

Abstract
BACKGROUND: Low-tidal-volume ventilation may be associated with repetitive opening and closing of terminal airways. The use of PEEP is intended to keep the alveoli open. No method of adjusting the optimal PEEP has shown to be superior or to improve clinical outcomes. We conducted a pilot study to evaluate the effect of setting an individualized level of PEEP at the highest compliance on oxygenation, multiple-organ-dysfunction, and survival in subjects with ARDS.
METHODS: Subjects with ARDS ventilated with low tidal volumes and limitation of airway pressure to 30 cm H2O were randomized to either a compliance-guided PEEP group or an FIO2-guided group.
RESULTS: Of the 159 patients with ARDS admitted during the study period, 70 met the inclusion criteria. Subjects in the compliance-guided group showed nonsignificant improvements in PaO2/FIO2 during the first 14 days, and in 28-day mortality (20.6% vs. 38.9%, P = .12). Multiple-organ-dysfunction-free days (median 6 vs 20.5 d, P = .02), respiratory-failure-free days (median 7.5 vs 14.5 d, P = .03), and hemodynamic-failure-free days (median 16 vs 22 d, P = .04) at 28 days were significantly lower in subjects with compliance-guided setting of PEEP.
CONCLUSIONS: In ARDS subjects, protective mechanical ventilation with PEEP application according to the highest compliance was associated with less organ dysfunction and a strong nonsignificant trend toward lower mortality. ClinicalTrials.gov Number NCT01119872.
Introduction
ARDS is characterized by the acute onset of hypoxemia and bilateral infiltrates that are consistent with pulmonary edema, without evidence of left heart failure.1 Mechanical ventilation is potentially lifesaving in patients with ARDS, but may cause ventilator-associated lung injury. Lung-protective ventilation strategies seek to prevent ventilator-associated lung injury by using low tidal volume (VT) to avoid overdistention, and PEEP to prevent repetitive alveolar collapse and reopening.2–4
The application of PEEP improves gas exchange and lung function. The main effect of increasing PEEP is to maintain the recruitment of alveolar units that were previously collapsed. Thus, since the VT is distributed to more alveoli, peak airway pressure is reduced and compliance is increased.5 However, the pressure needed to open and recruit some alveoli may overdistend others, which may direct blood perfusion away from these areas, thereby increasing dead space, pulmonary vascular resistance, and mean hydrostatic pressure, and thus increase lung damage.6 The preferred method of adjusting the PEEP is still controversial.7,8 The amount of potentially recruitable lung tissue has best been evaluated using computed tomography,9 but this approach is usually not readily available in ICUs for routine assessment of ventilator settings.
Some have suggested that lung mechanics are a better surrogate than gas exchange for bedside assessment of lung recruitment,10 and that the PEEP should be chosen individually.10–12 In fact, several studies have shown improved survival when PEEP is set above the lower inflection point on the pressure-volume curve, the steepest portion of the curve, a sign of increase of functional residual capacity.12–15 Unfortunately, all these studies also compared low versus high VT ventilation, which hinders evaluation of the effect directly attributable to PEEP. Recently, 2 studies compared different methods of PEEP setting. One study, based on individual maximum alveolar recruitment, failed to demonstrate a reduction in mortality, although they observed significant improvements in oxygenation16 and lung function.17
We conducted an open, randomized controlled pilot study to test the hypothesis that individualized PEEP set based on highest compliance would improve oxygenation, compared to setting PEEP based on FIO2.18
QUICK LOOK
Current knowledge
Lung-protective ventilation (low tidal volume and limited plateau pressure) improves outcomes in ARDS, but the best method of selecting the PEEP is controversial, and clinical trials have had conflicting results.
What this paper contributes to our knowledge
In ARDS patients, low-tidal-volume ventilation coupled with PEEP set according to the highest pulmonary compliance was associated with more organ-dysfunction-free days and a trend toward lower mortality.
Methods
This study was conducted in a 14-bed mixed medical-surgical ICU in Spain, over a time period of 60 months. The study protocol was approved by our institution's Ethics and Clinical Trials Committee, and registered at http://clinicaltrials.gov (NCT01119872). Written informed consent was required for inclusion, and obtained from the nearest relatives. No commercial entities had any role in any aspect of this study.
We screened all patients with ARDS according to the American-European consensus conference definition,1 who maintained ARDS criteria after 24 hours of mechanical ventilation, in order to confirm ARDS and exclude other causes of hypoxemia and pulmonary infiltrates, since mechanical ventilation parameters can affect oxygenation and whether the patient meets the ARDS definition.19 We excluded patients who were younger than 18 years, pregnant, or had neuromuscular disease, intracranial hypertension, head trauma, left ventricular dysfunction (on echocardiography), > 72 hours of mechanical ventilation, or barotrauma. Patients with end-stage conditions (death expected within 90 days) were also excluded. We defined barotrauma as the presence of air outside the tracheobronchial tree, resulting from presumed alveolar rupture, and manifested as interstitial emphysema, pneumothorax, pneumomediastinum, pneumoperitoneum, or subcutaneous emphysema.20 Patients who developed barotrauma during the first 24 hours of observation prior to randomization were also excluded, because it was not feasible to measure plateau pressure. In subjects excluded after randomization, the respiratory protocol was not applied, although protective lung ventilation was maintained, and they were kept in their assigned study groups for outcome analysis.
Study Design
All patients who met ARDS criteria were ventilated during 24 hours with low VT (6–8 mL/kg predicted body weight [PBW]), an inspiratory plateau pressure < 30 cm H2O, a breathing frequency of 30 breaths/min, adjusted to maintain a pH between 7.30 and 7.45, and limited to a maximum of 35 breaths/min, FIO2 that kept arterial oxygen saturation at 88–95% or PaO2 at 55–80 mm Hg, and PEEP adjusted to achieve the best oxygenation with the lowest FIO2 while avoiding adverse hemodynamic effects. If the plateau pressure was > 30 cm H2O with a VT of 6 mL/kg PBW, a stepwise VT reduction of 1 mL/kg PBW to as low as 4 mL/kg/PBW was allowed, in which case the plateau pressure limit was set at 35 cm H2O.
After 24 hours, subjects who met the inclusion criteria were randomized to either FIO2-guided PEEP (control group) or compliance-guided PEEP. Randomization was performed in blocks of 10, using sealed envelopes.
In the control group, PEEP was set based on the subject's FIO2, as applied in the ARDS Network study.18 In the compliance-guided group, PEEP was set daily, according to the method described by Suter et al.12 Static compliance was measured at increasing levels of PEEP and at constant PEEP. Static compliance was calculated as VT divided by the pressure difference at end of inflation hold (2 s), and PEEP was increased in steps of 2 cm H2O, beginning at 5 cm H2O, without an upper PEEP titration limit. The highest static compliance was considered to be the best PEEP. If at 2 different PEEPs the static compliance was identical, we chose the one with the lower plateau pressure (see the respiratory protocol in the supplementary materials at http://www.rcjournal.com). All subjects received sedatives and opioids at the time of PEEP setting. Neuromuscular blocking agents were used as required for low-VT ventilation, although not for the measurement of intrinsic PEEP or plateau pressure.
According to the study group, PEEP was adjusted once daily during the morning shift, until the weaning phase started. Intrinsic PEEP was measured before and after every change of applied PEEP, and the inspiratory/expiratory ratio was changed accordingly to prevent intrinsic PEEP.
All other ventilator parameters were set in the same way in both study groups, following the protocol applied for 24 hours before randomization.18
The weaning protocol was identical for both groups. Weaning was begun if the cause of respiratory failure had resolved, PaO2 was > 60 mm Hg, FIO2 was ≤ 0.4, and PEEP was below 6 cm H2O. In the compliance-guided group, PEEP was lowered by steps of 2 cm H2O. In the control group we applied the protocol described in the ARDS Network study18 (see the supplementary materials at http://www.rcjournal.com).
Subjects were monitored with a pulmonary artery catheter for at least the first 72 hours after randomization, to study the hemodynamic effects of PEEP. Therapy other than mechanical ventilation was prescribed at the discretion of the attending physicians not involved in the study. Our local protocols were applied to guide sedation, hemodynamic support, and other standard interventions.
End points were assessed at 28 days. The primary end point was PaO2/FIO2. Secondary end points were mortality, ventilator-free days, ICU and hospital stay, multiple-organ-dysfunction (MOD) free days, and respiratory and hemodynamic parameters.
Measurements
Data collected from each subject included demographics, risk factors for ARDS, routine laboratory measurements, Acute Physiology and Chronic Health Evaluation II score21 at ICU admission, daily Lung Injury Score,22 Sepsis-Related Organ Failure Assessment score,23 MOD score,24 days on mechanical ventilation, ICU and hospital outcomes and stay, 28-day mortality, pulmonary measurements, physiologic measurements, ventilatory measurements, cardiovascular measurements, adverse events, extrapulmonary organ failures, sedation, and daily chest x-ray. All measurements and data were recorded at study inclusion, at 6 hours after inclusion, and between 6:00 am and 8:00 am on days 1, 2, 3, 4, 7, 14, 21, and 28.
Organ failure was defined as a Sepsis-Related Organ Failure Assessment score23 > 2, and MOD requires ≥ 2 organ failures. Organ-dysfunction-free days were defined as days alive and free of any organ dysfunction,15,17 and ventilator-free days were defined as days of unassisted breathing, both calculated at 28 days (all deaths occurring prior to day 28 were considered as zero organ-dysfunction-free or ventilator-free days).18 Subjects were followed until hospital discharge or death.
Statistical Analysis
Normality of data distribution was assessed using the Kolmogorov-Smirnov test. Quantitative variables with normal distribution are expressed as mean ± SD, and were compared using the Student t test. Non-normal distribution variables are shown as medians and interquartile ranges, and were compared using the Mann-Whitney test. Qualitative variables are shown as percentages, and were compared with the chi-square test. Kaplan-Meier analysis with log-rank test was applied to compare survival at 28 days between groups. Statistical significance was set at P < .05, and results are expressed with their 95% confidence intervals. Statistical analysis was performed using statistics software (SPSS 15.0, SPSS, Chicago, Illinois).
Results
A total of 159 patients met the criteria for ARDS during the study period, 70 of whom were randomized to either compliance-guided (n = 34) or FIO2-guided PEEP adjustment (n = 36) (Fig. 1). No patients were excluded after randomization or discharged from hospital earlier than 28 days.
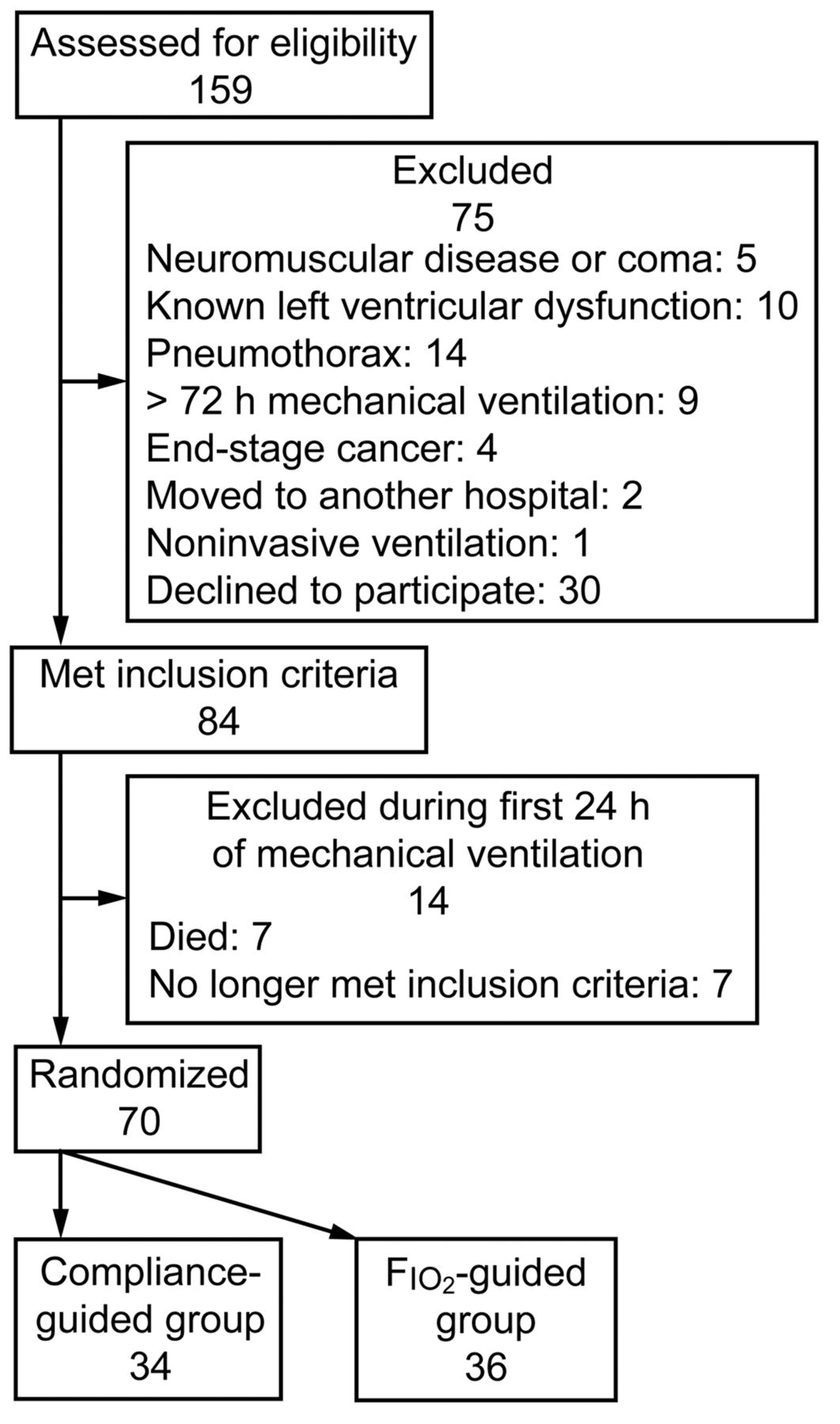
Screening and enrollment.
The main cause of ARDS was infection (n = 50, 71.4%) (detailed causes of ARDS per study group are shown in the supplementary materials at http://www.rcjournal.com). There were no significant differences in subject characteristics between study groups at randomization, except for the high incidence of MOD in the compliance-guided group (Table 1).
Baseline Characteristics of Subjects at Study Inclusion
Physiological Measurements
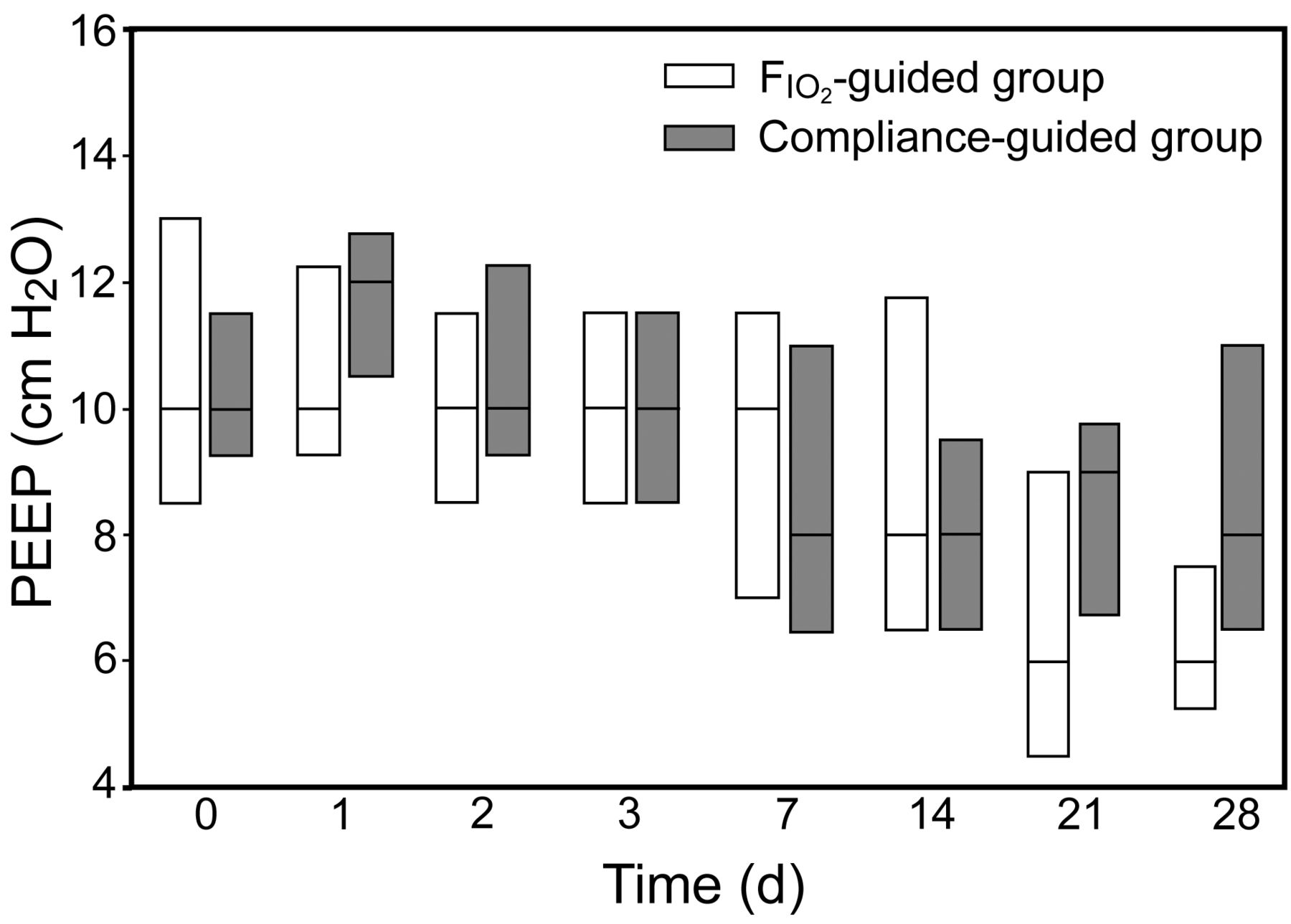
There was no difference in median PEEP at study entry (Fig. 2). Figure 3 shows the ventilatory parameters over the 28-day study period. There was no significant difference in PaO2/FIO2. There was a trend toward better oxygenation in the compliance-guided group over the first 2 weeks of study (see Fig. 3 and the supplementary materials at http://www.rcjournal.com). In the compliance-guided group there was also a nonsignificantly higher pulmonary compliance and lower airway pressure (see Fig. 3 and the supplementary materials at http://www.rcjournal.com). There were no differences in pH, VT, intrinsic PEEP, or breathing frequency (see the supplementary materials at http://www.rcjournal.com).

PEEP in the first 28 days.

PaO2/FIO2, static compliance, peak pressure, and plateau pressure.
In a post-hoc analysis we found that 80% of the subjects in the compliance-guided group would have had a different PEEP if set according to the FIO2/PEEP table. There were no limitations in daily PEEP changes, rather than the measurement frequency of PEEP.
Clinical Outcomes
The compliance-guided group had significantly more MOD-free days at day 28 (Table 2), in spite of a higher baseline incidence (see Table 1), as well as more ventilator-free days and hemodynamic failure-free days.
Clinical Outcomes
Twelve subjects developed barotrauma after randomization: 6 per study group (see Table 2). A total of 9 episodes of barotrauma occurred during the first week: 5 in the compliance-guided group, and 4 in the FIO2-guided group. One subject in the compliance-guided group and 2 in FIO2-guided group developed barotrauma in the second week of study.
Global 28-day mortality was 30% (21 subjects), with a hospital mortality of 42.8% (30 subjects). 28-day mortality was 20.6% (n = 7) in the compliance-guided group and 38.9% (n = 14) in the FIO2-guided group (P = .12) (Fig. 4). The main causes of death were multi-organ failure (n = 50, 71.4%) and refractory hypoxemia (n = 10, 14.3%). Subjects who died had a higher Sepsis-Related Organ Failure Assessment score23 at inclusion (11.4 ± 0.7 vs 8.1 ± 0.5, P = .01), as well as lower PaO2/FIO2 (126.4 ± 9.6 mm Hg vs 145.1 ± 4.3 mm Hg, P = .04) and a higher Lung Injury Score22 (3.25 [2.50–3.50] vs 3.00 [2.50–3.25], P = .04).
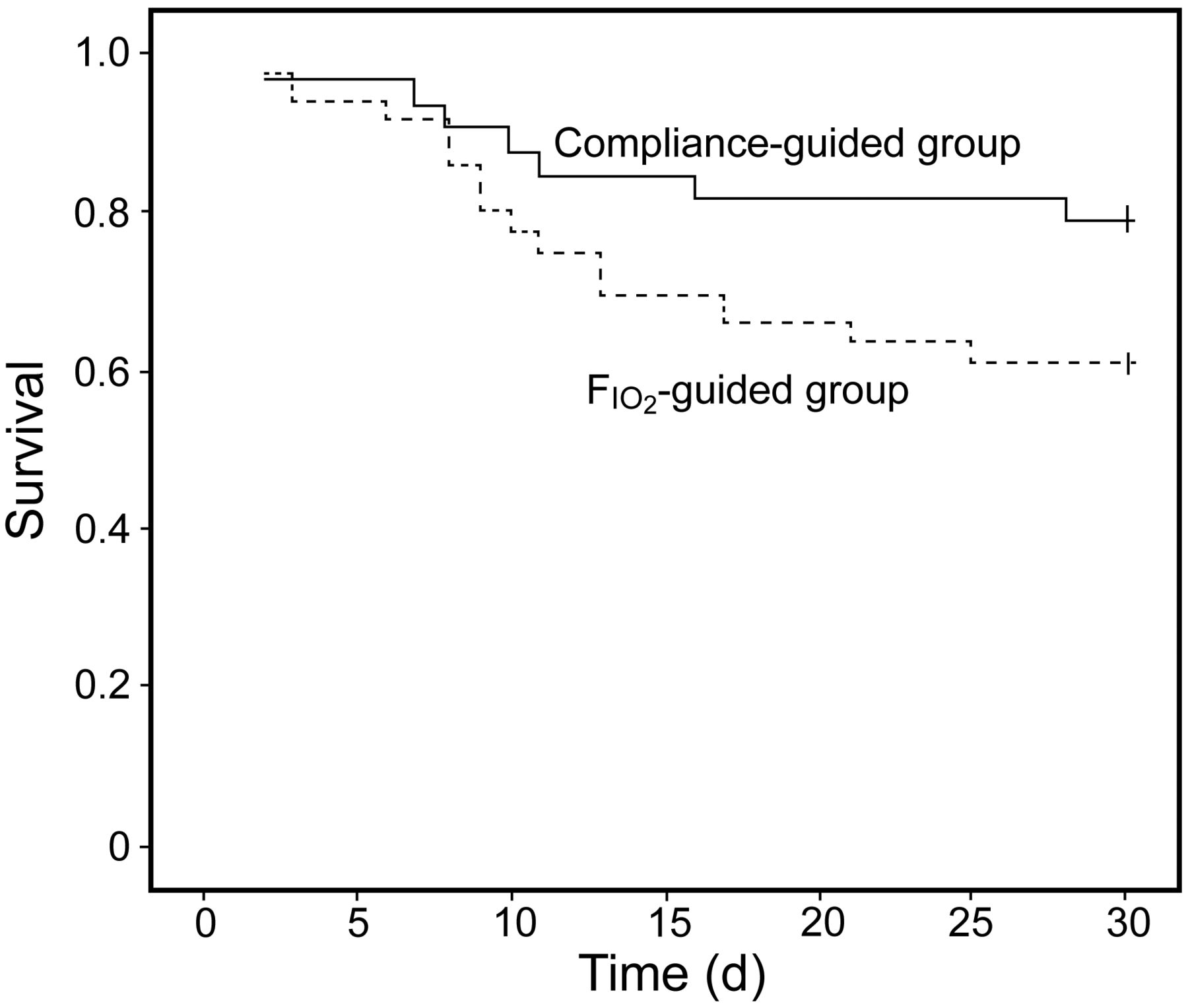
Kaplan-Meier curves for survival.
There were no significant differences in hemodynamic variables or sedative dosage between the groups (see the supplementary materials at http://www.rcjournal.com). There were no complications associated with insertion of the pulmonary artery catheter.
Discussion
In subjects with ARDS, ventilated with low VT and airway pressure limited to 30 cm H2O, compliance-guided PEEP adjustment, compared to FIO2-guided PEEP adjustment, had no significant effect on oxygenation, although it was associated with a significant reduction of the duration of MOD.
To our knowledge, static-compliance-guided PEEP has not previously been studied in a large group of subjects under lung-protective ventilation.25 Interestingly, there was no significant difference in the mean PEEP applied to the 2 groups. In previous studies PEEP was higher if set according to “compliance.”13,17,26 Although mean PEEP was similar, our post-hoc analysis showed that 80% of the compliance-guided subjects would have received different PEEP than did the control group. Hypothetically, subjects with customized PEEP might have been on higher or lower PEEP than those prescribed PEEP according to the PEEP/FIO2 table. Thus, the similar mean PEEP value, in our opinion, does not exclude the possibility that individual compliance-guided PEEP might be distributed over a wider range and might be associated with less ventilator-induced lung injury.
We also found that subjects on compliance-guided PEEP had nonsignificantly lower plateau pressures over the first 21 days of study (see Fig. 3). This could be explained by improved alveolar recruitment, since other respiratory parameters were set according to the same protocol in both groups, but this needs to be confirmed in a larger study. In previous studies, lower plateau pressure has been associated with lower mortality,18 and, similar to our findings, shorter duration of MOD.17,18
There have been only 3 randomized controlled clinical trials in which PEEP set according to the pressure-volume curve was compared with other methods of setting PEEP.13–15 Those studies compared higher versus lower VT and found progressive improvement of oxygenation14 over the first week.13,15 There were no data about the course of oxygenation beyond the first week. Those studies differed from ours in that PEEP was set slightly above the lower inflection point of the quasi-static pressure-volume curve. That method correlates poorly with alveolar recruitment, and therefore with total alveolar compliance.27 We also found a nonsignificant improvement in oxygenation in the compliance-guided group during the first 2 weeks, but this effect was not observed at later stages. Unlike in previous studies, improved oxygenation, if confirmed, may be attributed to the method of PEEP determination, since this was the only difference between the 2 study groups. Comparisons of oxygenation data are methodologically very difficult because of important differences in clinical course and how death and weaning should statistically be accounted for. In addition, in later stages of ARDS, with increased lung fibrosis,28,29 the use of the pressure-volume curve may be less effective in achieving alveolar recruitment and, consequently, in improving oxygenation.
We observed that customizing PEEP to the individual subject was associated with shorter duration of MOD at 28 days. It is reasonable to assume that this effect is the cause for the strong trend toward lower mortality in this study group. Previous studies have been criticized for similar results because subjects were ventilated with high VT, which is associated with higher mortality.18 A meta-analysis30 of 3 studies13–15 showed significantly lower mortality if PEEP was determined according to the pressure-volume curve. This effect on duration of MOD may be related to a reduced release of inflammatory cytokines. Several clinical studies have confirmed that an array of inflammatory cytokines is released into the systemic circulation as a consequence of high VT or high PEEP, which correlates with higher morbidity and mortality.14,18,31,32
Other studies have compared methods of setting PEEP. The Express study17 showed that, compared to a fixed and low PEEP, an individualized PEEP set at the highest value allowing a plateau pressure of 28–30 cm H2O is associated with significant increase of MOD-free days at 28 days, without improving survival. Talmor et al26 compared the application of fixed PEEP according to the ARDS Network standard-of-care recommendations,18 with an individualized method based on transpulmonary pressure at end-expiration. They found improved oxygenation, as well as a trend toward lower mortality in the customized PEEP group. It is interesting to note that, as in our study, Talmor et al found that the respiratory-system compliance appeared to be higher in their esophageal-pressure-guided group.26 Unlike in our study, however, they determined PEEP decrementally after a recruitment maneuver, which has been demonstrated to influence the evaluation of lung compliance according to the pressure-volume curve.27,33
Grasso et al34 found that, compared to the ARDS Network protocol,18 in subjects with a focal pattern of loss of aeration, PEEP is lower if set according to stress index and that the application of the ARDS Network protocol18 induces alveolar hyperinsufflation and increases cytokine plasma levels. The LOVs16 study found a lower incidence of refractory hypoxemia and need for rescue therapies associated with the application of PEEP according to FIO2 after a 40-second, 40 cm H2O airway pressure recruitment maneuver, compared to the ARDS Network protocol18 without previous recruitment maneuver, although without a statistically significant difference in rates of all-cause hospital mortality or barotrauma.
In our study 12 subjects (17%) developed barotrauma. The incidence of barotrauma in ARDS has been reported to range between 0 and > 76%,35 although recent studies show reduced incidences between 6% and 10%.16,17,36,37 Risk factors for barotrauma included high peak airway pressure, large VT, and the level of acute lung injury.38 The slightly higher incidence of barotrauma in our study may be explained by the high Lung Injury Score,22 as large VT and high peak airway pressure were avoided. The incidence of barotrauma was similar in our 2 study groups. Previous studies have not found differences in the incidence of barotrauma according the different levels or methods of PEEP applied.16,17,36,37
Our study has several limitations. Being a pilot study with the aim to provide a basis for a future multicenter study, it had a small sample size and its results require confirmation. The study was carried out in a single center, and included only 44% of subjects who met the inclusion criteria. Although randomized, the study was unblinded, and bias cannot be excluded. Some difficulties in setting PEEP at best compliance became apparent during the study. At times, several time-consuming attempts were required to find the best PEEP in the compliance group, including the need for muscle relaxants, or the study procedures had to be interrupted to allow for endotracheal suctioning. We also did not measure inflammatory cytokines to support the findings on MOD.
Conclusions
In conclusion, this randomized controlled pilot trial showed that individualized PEEP selection based on the best static compliance in subjects with ARDS treated with low VT and limited plateau pressure did not improve oxygenation, but was associated with a significant increase in organ-dysfunction-free days and a strong trend toward lower mortality at day 28. Larger, randomized, multicenter trials are necessary to validate this approach as an integral part of lung-protective strategy.
Footnotes
- Correspondence: María-Consuelo Pintado MD PhD, Intensive Care Unit, Hospital Universitario Príncipe de Asturias, Carretera Alcalá-Meco, SN E-28805, Alcalá de Henares, Madrid, Spain. E-mail: consuelopintado{at}yahoo.es.
Supplementary material related to this paper is available at http://www.rcjournal.com.
See the Related Editorial on Page 1552
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}