

Abstract
BACKGROUND: Patients undergoing pulmonary lobectomy carry a high risk of respiratory complications after surgery. The postoperative prophylactic treatment with helmet CPAP may prevent postoperative acute respiratory failure and improve the PaO2/FIO2.
METHODS: We randomly allocated 50 subjects to receive continuous oxygen therapy (air-entrainment mask, FIO2 0.4) or 2 cycles of helmet CPAP for 120 min, alternating with analog oxygen therapy for 4 hours. Blood gas values were collected at admission to ICU, after 1, 3, 7, 9, 24 hours, and then in the thoracic ward after 48 hours and one week after surgery. We investigated the incidence of postoperative complications, mortality, and length of hospital stay.
RESULTS: At the end of the second helmet CPAP treatment, the subjects had a significantly higher PaO2/FIO2, compared with the control group (366 ± 106 mm Hg vs 259 ± 60 mm Hg, P = .004), but the improvement in oxygenation did not continue beyond 24 hours. The postoperative preventive helmet CPAP treatment was associated with a significantly shorter hospital stay, in comparison to standard treatment (7 ± 4 d and 8 ± 13 d, respectively, P = .042). The number of minor or major postoperative complications was similar between the 2 groups. No difference in ICU readmission or mortality was observed.
CONCLUSIONS: The prophylactic use of helmet CPAP improved the PaO2/FIO2, but the oxygenation benefit was not lasting. In our study, helmet CPAP was a secure and well tolerated method in subjects who underwent pulmonary lobectomy. It might be safely applied whenever necessary.
- CPAP ventilation
- pulmonary surgical procedures
- respiratory insufficiency
- postoperative care
- pulmonary atelectasis
Introduction
Despite a more accurate preoperative patient assessment, utilization of modern anesthesiological and surgical techniques, and a wider use of postoperative monitoring, mortality after lung resection is still considerable, ranging from 2% to 11%, while pulmonary postoperative complications can reach an incidence of 15–18%.1–4 Acute respiratory failure after lung surgery is fatal in up to 40% to more than 60%.2 This high mortality is also related to postoperative reintubation and mechanical ventilation, which occurs in about 5% of patients.2 After thoracic surgery the loss of functional parenchyma, prolonged supine position, postoperative pain, reduction of diaphragmatic movement, and a possible lesion of the phrenic nerve work together to generate atelectasis and decreased residual functional capacity. In these patients, CPAP should improve the gas exchange and arterial oxygenation by opening previously closed lung units; on the other hand, applying continuous positive pressure on the airways theoretically might increase pulmonary air leaks and incidence of bronchopleural fistula.5
The effectiveness of CPAP and noninvasive ventilation (NIV) in the postoperative period with a prophylactic or therapeutic purpose has been investigated in different types of surgeries since the 1980s.6–12 In lung surgery there are only 3 prospective randomized trials.13–15
Auriant et al13 studied 48 patients with acute postoperative respiratory insufficiency after lung surgery. They observed that NIV treatment reduces the need for reintubation (50% in the no-NIV group vs 21% in the NIV group, P = .035) and overall mortality (37.5% vs 12.5%, P = .045).
Two studies evaluated the prophylactic use of CPAP or NIV. In the first study of Aguiló et al,14 prophylactic nasal bi-level positive airway pressure (BPAP), applied for one hour after extubation, improved oxygenation; however, only short-term data were recorded, and it is unclear whether the alveolar recruitment was kept after BPAP suspension. In the second prospective randomized trial, Perrin et al15 studied the prophylactic use of NIV administered preoperatively and postoperatively in patients who had a preoperative FEV1 < 70% of predicted value. In the BPAP group, postoperative PaO2 significantly improved during the stay (P = .04), and the incidence of atelectasis (P = .04) was significantly reduced.
We conducted this prospective randomized controlled study to evaluate the effectiveness of the prophylactic application of CPAP delivered by helmet after pulmonary lobectomy to improve oxygenation (PaO2/FIO2). We also investigated the incidence of postoperative pulmonary complications, with particular focus on air leaks, length of hospital stay, and mortality.
QUICK LOOK
Current knowledge
Pulmonary lobectomy is associated with a high risk of postoperative pulmonary complications, including atelectasis and pneumonia.
What this paper contributes to our knowledge
Postoperative application of CPAP by a helmet interface transiently improves oxygenation following lobectomy. This improvement is observed only during CPAP therapy.
Methods
This study was approved by the medical ethics committee of the University of Parma and was conducted in accordance with the principles outlined in the Declaration of Helsinki. Any patient prospectively scheduled for elective lung resection from March 2007 to December 2008 was eligible for the study.
Exclusion criteria were severe respiratory failure (respiratory frequency ≥ 25 breaths/min, PaO2 ≤ 60 mm Hg, PaCO2 ≥ 55 mm Hg, PaO2/FIO2 ≤ 200 mm Hg with FIO2 ≥ 0.6), inability to defend the airways, facial trauma, claustrophobia, neurological or psychiatric disorders, anxiety, any events contraindicating early patient extubation, and failure in placing an epidural or paravertebral catheter. Patients who had recently undergone gastroesophageal surgery were also excluded, as well as patients suffering from severe cardiac disease.
On the day before surgery all subjects were fully informed about the nature, characteristics, purposes, and potential risks of the study. Written informed consent was obtained from all of them.
Before anesthesia induction, a thoracic epidural or paravertebral catheter was placed to achieve good pain control in the intraoperative and postoperative period. After induction of general anesthesia a double-lumen tube was placed and one-lung ventilation was performed. All subjects underwent lung lobectomy for non-small-cell lung cancer, through a postero-lateral thoracotomy approach. Before chest wall closure, two 24 French chest tubes were placed and connected to a suction chamber drainage system (Pleur-evac, Teleflex Medical, Kenosha, Wisconsin). After extubation, a negative pressure of −20 cm H2O was applied on the chest tubes, but discontinued during CPAP delivery. The chest tubes were removed 24 hours after cessation of air leaks and/or fluid drainage < 250 mL/24 hours. At the end of surgery all subjects were extubated in the operating room and transferred to the ICU breathing spontaneously with oxygen supply (air-entrainment mask, FIO2 0.4). Postoperative analgesia was achieved using acetaminophen, 1 g every 6 hours, intravenously, and continuous infusion of 0.2% ropivacaine via the peridural or paravertebral catheter.
All subjects were monitored, intraoperatively and postoperatively, using an arterial catheter, a central venous catheter, continuous pulse oximetry, continuous electrocardiogram recording, and hourly urine flow.
After ICU admission, subjects underwent computerized randomization. The CPAP group received 2 CPAP cycles of 2 hours delivered by helmet (4-Vent, Rüsch, Mirandola, Italy). Setting parameters were: FIO2 0.4, PEEP 8 cm H2O, flow 45 L/min. PEEP was obtained by connecting the helmet's gas in-flow line with a high flow gas source (passing through a high compliance reservoir). On the helmet's out-flow line we placed a standard PEEP valve. After every cycle, subjects were treated with oxygen support delivered by an air-entrainment mask (FIO2 0.4). The control group received continuous oxygen therapy over an air-entrainment mask (FIO2 0.4). Blood gas values were collected at admission to ICU and after 1 hour, immediately before the first helmet CPAP treatment, immediately after the first helmet CPAP treatment, immediately before and after the second helmet CPAP treatment, then at 24 and 48 hours after surgery, always with subjects on oxygen therapy. At one week after surgery a sample was collected with subjects without oxygen therapy.
Standard therapy for all subjects included short-term antibiotic prophylaxis with ampicillin-sulbactam, aerosol therapy with salbutamol and beclomethasone 3 times a day, deep vein thrombosis prophylaxis with low-molecular-weight heparin, rapid mobilization and chest physiotherapy performed by a certified physiotherapist once daily starting from the first postoperative day. Every subject underwent scheduled chest x-ray every day during the first 2 postoperative days and the day after removal of chest tubes.
Pulmonary complications were classified as minor or major complications. Minor complications included sub-lobar lung atelectasis or uncomplicated sputum retention. We defined sputum retention as the presence of rales at pulmonary clinical exam in the absence of effective cough: it was considered as complicated when associated with hypoxemia and/or atelectasis, uncomplicated when normal gas exchange was maintained. Major complications included lobar lung atelectasis, complicated sputum retention, pneumonia defined according to the Center for Disease Control and Prevention criteria, pulmonary embolism, and ALI/ARDS.
In the case of lobar lung atelectasis or complicated sputum retention, subjects underwent fiberoptic bronchoscopy; if symptoms persisted 24 hours after bronchoscopy, a percutaneous crico-laryngeal mini-tracheostomy was placed in order to allow for a more effective secretion clearing, and an empiric wide spectrum antibiotic therapy was started.
We also investigated the presence of air leaks, defined by the presence of air bubbles in the water-seal chamber following the subject's forced expiration; they were defined as persistent air leaks if lasting more than one week after surgery.
In the absence of major postoperative complications, subjects were discharged from the ICU 18–24 hours after surgery and transferred to the thoracic surgery ward. The outcome assessment included documentation of overall morbidity and mortality, length of hospital stay, postoperative pulmonary complications, pulmonary air leaks, CO2 retention, and any case of CPAP interruption.
Power Calculation
The hypothesis zero of the study was that preventive CPAP after major thoracic surgery improves respiratory function and as a consequence the PaO2/FIO2. We considered as clinically important an increase in the PaO2/FIO2 of 50 mm Hg, with an expected standard deviation of 60 mm Hg. To detect this difference between the treatment and the control group, accepting a 2-tailed α error of 5%, and a β error of 20% or less, 22 subjects were studied in every group.16 To manage a drop-out rate of 10–15% a total of 52 subjects were studied.
Statistical Analysis
Statistical analysis was performed with statistics software (SPSS 15.0, SPSS, Chicago, Illinois). The analysis included only subjects who fulfilled the study protocol in terms of eligibility, interventions, and outcome assessment (“per-protocol” analysis). All subjects included in the analysis were followed until discharge from the hospital. The data of subjects who withdrew from or discontinued therapy were not included (one in each study group).
Normal distribution of the collected data were first evaluated using the Kolmogorov-Smirnov test. Continuous variables were analyzed using the analysis of variance. To control the effect of potentially confusing variables, analysis of covariance was used. Mixed between-within subject analysis of variance was used for repeated continuous variables to determine a difference between the groups and within each group during the study protocol. If the data were not normally distributed, the non-parametric Mann-Whitney test and Friedman test were used. Nominal data were analyzed by chi-square analysis with the Yates continuity correction or the Fisher exact test, as appropriate. A Wilcoxon rank-sum test to compare the length of stay between the 2 groups was used to assess the effect of treatment on the length of hospital stay. Continuous variables are presented as mean ± SD, 95% CI, or median (range), according to data distribution. Categorical data are presented as number and percent. P values < .05 were considered significant. Bonferroni correction was applied for multiple comparisons.
Results
Fifty-two subjects undergoing elective lung lobectomy were enrolled in the study. A flow chart in agreement with the CONSORT statement17 recording the recruitment process and progression of the trial is shown in Figure 1.

CONSORT flow diagram of progress through stages of the randomized trial.
The subject characteristics, comorbidities, preoperative respiratory function, and duration and type of intervention are shown in the Table. No significant differences were detected in the variables between the 2 groups except for the distribution of sex (P = .01).
Anthropometric, Lung Function, and Surgical Data
Nine hours after surgery, immediately after the second cycle of CPAP, the treatment group had a significantly better PaO2/FIO2, compared with the control group (P = .004): the mean values were 366 ± 106 mm Hg and 259 ± 60 mm Hg, respectively (Fig. 2). After the CPAP cycles were stopped, this improvement was lost and the PaO2/FIO2 was analogous in both groups after 24 hours, 48 hours, and one week.

Course of PaO2/FIO2 during 7 days. The error bars represent the 95% CIs.
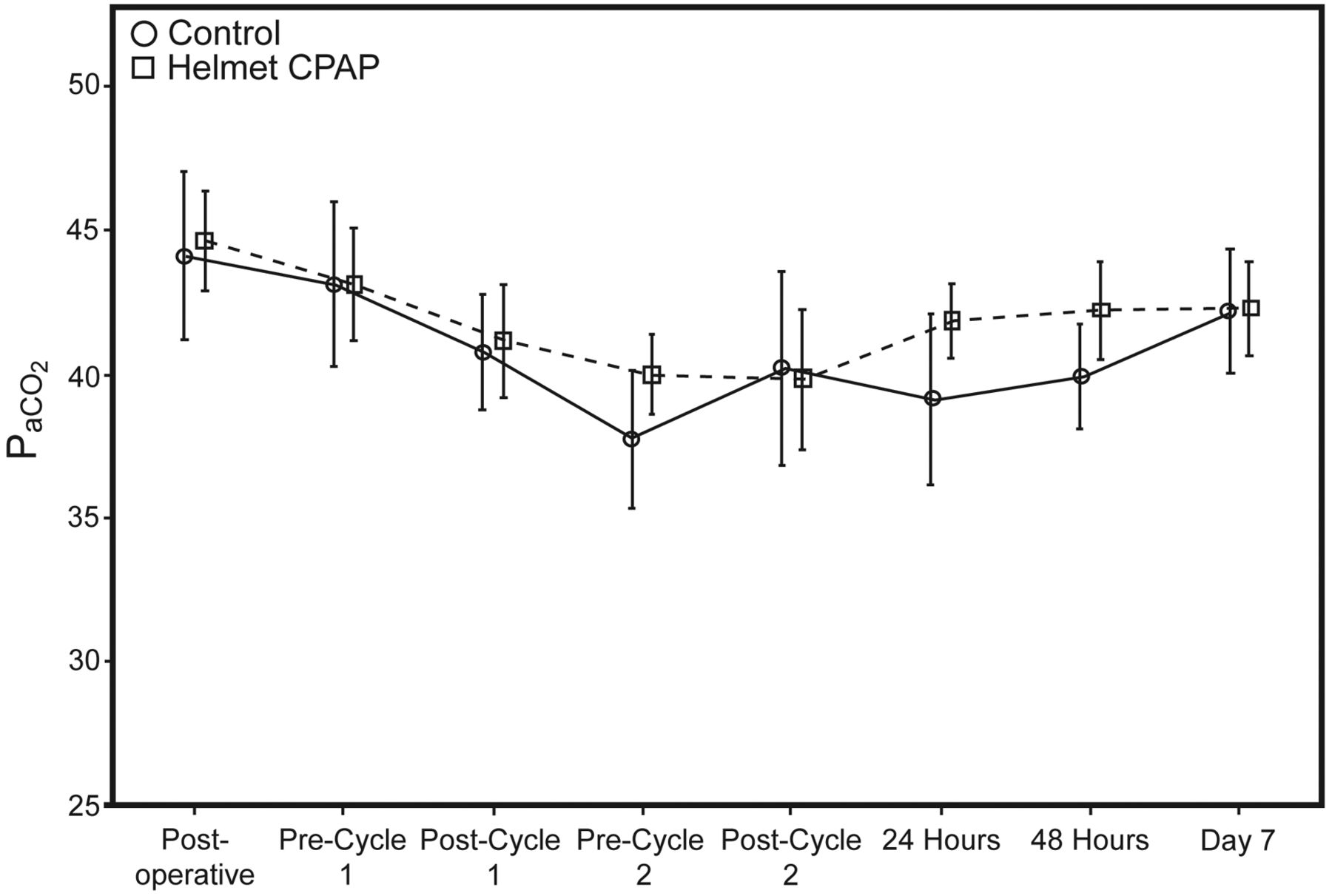
The course of the PaCO2 values in both groups is shown in Figure 3. During the whole observation time there was no difference in PaCO2, and application of helmet CPAP did not result in increased PaCO2 levels.

Course of PaCO2 values during 7 days. The error bars represent the 95% CIs.
Eleven subjects (22%) experienced postoperative respiratory complications: 7 subjects in the helmet CPAP group had minor complications, compared with 4 in the control group (P = .25). Major complications were similar in both groups: 3 subjects in the helmet CPAP group versus 4 subjects in the control group. In particular, 3 subjects in the control group developed pneumonia, but none in the helmet CPAP group (P = .24). No subject in either group needed to be reintubated.
Three (12%) subjects of the helmet CPAP group and one of the control group needed a bronchoscopic toilette due to sputum retention (P = .61). In 2 subjects of the helmet CPAP group, but none in the control group, a percutaneous crico-pharyngeal mini-tracheostomy was placed, which remained for 2 and 3 days, respectively. The difference between the 2 groups did not reach statistical significance (P = .49).
In the control group 18 subjects did not develop air leaks, 6 presented moderate air leaks spontaneously resolving within 7 days, and only one subject had lasting air leak over 10 days. In the CPAP group 21 subjects did not develop air leaks, 4 had air leaks resolving within 5 days, and no subject had persistent air leaks. Thus, the incidence of air leak 24 and 48 hours after the operation was higher in the control group than in the helmet CPAP group, although the difference was not statistically significant (P = .49). None of the subjects in either group developed bronchopleural fistula. Subjects of both groups had an ICU stay between 18 and 24 hours without any readmission.
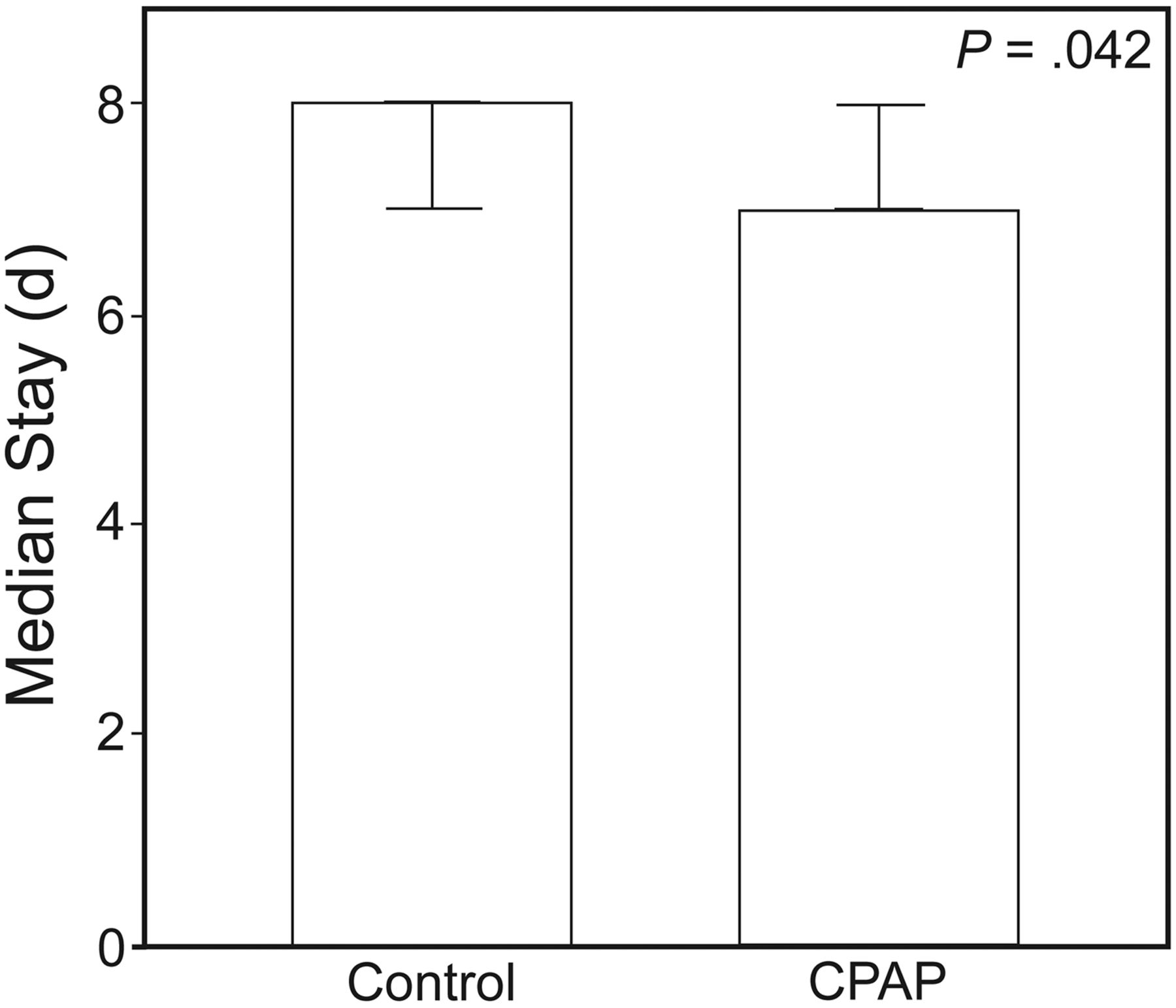
Subject outcome was validated by 2 variables: length of hospital stay, and mortality. Subjects in the helmet CPAP group had a median hospital stay of 7 days (range 6–10 d), compared to 8 days (range 7–21 d) for the subjects in the control group. As shown in Figure 4 the length of hospital stay was statistically shorter in the helmet CPAP group than in the other group (P = .042). One subject in the helmet CPAP group died on the 10th postoperative day (overall mortality of 2%); this difference between the groups was not statistically significant.

Median hospital stay. The error bars represent the 95% CIs.
Discussion
This study aimed to evaluate for the first time the prophylactic use of helmet CPAP after lung lobectomy. It was able to show that the prophylactic use of helmet CPAP can progressively improve the PaO2/FIO2, reaching a statistically significant higher value at the end of the second round of CPAP, compared to the control group. However, the improvement in terms of oxygenation was not lasting, and after conclusion of the treatment the values turned out to be similar to those in the control group after 24 hours, 48 hours, and one week after surgery.
Applying a prophylactic and not therapeutic treatment, we effected only 2 cycles lasting 2 hours in the first 12 hours postoperatively. In lung surgery, Aguilò14 examined the postoperative prophylactic use of nasal BPAP during only one hour after extubation and found a better oxygenation immediately after the conclusion of NIV. Perrin et al15 randomized 32 patients (14 in the study group vs 18 in the control group) candidates for lobectomy, who had a preoperative FEV1 < 70% of a predicted value, to use facial BPAP from one week before until 3 days after surgery. On days 1, 2, and 3, PaO2 was significantly improved in the NIV group. In this study all patients had a high risk of postoperative respiratory complications (eg, hypoxia).
Considering that we could not compare our experience to similar experiences in thoracic surgery, we evaluated clinical studies that analyzed the prophylactic use of NIV in patients undergoing other types of surgery, applying longer rounds in the first 24 hours postoperatively.6,11,12 Conflicting results have been obtained. For example, Squadrone et al9 studied, in a randomized multicenter trial, the preventive application of helmet CPAP in 209 subjects undergoing major abdominal surgery. All subjects were given helmet CPAP over 6 hours, followed by a 1-hour period in which they were supported only by an air-entrainment mask (FIO2 0.3). In those subjects who developed a PaO2/FIO2 < 300 mm Hg in the 1-hour period, CPAP treatment was replicated. In this trial the helmet CPAP group had a lower intubation rate (P = .005) and a lower occurrence of pneumonia (P = .02), infection (P = .03), and sepsis (P = .03). In our study, after the second cycle of helmet CPAP all subjects had a PaO2/FIO2 > 300 mm Hg, although the duration of CPAP was shorter and oxygen therapy was delivered to the subject every 4 hours. However, arterial blood gas analysis was done at the end of the helmet CPAP cycle. Kindgen-Milles and colleagues,11 who studied the prophylactic use of nasal CPAP after thoracic-abdominal vascular surgery concomitant with thoracotomy, but not affecting the pulmonary parenchyma, applied the CPAP for a consecutive 12–24 hours without interruptions; nevertheless, 4 hours after conclusion of the treatment the PaO2/FIO2 was inferior to the starting values immediately after extubation and equivalent to the parameters in the control group. Only Joris et al,12 who studied BPAP application during 24 hours after gastroplasty for bariatric surgery, found an instantaneous and lasting improvement in the respiratory function. Differently from our study, they selected a group of patients without thoracotomy and pulmonary resection. The use of BPAP and not CPAP seems not to be relevant, as no advantage of one method has been shown so far.7,9–13,15
Although the sample size has not been calculated to verify this issue, our study did not show significant differences in terms of minor or major complications between the 2 groups. None of the subjects had a PaO2/FIO2 < 100 mm Hg, or needed to be reintubated or readmitted to the ICU. The percentage of pulmonary infections was different between the 2 groups (0 in the treatment group, compared with 3 in the control group), but did not reach statistical difference.
Some researchers are skeptical about the early use of CPAP or NIV after thoracic surgery, because of its theoretical risk of favoring air leaks and bronchopleural fistula.5 In our study we saw no difference between the 2 groups; there was even a slightly higher number of air leaks in the control group. Also Aguilò et al did not find a higher risk for air leaks.14 In the case of gastric and/or esophageal surgery, NIV has been considered as relatively contraindicated because of the possible risk of anastomotic dehiscence; however, it has been shown that it can be safely used if a pressure of 12 cm H2O is not exceeded.7 In our study the prophylactic use of helmet CPAP had no influence on the mortality rate, although the small number of subjects did not allow for a definite assessment of mortality.
Concerning tolerability, only one subject temporarily stopped the treatment with helmet CPAP because of a claustrophobic attack. The choice of the helmet interface was guided by a better acceptance, as compared to oronasal mask,18–20 although the use of the helmet can be correlated to an increase in PaCO2 because of rebreathing of expired CO2.21,22 To minimize this risk a high flow of fresh gas has been proposed by Patroniti et al.23 In our study the air/oxygen mixture was applied with a flow of 45 L/min, and the PaCO2 values in the treatment group were always comparable to those in the control group. These data confirm that the use of a medium-high flow prevents this complication.
In contrast to most of the studies mentioned, we investigated an unselected, non-hypoxemic population. Nevertheless, in favor of the preventive CPAP treatment, we found shorter hospital stay in the treatment group: a result also reported by Perrin,15 Kindgen-Milles,11 and Squadrone.9 Four subjects in the control group had a hospital stay longer than 10 days: 3 of them developed a respiratory complication (pneumonia), and one suffered from a wound infection. Certainly, a further large randomized trial might help to elucidate whether CPAP is able to reduce hospital stay after lung resection also in non-hypoxemic patients and if it should be added to the standard therapy.
Conclusions
In conclusion, the prophylactic use of helmet CPAP after pulmonary lobectomy temporarily improved blood oxygenation, but this effect was not sustained. The method was well tolerated by the subjects after lobectomy. This study supports the rationale as to why helmet CPAP can be used as a safe and well tolerated method in situations such as hypoxemic, non-hypercapnic postoperative respiratory insufficiency.
Footnotes
- Correspondence: Stefanie Ziegler MD PhD, Department of Anesthesia, Intensive Care, and Pain Therapy, University Hospital of Parma, Via Gramsci 14, 43100 Parma 43100, Italy. E-mail: zieglerstefanie{at}gmail.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}