

Abstract
BACKGROUND: Expiratory positive airway pressure (EPAP) is a form of noninvasive positive-pressure ventilatory support that, in spite of not unloading respiratory muscles during inspiration, may reduce the inspiratory threshold load and attenuate expiratory dynamic airway compression, contributing to reduced expiratory air-flow limitation in patients with COPD. We sought to determine the effects of EPAP on operational lung volumes during exercise in COPD patients.
METHODS: This was a nonrandomized, experimental comparison of 2 exercise conditions (with and without EPAP); subjects completed a treadmill exercise test and performed, before and immediately after exercise, lung volume measurements. Those who overtly developed dynamic hyperinflation (DH), as defined by at least a 15% reduction from pre-exercise inspiratory capacity (IC), were invited for an additional research visit to repeat the same exercise protocol while receiving EPAP through a spring loaded resistor face mask. The primary outcome was IC variance (pre-post exercise) comparison under the 2 exercise conditions.
RESULTS: Forty-six subjects (32 males), a mean 65.0 ± 8.2 years of age, and with moderate to severe COPD (FEV1 = 38 ± 16% predicted) were initially enrolled. From this initial sample, 17 (37%) presented overt DH, as previously defined. No significant difference was found between these subjects and the rest of the initial sample. Comparing before and after exercise, there was significantly less reduction in IC observed when EPAP was used (−0.18 ± 0.35 L vs −0.57 ± 0.45 L, P = .02), allowing greater IC final values (1.45 ± 0.50 L vs 1.13 ± 0.52 L, P = .02).
CONCLUSIONS: The application of EPAP reduced DH, as shown by lower operational lung volumes after submaximal exercise in COPD patients who previously manifested exercise DH.
Introduction
The clinical hallmark of patients with COPD is exercise intolerance, the mechanisms of which are complex and multifactorial.1 However, changes in the mechanics of ventilation during exercise play a major role in exercise intolerance.2,3 A key concept is that activity limitation in these patients is linked to hyperinflation, particularly dynamic hyperinflation (DH),4 and reducing operational lung volumes in patients with COPD through pharmacologic (bronchodilators) and non-pharmacologic means (inhaled oxygen and oxygen/helium mixtures, rehabilitation exercise training) has proved to be an efficient strategy for improving their exercise tolerance and activity.5
Noninvasive ventilation (NIV) has been used as an aid to improve exercise tolerance in COPD patients.6–8 The rationale for NIV is to assist exercise performance. Considering the intrinsic mechanical loading and probable functional inspiratory muscle weakness in COPD, assisted ventilation should provide symptomatic benefit by unloading and assisting such overburdened ventilatory muscles.9 Among NIV modalities, expiratory positive airway pressure (EPAP), in spite of not unloading respiratory muscles during inspiration, represents the simplest strategy and can be offered by less costly and elementary devices. The EPAP technique is believed to move the equal pressure point to more central and solid airways. Both increases and decreases of pulmonary volumes have been described in COPD patients.10 This may be one of the explanations why pursed-lip breathing, a type of breathing resulting in positive expiratory pressure and thought to have similarities with EPAP, is spontaneously adopted by many patients.11 Theoretically, EPAP could alleviate dynamic compression on expiration, attenuating expiratory air-flow limitation11 and reduce the inspiratory threshold load of hyperinflated lungs in COPD patients, promoting an enhancement in neuromuscular coupling.9 On the other hand, a resistance during expiration may be accompanied by an increase in lung volumes,12 an undesirable effect in subjects whose lungs tend to be already hyperinflated. Previous studies that applied continuous positive airway pressure (CPAP) in COPD patients during exercise demonstrated improvement in exercise endurance13 and reduction of inspiratory muscle effort14 and dyspnea.13–15 Therefore, this study aimed to evaluate the effects of EPAP delivered by a spring loaded resistor face mask on operational lung volumes during exercise in patients with moderate to severe COPD who overtly developed effort related DH.
QUICK LOOK
Current knowledge
Activity in COPD patients is limited by the development of dynamic hyperinflation. Changes in respiratory mechanics during exercise in patients with dynamic hyperinflation leads to exercise intolerance.
What this paper contributes to our knowledge
The use of expiratory positive airway pressure during submaximal exercise may promote a reduction in the development of dynamic hyperinflation in COPD patients. The clinical impact of this reduction remains unanswered.
Methods
Subjects
Fifty-one men and women with moderate to very severe COPD, according to the Global Initiative for Chronic Obstructive Lung Disease criteria,16 able to perform treadmill exercise tests, and free from other substantial disease potentially contributing to exercise limitation were recruited from the pulmonary clinic at a tertiary-care university hospital. All patients of this convenience sample were clinically stable (during the 8 week period prior to the study) and receiving appropriate standard therapy with long-acting bronchodilators. Those with FEV1 < 50% of predicted were receiving inhaled steroids plus long-acting bronchodilators.16 Exclusion criteria included: cardiovascular system contraindications for exercise, long-term oxygen therapy or arterial oxygen saturation < 85% at rest, use of oral corticosteroids or antihistamines, and changes in chronic inhaled therapy. Incapacity to complete the exercise test protocol was also considered an exclusion criterion. The study was approved by the ethics committee of the Clinical Hospital of Porto Alegre, project approval number 05–449, and all subjects gave written informed consent.
Study Design
From January to June 2008, after a screening visit for clinical evaluation (Visit 1), all participants completed pulmonary function tests that included spirometry, lung volumes measurements, and lung diffusion capacity for carbon monoxide (DLCO). During Visit 2, subjects performed treadmill exercise test, and lung function tests were performed before (post-bronchodilator, salbutamol 400 μg) and immediately after exercise (up to 2 min maximum between the exercise and the pulmonary function test). The plethysmographic box was 8 meters from the treadmill, in the same room. For subjects who developed substantial DH (n = 17), as defined by at least a 15% reduction from pre-exercise inspiratory capacity (IC),3 a third research visit (Visit 3) was planned. At this point, subjects had to repeat the treadmill exercise test, with the same speed and grade protocol performed in Visit 2, using the spring loaded resistor face mask during exercise. Similarly, lung function measurements were performed before and immediately after exercise cessation (Fig. 1). Prescribed long-acting bronchodilators were suspended 24 hours before Visits 2 and 3, and short-acting bronchodilators were used just before the exercise tests.

Study design. Only the patients who presented a 15% reduction in inspiratory capacity after exercise test during Visit 2 were asked to Visit 3. EPAP = expiratory positive expiratory pressure. PFTs = pulmonary function tests.
Procedures
Pulmonary Function Tests.
Spirometric tests were performed using a computerized system (Eric Jaeger, Friedberg, Germany), according to American Thoracic Society recommendations.17 Results are expressed as absolute values and percent of predicted.18 DLCO was measured by single breath technique, and the residual volume (RV) and total lung capacity (TLC) were measured in a constant-volume body plethysmograph (Eric Jaeger, Friedberg, Germany). Observed values were compared with Brazilian standards.19,20 All these pulmonary function measurements were executed in Visits 2 and 3 previous to the exercise test (before and 20 min after inhalation of salbutamol, 400 μg via metered-dose inhaler) and immediately afterward. IC measures before and after exercise were done to track DH. Subjects were tested in the seated position wearing a nose clip and asked to breathe regularly for at least 3 tidal maneuvers. They were then urged to take a deep breath, to TLC, without hesitation. At least 3 acceptable maneuvers were performed with variations < 10%, with the highest value stored.17 Lung hyperinflation is present when gas volume in the lungs is increased, compared with the predicted value. The IC is the maximal volume of air that can be inhaled after a spontaneous expiration. In this respect, the smaller the IC in flow-limited patients, the closer the operating tidal volume is to TLC. After exercise, greater reduction in IC usually means higher levels of DH.21
Exercise Tests.
Exercise tests were performed on a treadmill (Inbramed, Inbrasport, Porto Alegre, Brazil), with the subjects being allowed to hold onto the side bars whenever necessary for stabilization purposes. The exercise protocol was planned to have warm-up, incremental, and submaximal phases. The test initiated with a warm-up period of 5 min at a gentle walk (around 1.5 km/h). Thereafter, the speed was increased at a constant rate of 0.5 km/h (incremental phase) until a point where the subject reported a moderate to severe perception of dyspnea assessed by the modified Borg scale (rating shortness of breath between 3–6).22 At this point, the speed was kept constant (submaximal phase) and the subject was instructed to walk until he or she had completed 20 min of total exercise time (including warm-up). Subjects rated their shortness of breath and leg effort each 2 min, and small variations in speed during the submaximal phase were acceptable as long as sensation of dyspnea was maintained around 3–6. If the subject was unable to complete 20 min of exercise due to any reason, he or she was excluded. Heart rate and pulse oximetry were monitored during all exercise time (Nellcor NPB 195, Mallinckrodt, Greenville, Illinois).
Subjects for whom a third visit was indicated were booked 48 hours later. The exercise test for the third visit was at the same speed progression and exercise duration as the test in the second visit.
EPAP.
EPAP was applied with a silicone face mask loaded with a spring linear pressure resistor (Vital Signs USA, Totowa, New Jersey) in a unidirectional expiratory valve (Fig. 2). The device was placed on the subject's face and held in place with straps around the head. At the time of evaluation, the participants first spent some time to get used to the EPAP mask (EPAP desensitization time). Thereafter, the resistor was adjusted to perform a load around 5–10 cm H2O, based on previous studies that used these values and encountered some clinical benefits in COPD patients during exercise.13,14

Silicone face mask loaded with a spring linear pressure resistor in a unidirectional expiratory valve.
Data Analysis
The primary efficacy variable was the variation pre-post exercise in IC with and without the EPAP device. The required sample size (n = 16) was calculated, using the paired t test, in order to detect a difference in IC variation pre-post exercise of 15% (SD 15%) of predicted values comparing tests with and without EPAP. The β and α errors were set at 20% and 5%, respectively. These values were based on previous studies3 and our first 10 pilot patients. Data are described as mean and standard deviation.
Characteristics of subjects with and without DH were compared using the chi-square test with Yates correction for the variables sex, air trapping, and lung hyperinflation, and the Mann-Whitney test or independent samples Student t test for the other variables. Measures with and without EPAP in subjects with DH were compared using the Student t test for paired samples. IC variance under the 2 exercise conditions were determined as IC pre-post exercise values. Once obtained, the mean IC variance with and without EPAP were compared using the paired t test.
The level of significance was set at α = .05. Statistical analyses was with statistics software (SPSS 13.0, SPSS, Chicago, Illinois).
Results
Fifty-one patients with moderate to severe COPD were initially recruited. Five subjects were excluded because they did not tolerate the minimal walking time on the treadmill (20 min), according to our exercise test protocol. Hence, our initial sample was 46 subjects (32 males), with mean age of 65.0 ± 8.2 years and post-bronchodilator values of FEV1, TLC, RV, and DLCO of, respectively, 1.01 ± 0.06 L (38 ± 16% predicted), 7.22 ± 0.20 L (129 ± 19% predicted), 4.89 ± 0.17 L (241 ± 66% predicted), and 10.73 ± 0.74 mL/min/mm Hg (46 ± 17% predicted). From this initial sample, 17 (37%) presented a 15% or greater (0.60 ± 0.35 L) reduction in IC after exercise, filling the predefined criterion to perform Visit 3. A similar absolute mean increase was found in functional residual capacity (FRC) values after exercise in this group (0.69 ± 1.1 L and 36 ± 49%) compatible with constant values of TLC before and after exercise (6.93 ± 1.4 L and 7.09 ± 7.1 L, respectively, P = .45). Baseline characteristics of 17 subjects who overtly developed DH during exercise testing are described in Table 1. The baseline characteristics of these subjects (n = 17) were not different, compared to the remaining subjects (n = 29). After this point, only the data relative to these 17 subjects will be presented.
Baseline Characteristics of 17 Subjects With COPD Who Overtly Developed Hyperinflation and Underwent Exercise Testing
Pulmonary function parameters pre and post-bronchodilator (measured before exercise) showed a significant improvement in FEV1, FVC, peak expiratory flow, RV, RV/TLC, DLCO, IC, and IC/TLC, with similar behavior during Visits 2 and 3 (data not shown).
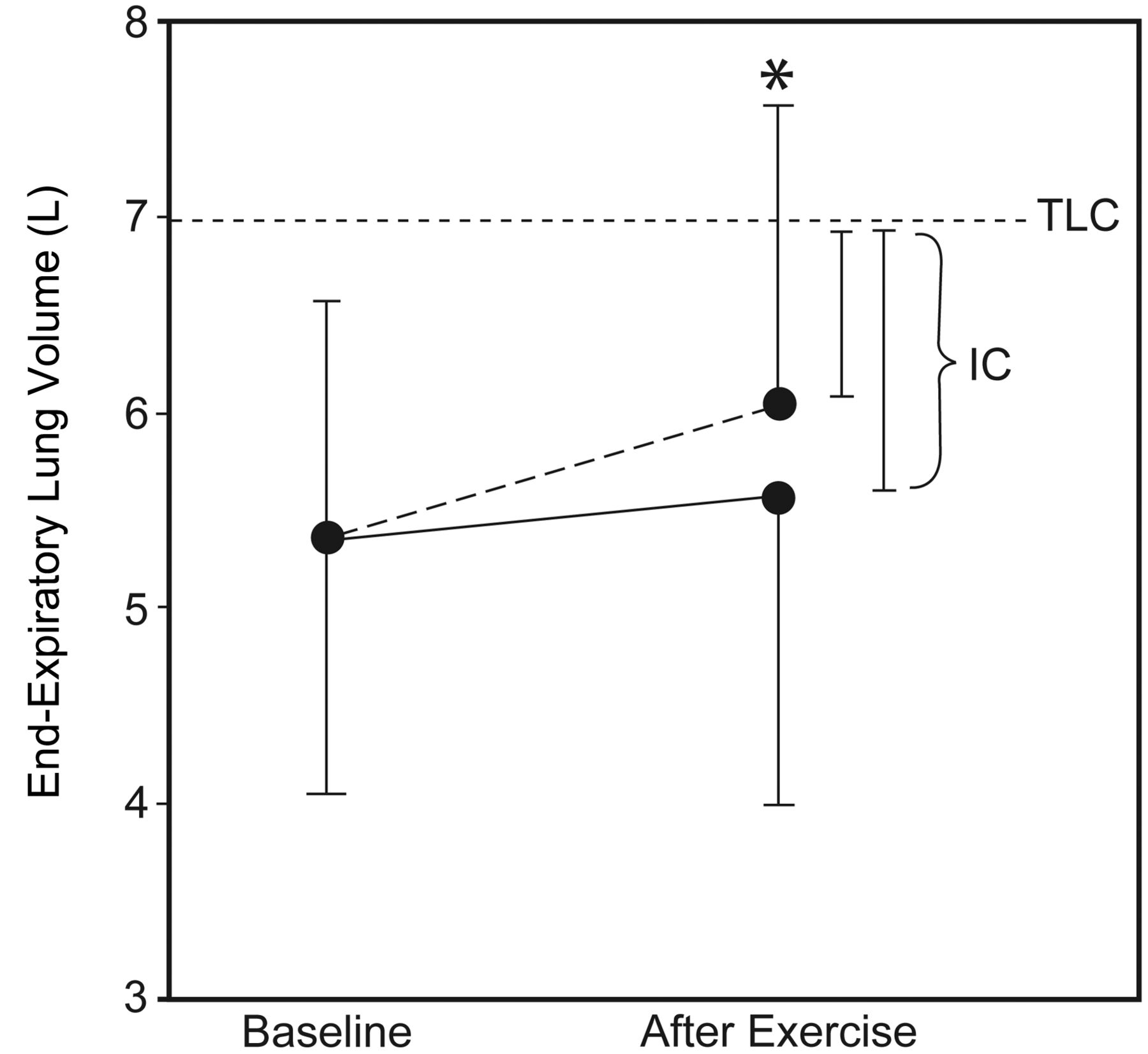
After exercise in Visit 2 (without EPAP) a significant decrease in IC, as expected by the definition adopted to select these subjects, as well as reciprocal FRC increase, were observed. Whereas in Visit 3, when exercise testing was made with EPAP, no significant alterations in FRC, IC, or FRC/TLC occurred (Table 2). Comparing IC variation before and after exercise, significantly less change was observed when EPAP was used (−0.18 ± 0.35 L vs −0.57 ± 0.45 L, P = .02, −6 ± 16% predicted vs −23 ± 16% predicted, P = .01). Similar, but reciprocal, alterations were found when the same analysis was made with FRC (variation pre-post exercise without EPAP 0.69 ± 1.10 L, with EPAP 0.22 ± 0.68 L, P = .02, Fig. 3). In this way, post exercise IC values were different when EPAP was used. They were greater with EPAP (1.45 ± 0.50 L, 55 ± 25% predicted) than without EPAP (1.13 ± 0.52 L, 40 ± 24% predicted, P = .02). No difference regarding pulse oximetry was observed comparing exercise with and without EPAP.
Lung Function Measurements Before and After Exercise With and Without EPAP (n = 17)

End-expiratory lung volume before (baseline) and immediately after exercise with (solid line) and without (dashed line) expiratory positive airway pressure (EPAP) support. Note a significant lower increment in operational lung volumes after exercise with EPAP (n = 17). * P < .05 between the end-expiratory lung volume values (denomination of functional residual capacity during exercise) with and without EPAP after exercise. TLC = total lung capacity. IC = inspiratory capacity.
Discussion
This study demonstrated the beneficial effects of EPAP on operational lung volumes during walking exercise in patients with COPD. The main novel finding of the present study is that the application of EPAP with a simple device (a resistor loaded face mask) was associated with reduced DH, as demonstrated by little change in IC immediately after submaximal exercise, and, consequently, lower end-expiratory lung volume/TLC. As neuromechanical exercise dissociation and dyspnea in these patients are highly correlated with this parameter (r = 0.78 and r = 0.69, respectively, P < .01),4 the hope is that this respiratory support could be used as an auxiliary strategy to improve exercise performance and effort related dyspnea. In fact, a recent study demonstrated a significant increment in IC and marginally prolonged exercise time using a similar EPAP device.23 This study used an exercise protocol in order to evaluate duration of exercise until fatigue (using 30% of 1 maximal repetition alternate knee extension exercise at 70% age-predicted maximal heart rate). Our data, on the other hand, were obtained from a whole body, subjectively determined moderate to intense exercise, in more severe COPD patients (mean FEV1 38% vs 61% predicted).
The mechanism thought to promote this attenuation in exercise DH is reduction of expiratory dynamic airway compression. Application of EPAP may increase bronchial pressure and consequently transmural pressure, leading to a diminution of airway collapse.11 Additionally, EPAP should reduce the inspiratory threshold load on the inspiratory muscles of hyperinflated COPD patients and enhance neuromuscular coupling.9 Unfortunately, the study design was not randomized, and none of the patients performed familiarization for walking on the treadmill. Therefore, improved treadmill walking skills in the second exercise test (Visit 3, with EPAP) could partially or completely explain our findings.
Effects of EPAP on COPD
Several studies have evaluated NIV to improve exercise in COPD patients.8,24–26 A few studies, however, have used NIV without additional inspiratory support (ie, CPAP only), thus potentially compromising the interpretation of results. Furthermore, their primary objective was not the evaluation of the effect on physiological variables that may detect DH,11,13–15 except one study on which we previously commented.23 Nevertheless, 2 studies reported the effects of CPAP on operational lung volumes during exercise in COPD, and there was no change in end-expiratory lung volume with the addition of CPAP.13,14
The physiological rationale for EPAP utilization in COPD patients is explained by potential improvement in ventilation-perfusion ratio,27 change in breathing pattern,28,29 reduction of expiratory flow limitation,30 and improved length/tension relation of the respiratory muscles.31 These EPAP benefits are believed to be achieved by avoiding or reducing expiratory airway collapse that usually occurs in COPD patients, resulting in more homogenous ventilation and lower waste in dead space. Previous studies that used positive expiratory pressure in patients with severe airway obstruction actually demonstrated a decrease in minute ventilation, tidal volume, breathing frequency, and physiologic dead-space ventilation at rest27 and during exercise.11 This improvement in ventilatory efficiency for a given level of external work may delay the development of DH, which plays a pivotal role in COPD exercise intolerance. On the other hand, EPAP can simply reduce airway collapse, prolonging expiratory time, and thereby reducing lung volumes.
The fact is that we observed a reduction in the rate of development in DH, as observed by lower operational lung volumes (see Fig. 3) with EPAP, but, as cardio-respiratory parameters during exercise tests were not assessed, the exact physiological mechanism cannot be determined.
In our study, we chose to use an EPAP face mask because of its lower cost, which facilitates its use in pulmonary rehabilitation centers. Values close to 10 cm H2O are recommended to obtain satisfactory results, but it is important to respect the patient's capacity to overcome the forced expiratory load.32 We chose EPAP values close to 10 cm H2O, but if the patients were not able to overcome the resistance imposed, the value was reduced gradually to as low as 5 cm H2O.
Increments in resting and dynamic IC have been shown to correlate well with improved peak oxygen consumption, constant work endurance time, and reduced exercise dyspnea intensity,33,34 and EPAP may decrease inspiratory muscle effort during exercise, through inspiratory threshold reduction.34 On the other hand, this modality of NIV might increase expiratory muscle effort in some individuals,34 resulting in greater dyspnea sensation.11 So the lesser degree of DH observed with EPAP has the potential to result in greater exercise endurance, with reduced dyspnea perception, whereas an increased resistant work and, consequently, expiratory effort could counterbalance this beneficial effect. Therefore, the real clinical benefit of EPAP during exercise remains to be determined.
Methodological Considerations
The major limitation of the present study is that we did not evaluate the potential clinical benefits of the experimental intervention. Actually, we adopted a simple and straightforward exercise test protocol, obviating a previous incremental exercise test. This was accomplished by anchoring the exercise intensity to a breathlessness symptom score (Borg scale 3–6), previously suggested to effectively estimate exercise intensity,35,36 and currently accepted to determine intensity for exercise prescription.37 This strategy seemed to be effective, since development of DH was observed. In future studies, we speculate that the level of work intensity could be identified in the first 5–10 min (rating shortness of breath in a greater level of intensity, around 5–7 on the Borg scale) and ask the patient to walk thereafter as long as possible. In this manner, the exercise endurance and peak dyspnea could be assessed.
Second, the intervention and control exercise test were not randomized or blinded. Furthermore, familiarization with walking on a treadmill requires practice and skill. Therefore, the practice (familiarization) with the exercise protocol test in Visit 3 may have influenced our results.
Third, the evaluation of EPAP effectiveness was done only in COPD subjects who overtly developed DH after exercise (IC decrease > 15%); maybe this would not be so efficient in subjects with lower levels of DH. A possible explanation for the small number of subjects with DH is the fact that we did not evaluate serial IC measures during exercise, but only immediately after. Studies that measured DH during cardiopulmonary exercise tests found a reduction in IC during exercise as the ventilatory demand increased.2,4,38,39 Another reason for the lower DH rate may be the use of bronchodilator, which was offered to all participants before the exercise, because we were interested in evaluating the effects of EPAP over DH in COPD patients with their best possible condition. Additionally, our findings, therefore, could not be generalized for COPD patients without recent use of bronchodilator, since the use of bronchodilator immediately before an exercise test interferes with the degree of DH developed during the test.40 The last methodological issue is that following exercise we assessed the accuracy of lung volumes measured by whole body plethysmography, wherein the breathing pattern could interfere with the maneuvers. As shown, this appeared not to jeopardize plethysmographic determinations of lung volumes, since FRC and IC changes were exactly reciprocal. Considering that the majority of patients with moderate to severe COPD do not develop contractile fatigue of the diaphragm after high-intensity exercise to the limit of tolerance (affecting IC measurements),41 this finding is consistent with the concept that TLC remains constant during exercise.42
Conclusions
The use of EPAP during submaximal exercise seems to promote significant reduction in the development of DH in COPD patients (post exercise IC values with and without EPAP, respectively, 1.45 ± 0.50 L vs 1.13 ± 0.52 L, P = .02). Whether this physiological benefit will be translated into real clinical advantages remains to be answered. Moreover, lung volumes determination by whole body plethysmography performed immediately after exercise seems to be accurate and supportive of the concept that TLC does not change with exercise.
Acknowledgments
The authors would like to thank all the colleagues who helped with laboratory technical support, as well as all the subjects for their effort and enthusiastic cooperation throughout the study.
Footnotes
- Correspondence: Mariane Borba Monteiro PT DSc, Department of Physiotherapy, Centro Universitário Metodista do Instituto Porto Alegre, Rua Coronel Joaquim Pedro Salgado, 80 Rio Branco, CEP 90420–060, Porto Alegre, Rio Grande do Sul, Brazil. E-mail: marianemonteiro{at}hotmail.com.
This research had financial support to perform lung function tests from the Incentive Fund Research of Hospital de Clínicas de Porto Alegre, Porto Alegre, Brazil.
Dr Zimermann Teixeira presented a version of this paper at the meeting of European Respiratory Society, held September 18–22, 2010, in Barcelona, Spain.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 1530
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}