet been established.
The landmark trial on PP7 demonstrated a mortality benefit in subjects with severe ARDS using 16-h prone sessions. Yet, there is evidence of beneficial physiological effects after 16 h of PP.19,-,21 Prolonged PP is safe and easy to implement when it is performed by trained staff, within an established protocol.22 Furthermore, increased duration of PP may reduce the rate of postural changes, which may subsequently decrease staff work load and cumulative exposure to SARS-CoV-2.22-25 However, prolonged PP may be associated with excessive use of neuromuscular blocking agents (NMBAs) and may delay mechanical ventilation weaning.
For these reasons, the pilot OptiMal pronE position LEngTh in patients with acuTE respiratory distress syndrome due to COVID-19 (OmeLEtte) randomized clinical trial was conducted, seeking to evaluate the effects of prolonged versus standard PP. The goal was to test the hypothesis that prolonged PP was superior based on beneficial time-dependent PP effects. Prolonged PP was compared to standard-of-care PP time, measured by the number of days alive and free from mechanical ventilation during the first 28 d of in-patient hospitalization.
QUICK LOOK
Current knowledge
Prone position (PP) reduces mortality in moderate-to-severe ARDS. However, the optimum length of time to apply this strategy and the optimum duration have not yet been established by clinical studies.
What this paper contributes to our knowledge
In a single-center clinical trial, a standard duration strategy of PP ventilation versus prolonged prone position was associated with reduced time to successful extubation in survivors, as well as shorter ICU stay and less muscular impairment.
Methods
This was a randomized controlled, parallel, and open clinical trial conducted in the medical-surgical ICU of a tertiary referral hospital in Madrid, Spain, from March–September 2021. Study approval was authorized by the local ethics committee (Comité Ético de Investigación Clínica, Instituto de Investigación Hospital 12 de Octubre; Reference CEIm 21/116). Written consent to participate in the study was obtained from all subjects or their next of kin after receiving verbal and written information about the research. The study protocol was registered on ClinicalTrials.gov before the first subject enrollment (NCT05012267). The study met the Consolidated Standards of Reporting Trials (CONSORT) Statement for Randomized Trials of Non-pharmacologic Treatments.26
Subjects > 18 y who fit the following criteria were included: ARDS due to COVID-19 as defined according to the ARDS Berlin definition27 and invasive mechanical ventilation and indication of PP according to the PROSEVA study7 criteria (PaO2/FIO2 < 150 mm Hg, with an FIO2 ≥ 0.6, and PEEP ≥ 5 cm H2O) despite fluid restriction, NMBAs, and optimal PEEP levels. Exclusion criteria were contraindications to PP ventilation (increased intracranial or intra-abdominal pressure; massive hemoptysis; recent tracheal surgery or sternotomy; unstable hemodynamic status; recent pacemaker implantation; severe facial laceration; open abdominal wound; spine, femur, or pelvis fracture; or pregnancy), limitation of life-sustaining care, and high probability of death during the following 24 h in the ICU. Subjects were randomized within 24 h of admission to the ICU. The screening process and the non-pharmacologic interventions were performed by the ICU staff.
Randomization and Allocation
Unrestricted randomization was performed by sequentially numbered, opaque sealed envelopes. A professional who was external to the research team carried out this process. The envelopes were opened only after they had been irreversibly assigned to the participants. Subjects were randomly allocated in 2 groups: standard PP (∼16 h), while the intervention group received prolonged PP (48 h).
Procedures
Respiratory management.
No changes were made to the written protocol used routinely in our unit. Subjects were ventilated with a 6–8-mL/kg tidal volume (VT), and PEEP was applied according to highest static compliance (C). The levels of PEEP and VT were adjusted to maintain the inspiratory plateau pressure < 30 cm H2O. Weaning from mechanical ventilation was conducted in the same way for both study groups according to the unit protocol. All subjects had an arterial line catheter and were ventilated with either a Servo-i or Servo-u ventilator (Getinge, Göteborg, Sweden), a Carescape R860 ventilator (GE Healthcare, Madison, Wisconsin), or an Evita XL ventilator (Dräger, Lübeck, Germany).
Prone position.
PP maneuvers in our unit were conducted as follows:28 The switch from SP to PP usually required a team of 6 people. Prior to the maneuver, there was a team briefing to identify each member’s role, check the security of endotracheal tube and intravascular catheters, and decide the side of the upturn. Standard monitoring during the procedure included pulse oximetry and invasive arterial blood pressure. The head and the neck protruded from the sheet surface to allow proper management of the airway. A reverse Trendelenburg position (10°) was applied to decrease facial edema and the risk of intra-abdominal hypertension. Subjects were placed with arms parallel to their torso; the abdomen was unsupported, and their face turned to the right or the left side. Postural changes were performed every 2 h. The subject’s chest and pelvis were supported to guarantee abdominal suspension.
Criteria for stopping PP treatment:
Intervention group: After 48 h.
Standard PP group: Any time after 16 h if there was an improvement in oxygenation (defined as a PaO2/FIO2 ≥ 150 mm Hg, with an FIO2 ≤ 0.6 regardless of PEEP level).
In both groups: Whenever a complication occurred. Complications leading to the immediate interruption of prone treatment included unplanned extubation, main-stem bronchus intubation, endotracheal tube obstruction, hemoptysis, cardiac arrest, and any other life-threatening reason for which the clinician decided to stop the treatment.
Subsequent PP sessions.
In both groups, PP was continued if subjects continued to fulfill the criteria indicating therapy (PaO2/FIO2 < 150 mm Hg, with an FIO2 ≥ 0.6, and PEEP levels ≥ 5 cm H2O), with no exclusion criteria met.
Sedation and nutrition support.
A sedation protocol based on midazolam and morphine was used. During PP, all subjects received a continuous infusion of cisatracurium to achieve train of four response of 1–2. Nutrition support followed local protocol as previously described.28
Measurements
Demographic variables, admission diagnosis, and severity scores (Acute Physiologic and Chronic Health Evaluation II score and Simplified Acute Physiology Score II [SAPS II]) were documented on ICU admission. The number of PP sessions and their duration were recorded. Associated ICU treatments, such as duration of mechanical ventilation, vasopressors, tracheostomy, renal replacement therapy, extracorporeal membrane oxygenation, corticosteroids, and NMBAs, were detailed as well as subject outcomes.
Pulmonary mechanics and arterial blood gas were recorded at 5 different study times: (1) prior to pronation (baseline), (2) during the first hour after the pronation, (3) during the last hour before supination, (4) within the first hour after turning the subject back to SP, and (5) 12 h after supination with the condition that the subject remained in SP. At each time point, end-inspiratory and end-expiratory airway occlusion maneuvers were performed; arterial blood samples were drawn in 3-mL heparinized syringes, and gas exchange was monitored by blood gas bedside analyzers (GEM Premier 3000, model 5700, Instrumentation Laboratory, Lexington, Massachusetts).
Static values were recorded and calculated in these periods to obtain the following variables: C, calculated as the ratio between VT and airway driving pressure (ΔP); PaO2/FIO2; corrected minute ventilation;29 and ventilatory ratio (VR)30 as previously described. Mechanical power (MP) was calculated according to the formula:31

MP is expressed in J/min, the VT in L, breathing frequency in breaths/min, and peak pressure and ΔP in cm H2O.
Subjects were defined as O2-responders if they had an increase in the PaO2/FIO2 ≥ 20 mm Hg compared to baseline values in SP (study time 1).32,33 Moreover, to evaluate time-dependent effect, responders were defined as having a change between baseline values and end-session values (during the last hour before supination) < 0% according to the expected physiological effect and CO2-responders if their VR was reduced during prone ventilation, as assessed by ΔVR < 0%; ΔP-responders were assessed by ΔP < 0%; MP-responders were assessed by ΔMP < 0%. Each subject could be a responder for one parameter independently of the response to other parameters.
Successful extubation was defined as no re-intubation or use of noninvasive ventilation in the 48 h after extubation. In subjects who had undergone a tracheostomy, successful weaning from the ventilator was defined as the ability to breathe unassisted through the tracheostomy cannula for at least 24 h.
Complications related to PP were studied. The evaluation of cutaneous pressure lesions was carried out daily by the nursing staff using the classification of the National Pressure Injury Advisory Panel (https://npiap.com, Accessed March 15, 2024). The development of pneumothorax or ventilator-associated pneumonia was evaluated by chest radiography. Displacement and accidental withdrawal of the orotracheal tube were also registered.
A follow-up appointment was arranged for all subjects at 6 months after ICU discharge. This consultation included anamnesis and an assessment of potentially affected domains where post–intensive care syndrome (PICS) was evaluated: mental status, cognition, muscle strength, pulmonary function, dependence, and functional status. All variables related to this assessment were prospectively recorded. PICS diagnosis was considered when at least one anomalous result in the next items was present at 6-months post-ICU discharge: weight loss > 5%, mild or moderate dyspnea (modified Medical Research Council [mMRC] questionnaire > 1),34 deranged quality of life (EuroQol-5 Dimension questionnaire < 80),35 muscle weakness measured by a total mMRC muscle testing grading system < 48,36 dysphagia, deficient performance in activities of day living (Barthel questionnaire < 100),37 or altered mental state (Pfeiffer questionnaire < 100).38
Outcome Measures
Ventilator-free days (VFDs) through day 28 was the primary end point. Hospitalized subjects who died before day 28 were considered to have 0 VFDs. Secondary end points included ICU mortality, time to successful extubation, length of sedation and NMBAs, ICU length of stay (LOS), hospital LOS, rate of PP complications, and measurements of arterial blood gas and respiratory system mechanics during PP.
Statistical Analysis
This pilot study was, therefore, designed to gain more knowledge on this specific area to design future prospective multi-center studies. The number of subjects included was arbitrarily set for this trial at 60, as there were no prior randomized controlled trials comparing PP duration to use as reference at the time of study design.
Statistical analyses were performed with SPSS Statistics 25.0 (IBM, Armonk, New York). The data were prospectively collected in a specifically designed database enabling blinded data collection. Qualitative variables were described with absolute frequency and relative percentages. Quantitative variables were expressed with mean and SD or median and corresponding interquartile range (IQR). A P value of ≤ .05 (2 sided) was considered significant. After demonstrating a non-normal distribution of data, differences among groups were compared using Mann-Whitney-Wilcoxon test for continuous variables or Pearson chi-square test for categorical variables. Kaplan-Meier curves were plotted for time to death and unassisted breathing.
After bivariate analysis, multivariable logistic analysis and linear regression analysis were employed to assess the association between baselines variables and 28-d mortality or duration of mechanical ventilation, respectively. Variables with a P value of ≤ .20 in the bivariate analysis were considered for inclusion in the multivariable logistic regression analysis. Regarding PP maneuver analysis, Friedman test was used to detect significant changes in arterial blood gas and lung mechanics across the 5 study points during the different PP sessions. Post hoc analysis with Wilcoxon signed-rank tests was conducted with a Bonferroni correction applied for multiple comparisons, resulting in a significance level set at P < .005. Mann-Whitney rank-sum test was used to compare nonparametric continuous variables between study groups. Chi-square test or Fisher exact test was used for categorical variables.
Results
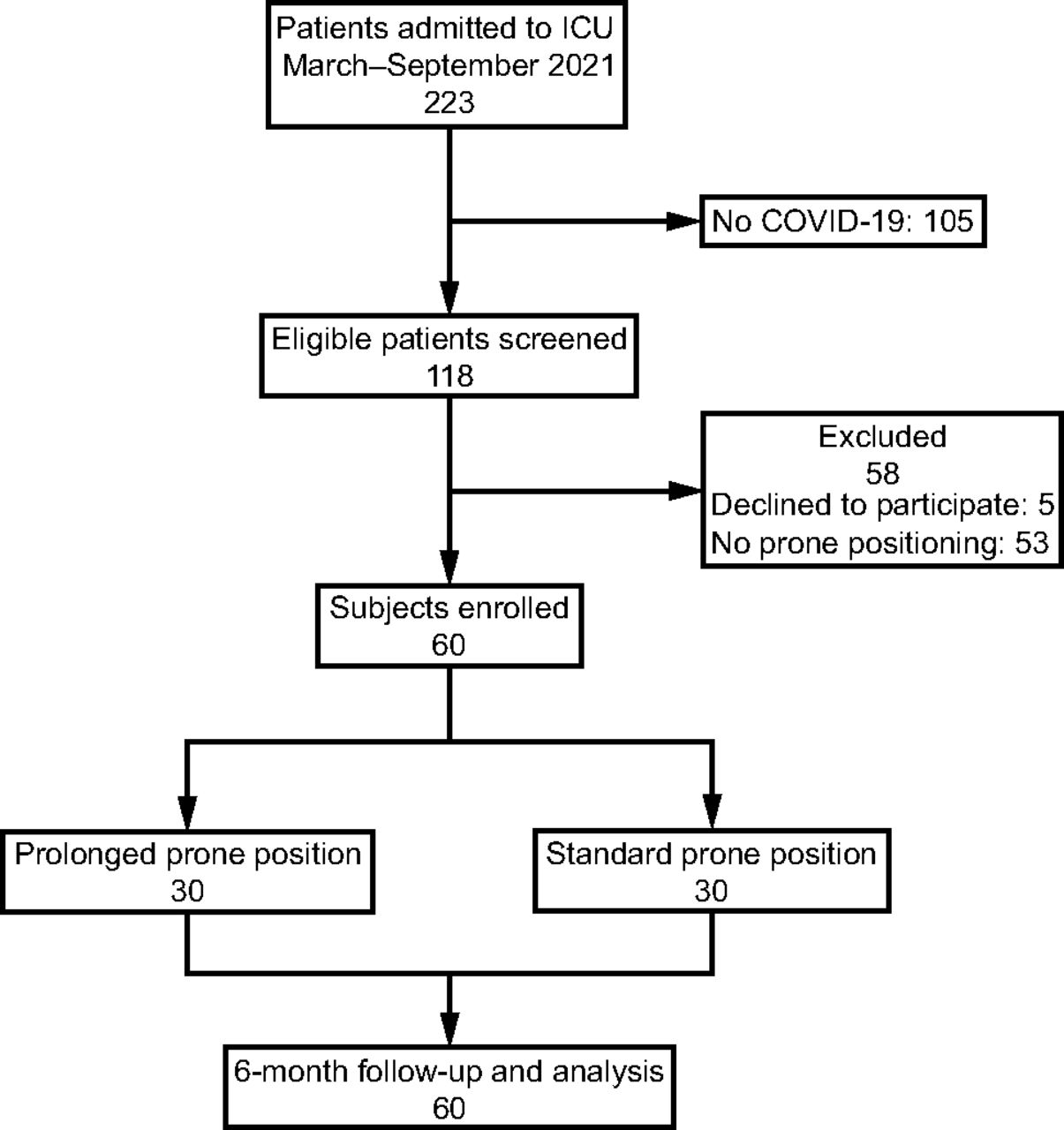
From March 1, 2021–September 30, 2021, 223 patients were admitted to the ICU, 118 of which tested COVID-19 positive (Fig. 1). Fifty-eight patients were excluded according to study criteria. Sixty subjects underwent randomization and were included in the analysis: 30 in the prolonged PP group and 30 in the standard PP group. Baseline characteristics of subjects are presented in Table 1. On inclusion, subjects in both groups had similar baseline characteristics, except for age. Number of PP sessions were similar in both groups (2 [IQR 1–3] vs 2.00 [IQR 1–3], P = .29) with significant differences in median total duration of PP (32 [IQR 16–58] h vs 96 [IQR 48–156] h, P < .001). Baseline ventilator settings, respiratory system mechanics, and results of arterial blood gas measurements were also similar between groups (Table 1).

Flow chart.
Baseline Characteristics at Admission to the ICU
Primary and Secondary Outcomes
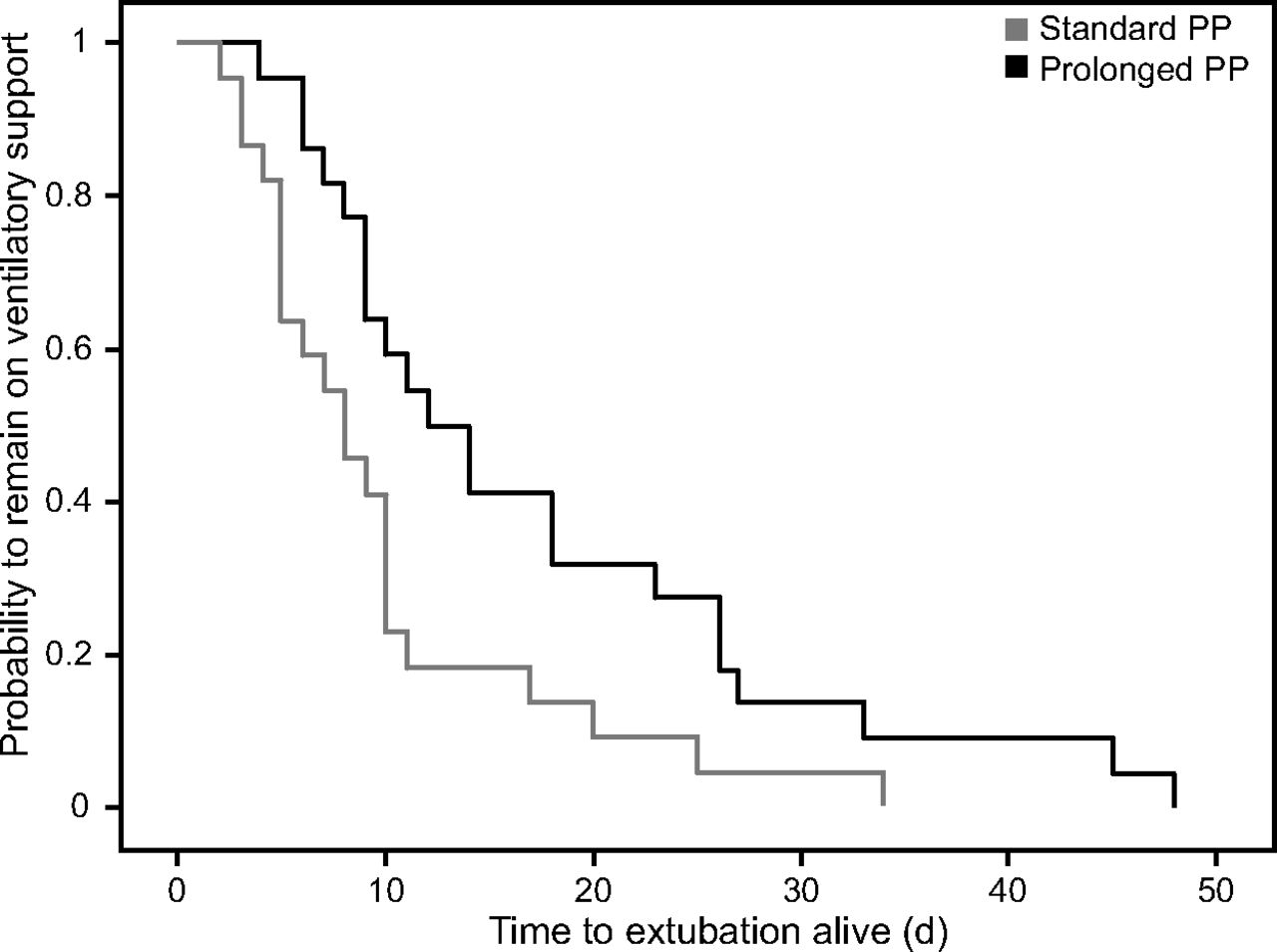
Subject outcomes are shown in Table 2. The primary composite outcome of VFDs to day 28 was not significantly different in the standard PP group compared with the prolonged PP group (18 [IQR 0–23] VFDs vs 7.5 [IQR 0–19.0] VFDs; difference, −10.5 [95% CI −3.5 to 19.0], P = .08). The difference in primary outcome was largely attributable to a shorter time to successful extubation in survivors (8.00 [IQR 5.00–10.25] d versus 13.00 [IQR 8.75–26.00] d; difference, −5 [95% CI −15 to 0], P = .001), whereas 28-d mortality was similar between the groups (10% vs 20%, P = .30). The results of bivariate and multivariate analyses of risk factors predicting 28-d mortality are shown in Table S1 (see related supplementary materials at http://www.rcjournal.com). Multivariate analysis indicated that SAPS II score was the only baseline variable significantly associated with 28-d mortality. A comparison of the two survival curves showed subjects in the standard PP group had a lower probability of remaining on ventilatory support (P = .02) (Fig. 2). After adjustment for age, body mass index, and sex at the time of inclusion, duration of mechanical ventilation remained significantly shorter in the standard PP group (Fig. 3).

Kaplan-Meier plot of the probability of remaining on ventilatory support. Log rank was used to compare the curves, P = .02. PP = prone position.

Forest plot from multiple linear regression analysis of duration of mechanical ventilation. β coefficients of single independent variables are pictured as black squares with their corresponding 95% CI. BMI = body mass index; PP = prone position.
Primary and Secondary Outcomes According to Study Group
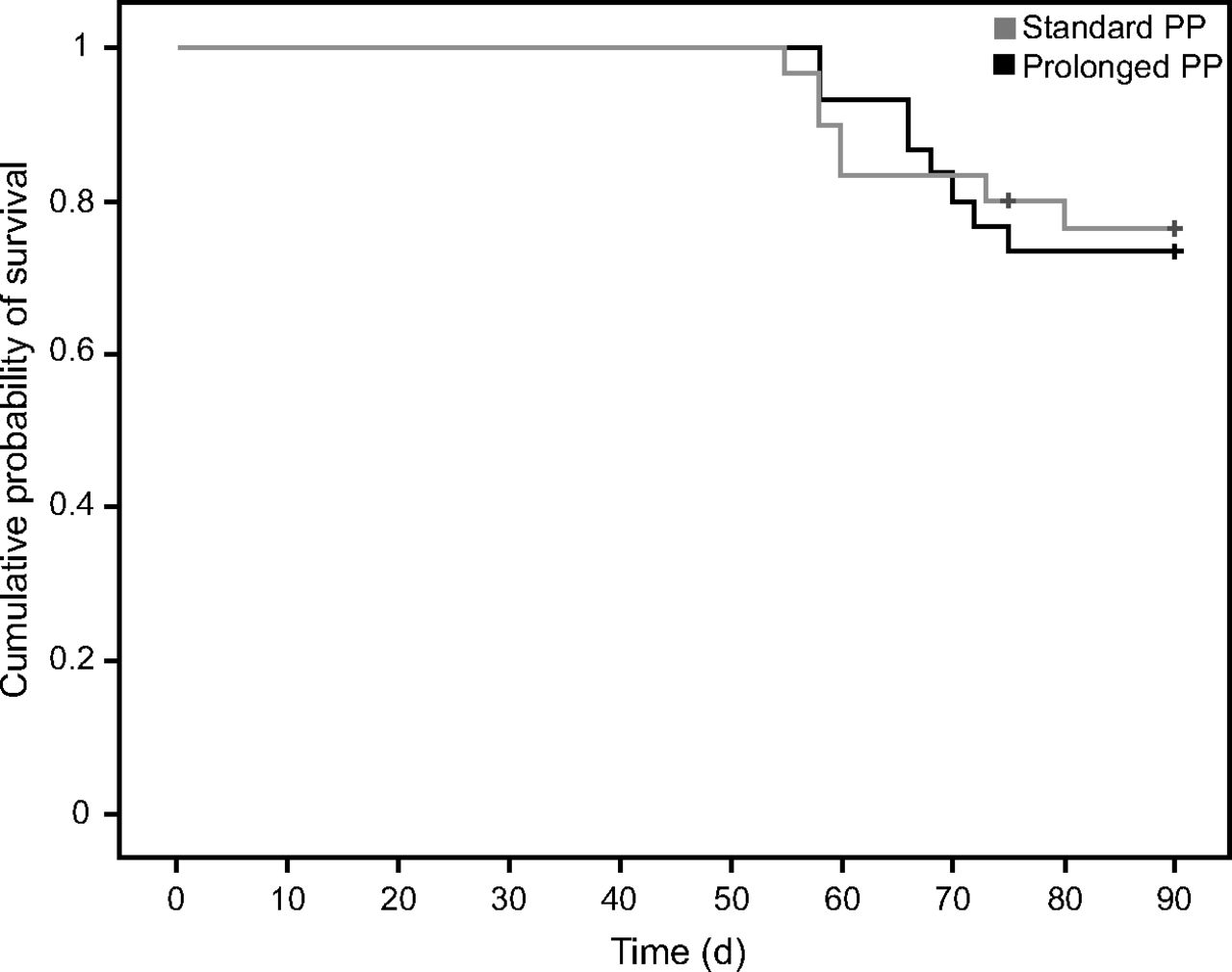
There were no differences in 90-d mortality (Fig. 4), need for tracheostomy, or support with venovenous extracorporeal membrane oxygenation. Nevertheless, prolonged PP was significantly associated with longer ICU LOS (18.5 [IQR 11.8–25.3] d vs 11.50 [IQR 7.75–25.00] d, P = .050) and extended administration of NMBAs (12.50 [IQR 5.75–20.00] d vs 5.0 [IQR 2.0–14.5] d, P = .005). At the 6-month follow-up, 40 subjects (66.7%) met PICS criteria with significant differences between study groups (15 subjects in the standard PP group vs 27 subjects in the prolonged PP group, P = .040). Physical, cognitive, and psychiatric assessments are shown in Table 3. Prolonged PP was associated with significant muscular impairment according to lower mMRC values (59.6 [IQR 59.1–60.0] vs 56.5 [IQR 54.1–58.9], P = .02).

Kaplan-Meier plot of the probability of survival from randomization to day 90. Log rank was used to compare the curves, P = .28. PP = prone position.
Prone Position and Post–Intensive Care Syndrome
Displacements of the arterial line, central venous line, or orotracheal tube were not observed while changing position or during PP. Grade 1–2 pressure wounds on the face (n = 20, 33.3%), chest (n = 21, 35%), and hips (n = 15, 25%) were relatively common. There were significant differences in all these wounds between study groups, finding higher rates in the prolonged PP group (Table 4). Eighteen subjects (30%) developed ventilator-associated pneumonia during their ICU stay, without significant differences between study groups (11 subjects [36%] in the prolonged PP group vs 7 subjects [23%] in the standard PP group, P = .39). No subject developed hemodynamic instability or cardiac arrest during pronation/supination.
Anatomical Localization of Pressure Wounds
Ventilator Settings and Lung Function
The evolution of lung mechanics over time along with arterial blood gas and ventilator settings during the first PP maneuver is specified in Table 5, while differences between study groups are recorded in Table 6. Subject progression during the second PP maneuver and the third or more PP maneuvers is presented in the supplementary files (see related supplementary materials at http://www.rcjournal.com). At the end of the first PP session, subjects globally showed a significant increase in pH, C, and PaO2/FIO2 with a significant decrease in ΔP. As for successive maneuvers, only the PaO2/FIO2 after re-supination remained significantly higher compared to baseline values, with no differences in lung mechanics.
Arterial Blood Gas and Lung Mechanics During the First Prone Position Session
Response to First Prone Position Session Between Study Groups
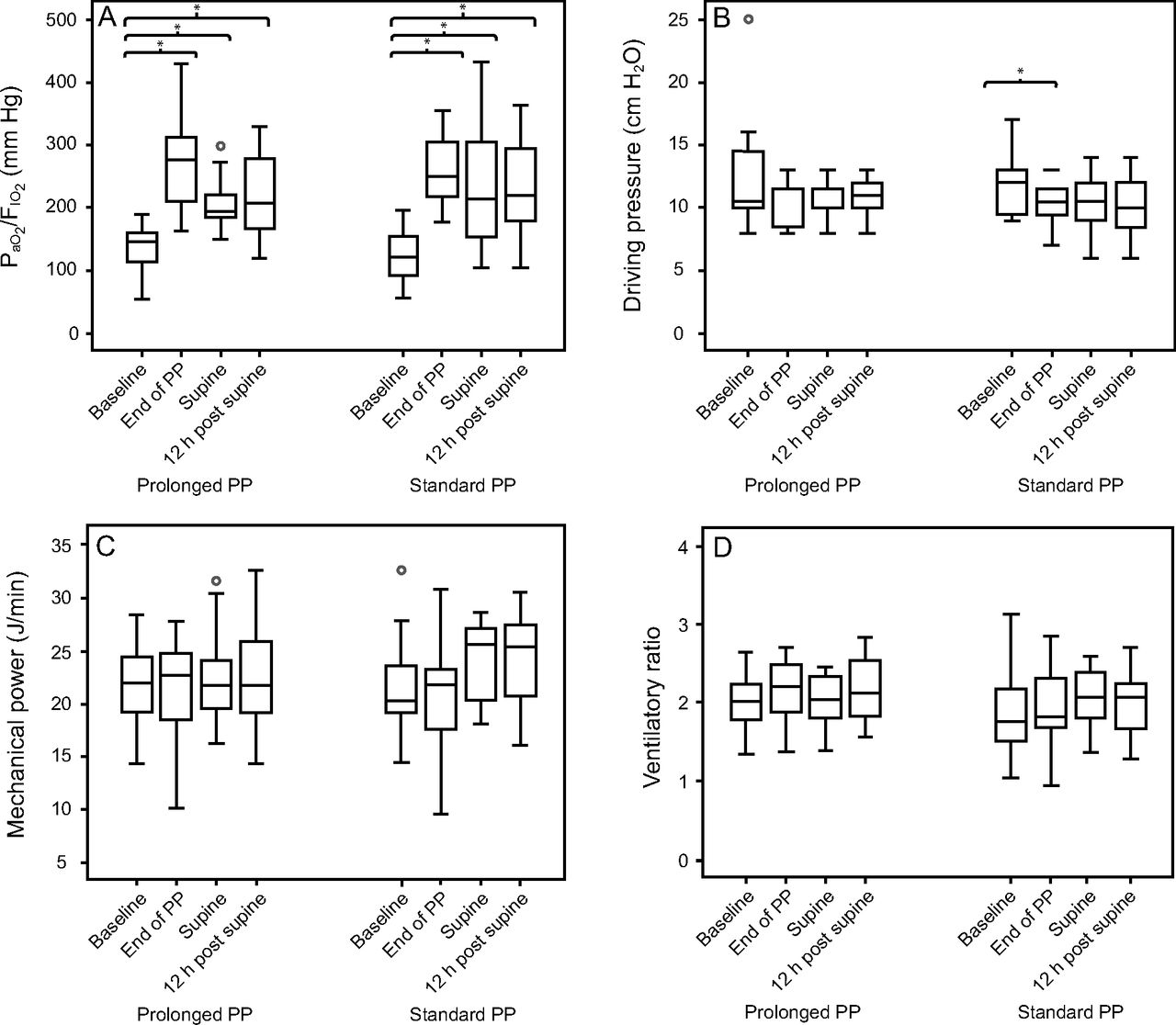
In the first PP session, there was a similar tendency in O2-responders, ΔP-responders, and MP-responders, achieving higher response rates immediately after PP (responder rates of 95, 73.3, and 47.2%, respectively) and progressively decreasing until stabilization was reached 12 h after SP, with responder rates of 81.6, 51.5, and 35%, respectively. VR-responders exhibited an inverse behavior, slightly increasing its value during the different study time-points (Fig. 5). There were no differences between groups at any of the study time points regarding these ventilatory variables. On average, PaO2/FIO2 after re-supination at the end of the second or more PP sessions remained significantly higher as compared to baseline values but with reduced responder rates after 12 h of PP compared to the first maneuver. Other variables evolved similarly, exhibiting responder rates around 50% in the consecutive PP sessions.

Post hoc analysis with Wilcoxon signed-rank tests of the physiological parameters changes during the first session of prone position (PP) between study groups at baseline, end of PP, supine position (SP), and 12 h after SP. *P < .005 after applying a Bonferroni correction for multiple comparisons compared to baseline value (before PP). PP = prone position.
Discussion
In this single-center, randomized controlled study involving 60 adults with severe ARDS due to COVID-19, the use of standard or prolonged PP resulted in a similar number of days alive and free of mechanical ventilation during the first 28 d. Subjects who received standard PP were extubated earlier, had shorter ICU LOS, and received less NMBAs compared with those who were included in the prolonged PP group. Pressure injuries and PICS incidence were also lower in the standard PP group.
Since the landmark trial on mechanical ventilation with PP,7 it is well known that PP in patients with severe ARDS is associated with improved survival. However, the optimal duration of PP has not been established. Amid the COVID-19 pandemic, different retrospective studies23,24,39,40 and one clinical trial25 addressed the possibility and feasibility of prolonged PP to reduce staff work load and decrease the risk of staff infection. Instead of focusing on PP complications, we analyzed clinical implications of a standard versus prolonged PP strategy, choosing VFDs as the primary outcome of the study. Despite not reaching statistical significance, we found differences favoring a standard PP strategy gaining 10 VFDs in the standard PP group. This difference was driven by a 5-d absolute reduction of time to extubation among subjects in the standard PP group. There were no detectable differences in mortality between groups.
One possible explanation for the absence of impact on mortality could be the low 28-d mortality rate in our study compared to previously published research (27% to 44%).17,39,41 We performed our study between the third and fourth COVID-19 waves in Spain, whereas most of the previous studies were conducted during the first wave. The reduced mortality rate could be attributable to a better understanding of the disease with significant treatment modifications, as well as sufficient available resources and an improved identification of patients at high risk of invasive respiratory support.
Besides the overall low mortality rate, the absence of significant differences in mortality between groups may be influenced by the small sample size. Morbidity outcomes are expected to be more sensitive than mortality and thus require a smaller sample size in order to demonstrate that an intervention has a statistically significant impact.42 The main finding of our study was the reduction in mechanical ventilation duration using a standard PP strategy. Whereas time to successful extubation in the prolonged PP group was slightly shorter to what was previously described in subjects with severe ARDS7 or specific subjects with COVID-19,18,39 a strategy of standard PP in our study was associated with a 5-d absolute reduction of time to extubation in survivors.
To explain this finding, first we analyzed the pathophysiologic respiratory effects of PP. The improvement in oxygenation and mechanical parameters observed after the first PP session is in line with those reported in other studies, with a significant increase of the PaO2/FIO2 between pre PP and post SP.18,24,40 We used an increase in PaO2/FIO2 during pronation of at least 20 mm Hg as cutoff to define the response to PP in terms of oxygenation. Using this definition, 82% of subjects were considered O2-responders after the first maneuver. When looking at the literature using the same cutoff, the percentage of O2-responders seems similar to previously reported in COVID-19–induced ARDS18 or in general ARDS population.32,33 Additionally, we found a significant increase in C and a modest decrease in ΔP after the first PP, which is consistent with what is known in the classic non–COVID-19 ARDS.43
However, there were no differences in respiratory benefits between both study groups 12 h after each SP. Immediately following PP, most subjects had significantly improved oxygenation, but it seems that in O2 responders the beneficial effect of PP did not continue to increase after 16 h. In fact, both study groups required a similar number of PP sessions, unlike other uncontrolled studies that suggested an inverse relation between duration of prone sessions and number of sessions required.39
In our study, subjects under PP received a continuous NMBAs infusion during the whole session. Therefore, subjects in the standard PP group received significantly fewer days of deep sedation and NMBAs, which may be the key factor in the reduced duration of mechanical ventilation and ICU LOS of this study group. Sedation and prolonged mechanical ventilation are well-known risk factors for PICS,34 contributing to a higher incidence in subjects of the prolonged PP group.
PP-related adverse effects were uncommon except for pressure sores on the ventral body surface, with a rate comparable to that reported in the PROSEVA trial7,44 or other previous experiences,24,39 which have shown that most prone-related pressure ulcers are grade 1–2. Even though the incidence was low, we found significant differences favoring a standard PP strategy. Therefore, it does not seem logical to prolong PP sessions, since it is unclear that it will be beneficial from a respiratory standpoint and is potentially harmful in other aspects.
Limitations
This study has several limitations. First, the non-blinded design might have introduced bias. Second, this was a single-center study with a small sample size, so the study may have been underpowered to exclude a clinically meaningful difference between groups. To our knowledge, this is the first interventional trial testing these PP strategies; and therefore, there were no previous data available to facilitate a power calculation. Finally, a large proportion of adverse events associated to PP in our study may be related to deep sedation and NMBAs, so results could be different in centers that do not routinely use paralytics in PP.
Conclusions
Among subjects with severe ARDS due to COVID-19, a standard PP strategy, compared with a prolonged PP strategy, did not improve 28-d VFDs. However, the standard duration of PP was associated with a shorter ICU LOS, a decreased use of NMBAs, and less muscular impairment on follow-up. More extensive studies are required to confirm our findings.
Acknowledgments
We would like to thank everyone who contributed to this paper. In particular, we want to acknowledge all the staff of the medical ICU of the Hospital 12 de Octubre.
Footnotes
- Correspondence: Ignacio Sáez de la Fuente MD, Department of Critical Care. Hospital Universitario 12 de Octubre. Avenida de Córdoba s/n, 28041, Madrid, Spain. E-mail: Ignacio.saez{at}salud.madrid.org
The authors have disclosed no conflicts of interest.
This paper was presented at ESICM LIVES 40, held May 12–14, 2022, in Madrid, Spain; at LVII National Congress of the Spanish Society of Intensive and Critical Medicine and Coronary Units, held June 12–15, 2022, in Seville, Spain; and at ESICM LIVES 2022 Annual Congress, held October 24–26, 2022, in Paris, France.
Supplementary material related to this paper is available at http://www.rcjournal.com.
See the Related Editorial on Page 911
- Copyright © 2024 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}