

Abstract
BACKGROUND: Our objective was to evaluate the feasibility, the quality of synchronization, and the influence on respiratory parameters of the noninvasive neurally adjusted ventilatory assist (NIV-NAVA) mode in infants after cardiac bypass surgery. We conducted a prospective, randomized cross-over study in infants undergoing noninvasive ventilation (NIV) after cardiac surgery.
METHODS: Subjects were 10 infants < 5 kg. After extubation, subjects underwent 2 consecutive ventilatory modes after randomization into groups. In the CPAP first group, the subjects were ventilated first in nasal CPAP-1 and then in NIV-NAVA-2 for 30 min in each mode. In the NIV-NAVA first group, periods were reversed. All children were ventilated using the same interface.
RESULTS: The analysis of curves showed a synchronization rate of 99.3% for all respiratory cycles. The rate of pneumatic inspiratory trigger was 3.4%. Asynchronies were infrequent. Some typical respiratory patterns (continuous effort and discontinuous inspiration) were found at rates of 10.9% and 31.1%, respectively. The respiratory trends showed a lower maximum diaphragmatic electrical activity (EAdi(max)) in NIV-NAVA periods compared with CPAP periods (P < .001 in the beginning of periods). The breathing frequency decreased significantly during the nasal CPAP-2 and NIV-NAVA-1 periods (P < .05). The inspiratory pressure increased significantly during the NIV-NAVA-1 and NIV-NAVA-2 periods (P < .05), but there was no significant difference for each parameter when comparing Δ values between the beginning and the end of each period. The EAdi signal was easy to obtain in all subjects, and no major side effects were associated with the use of NIV-NAVA.
CONCLUSIONS: NIV-NAVA allows good synchronization in bi-level NIV in infant cardiac subjects weighing < 5 kg. The analysis of respiratory parameters shows that NIV NAVA decreases the work of breathing more effectively than nasal CPAP. The study shows some typical respiratory patterns in infants. (ClinicalTrials.gov registration NCT01570933.)
Introduction
Newborns with congenital cardiac malformation who undergo cardiac surgery with cardiopulmonary bypass in the first days of life often require noninvasive ventilation (NIV) subsequent to conventional ventilation after extubation. Bi-level synchronized NIV could be helpful in improving ventilatory support in some patients, but is difficult to achieve in newborns. Almost all modern neonatal ventilators use pressure or flow signals to detect inspiratory trigger and synchronize ventilatory support with the breathing of the patient. Breath detection in low-weight patients is difficult because of the low pressures and tidal volumes developed by the patients and the high leakage flow on the currently available interfaces.1
With neurally adjusted ventilatory assist (NAVA), it is possible to record the diaphragmatic electrical activity (EAdi) via an esophageal catheter and thereby synchronize breaths from the ventilator with the inspiratory efforts of the patient. In NAVA, the level of assist is coupled to the EAdi signal.2 Adult and pediatric studies showed that NAVA increases breath-to-breath variability and improves patient-ventilator synchrony and patient comfort.3–9 This last improvement is also effective in NIV in adult and pediatric subjects10,11 and in very low birthweight infants, even in the presence of large leaks.12
To our knowledge, no previous study was designed to evaluate this ventilation mode exclusively in the postoperative period after cardiac surgery in newborns. The purpose of this study is to evaluate the feasibility and the quality of synchronization of this ventilatory mode and its influence on ventilatory parameters in this category of patients.
QUICK LOOK
Current knowledge
Neurally adjusted ventilator assist (NAVA) measures the electrical signal of the diaphragm (EAdi) and uses this signal to trigger and cycle the ventilator. The level of NAVA support is also controlled as an amplification of the EAdi signal. Breath to breath variability and patient comfort have been demonstrated with NAVA compared to pressure-support ventilation.
What this paper contributes to our knowledge
In a population of infants who had undergone cardiac bypass surgery and who weighed < 5 kg, noninvasive ventilation (NIV) in NIV-NAVA mode provided good synchronization after extubation. Compared with nasal CPAP alone, NIV-NAVA resulted in a reduction in EAdi, suggesting an improvement in off-loading the diaphragm.
Methods
Subjects
In our unit, all patients with a weight below 5 kg benefit from NIV after conventional ventilation following cardiac surgery with bypass. Children were thus eligible for inclusion in the study if their weight was below 5 kg, they were in the postoperative period after cardiac surgery with cardiopulmonary bypass (maximum 10 d after surgery), and they were receiving conventional ventilation. Exclusion criteria were: high frequency oscillation ventilation, extubation criteria not fulfilled on day 10, proven or suspected sepsis, esophageal pathology (except for gastroesophageal reflux). This study was approved by the ethics committee of our hospital (2011/15SEP/364). Written informed consent from each subject's parents was obtained.
Study Design
We conducted a prospective, randomized, cross-over clinical trial comparing the use of nasal CPAP versus NIV-NAVA.
Protocol
The 6 French/50 cm esophageal NAVA catheter (Maquet Critical, Wayne, New Jersey) was placed after informed consent by the subject's parents and at least 30 min before the beginning of the study, according to the manufacturer's recommendations. The ventilation mode was then switched to pressure support by keeping the same PEEP and defining a pressure support of 10 cm H2O. After 30 min, the child was extubated according to the procedures of the service. The extubation criteria were effective coughing and swallowing, stable cardiovascular status, no inotrope/vasoactive drugs (except for dobutamine ≤ 5 μg/kg/min or milrinone), corrected metabolic disorders, adequate oxygenation (pulse oximetry within the target values of the child), inspiratory pressure ≤ 30 cm H2O, PEEP between 4 and 6 cm H2O, arterial or venous pH ≥ 7.25, no sedation (excepted midazolam < 1 μg/kg/min or sufentanyl < 0.2 μg/kg/h) or appropriate level of consciousness, and no scheduled surgery in the next 12 h. An epinephrine nebulization could be given before starting NIV in case of respiratory distress due to laryngeal edema.
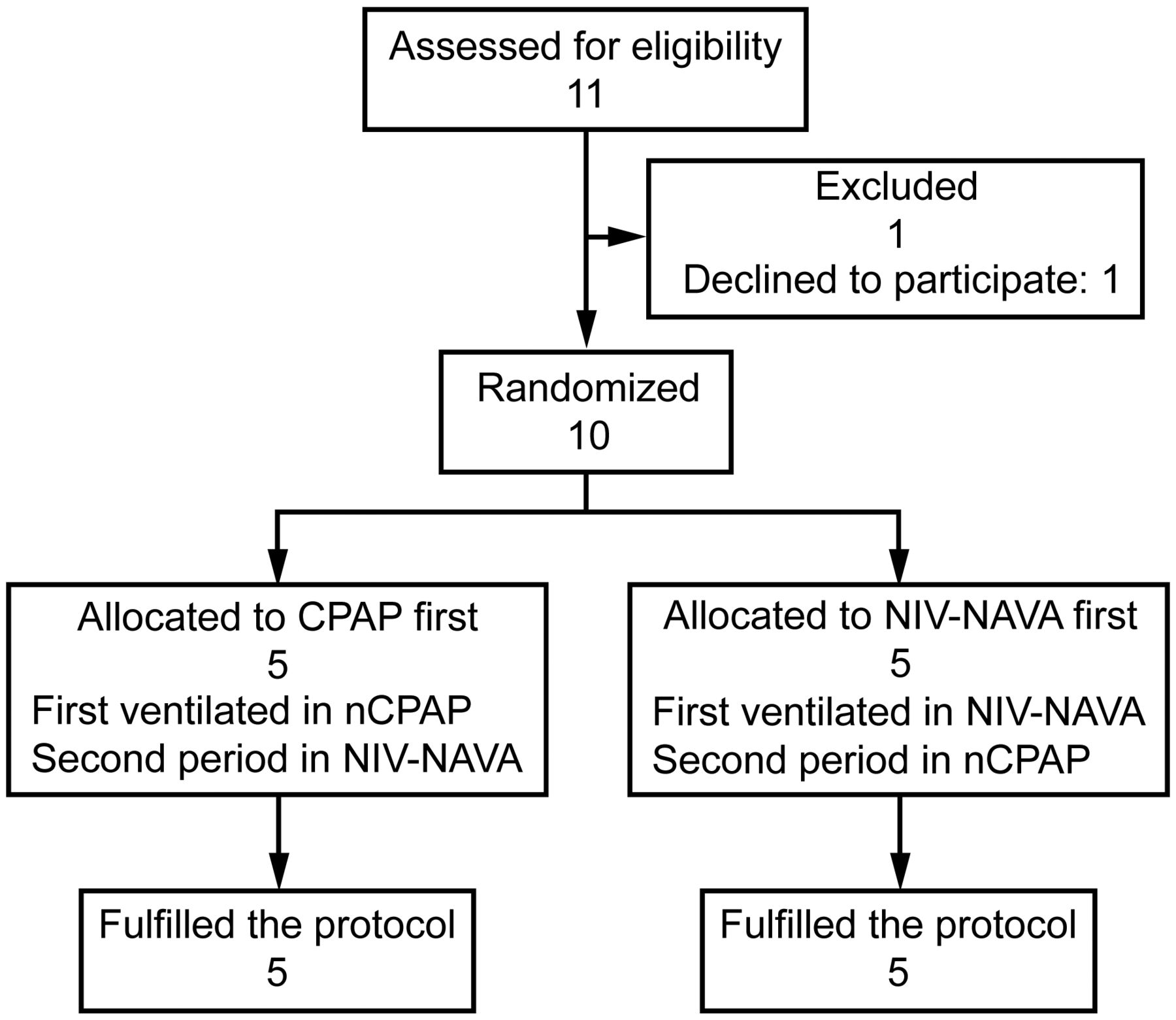
After extubation, subjects were randomized by manual blind toss into the CPAP first or NIV-NAVA first groups. In the CPAP first group, the subjects were ventilated first in nasal CPAP-1 and then in NIV-NAVA-2. In the NIV-NAVA first group, the subjects were ventilated first in NIV-NAVA-1 and then in nasal CPAP-2. Each mode was used for 30 min (Fig. 1). During the first 15 min, the ventilation parameters were adapted according to the procedures below: FIO2 according to targeted SpO2 values of the child and/or 10% higher than FIO2 in invasive ventilation mode, PEEP/CPAP level between 4 and 6 cm H2O to minimize respiratory efforts, and adaptation of the NIV-NAVA level to reach an EAdi level equal to the mean EAdi level over the last 5 min of the invasive mode. Inspiratory pressure was limited to 30 cm H2O. At any time, if re-intubation criteria were met, the child was re-intubated and returned to conventional ventilation. The re-intubation criteria were signs of discomfort, sweating, increased signs of respiratory distress (nasal flaring, increased work of breathing, paradoxical breathing, grunting), desaturation (pulse oximetry < target values for the child), breathing rhythm > 2 times the normal values, heart rhythm increased by > 20% compared with basal status, systolic arterial blood pressure increased by > 20% compared with basal status or < limit values for age, hypoventilation (confirmed by arterial or venous blood gases), or neurological impairment.

Flow diagram. nCPAP = nasal CPAP, NIV-NAVA = noninvasive neurally adjusted ventilatory assist.
All children were ventilated using the Miniflow interface (Medical Innovations GmbH, Puchheim, Germany) with nasal prongs adapted to the morphology of the child. A Servo-i ventilator (Maquet) administered nasal CPAP and NIV-NAVA mode.
Data Collection
The curve analysis was performed using the Servo-tracker (Maquet) and Acqknowledge (Biopac Systems, Goleta, California) software. The Servo-tracker software recorded pressure, flow, and EAdi signals at a 100-Hz rate at min 16, 21, and 29 in NIV-NAVA mode. Numeric data obtained were then used to plot ventilation curves. Different typical respiratory patterns could then be identified and analyzed.
Ventilator asynchronies were defined as follows. Double triggering was characterized by 2 consecutive inspiratory cycles without intermediate expiratory time,13 with the EAdi in its inspiratory phase and not varying. An ineffective effort was characterized by an increase in the EAdi curve without pressure or flow curve modification. Subject's demand to receive ventilation was not rewarded,14 and they were not ventilated for that muscular contraction. A pneumatic auto-triggering was characterized by increase in pressure and flow, but with a flat EAdi signal. Although the diaphragm did not contract, the ventilator was triggered. For our study, we defined auto-triggering as a minimum increase in pressure of 2 cm H2O without EAdi modification and without a drop in pressure before the beginning of inspiration. In this case, a ventilator-assisted breath was delivered in the absence of subject effort or initiation.14
The synchronization analysis also included the delay times (dT) between the start of the increase in the EAdi signal and the start of pressurization by the ventilator. These dT were calculated for every respiratory cycle, including those present in continuous efforts. Spahija et al5 measured mean dT of 105 ms, whereas Piquilloud et al6 measured median dT of 69 ms in adult subjects. In a pediatric study, de la Oliva et al3 reported median dT < 50 ms. Because infants have short inspiratory times, we arbitrarily defined a dT of > 100 ms as abnormal.
Other typical respiratory patterns were defined as follows. A discontinuous inspiration was defined as respiratory cycles characterized by an escalation curve during inspiration. This escalation had to be present on the EAdi curve and on the pressure curve (Fig. 2). A continuous effort was represented by respiratory cycles during which the patient breathed with a tonic activity of the diaphragm superior to 1 μV. Moreover, the intermediate EAdi(min) was superior to the EAdi(min) from the start, and the continuous effort stopped when the EAdi(min) at the end was equal to the one at the start. This is mainly due to persistent diaphragmatic activity at expiration (Fig. 3). A pneumatic inspiratory trigger, also called inspiratory threshold trigger, is characterized by a drop in pressure just before the beginning of the inspiration (Fig. 4). This pneumatic trigger is quite normal in conventional ventilation and allows the patient to trigger the inspiratory cycles. In NIV-NAVA mode, the inspiratory trigger depends primarily on the EAdi signal (neurological trigger) and secondarily on pneumatic values like flow or pressure. This mechanism operates under the law of first come, first served.15 In children, pneumatic inspiratory trigger could probably be related to prior activation of accessory respiratory muscles (before diaphragmatic contraction) or to electrocardiograph filtering of the EAdi signal. An early expiration was represented by a pressure drop at the end of expiration. The pressure fell below the PEEP. It is due to a delay during the closing of the expiratory valve placed at the outlet of the respirator. This closing delay leads to a more important pressure drop at the end of expiration. This phenomenon is uncontrollable: it is an algorithm stored in the memory of the ventilator (Fig. 4).

Airway pressure (Paw) and diaphragmatic electrical activity (EAdi) curves (A: simulated, B: actual subject) showing a discontinuous inspiration. The escalation of the curves is similar in both the pressure and diaphragmatic electrical activity curve.

Diaphragmatic electrical activity (EAdi) curves showing a continuous effort (A: simulated, B: actual subject curve). The intermediate minimum EAdi (EAdi min) is higher than the minimum EAdi from the start and at the end. The intermediate minimum EAdi is higher than 1 μV.

Actual subject pressure and diaphragmatic electrical activity (EAdi) curves showing pneumatic inspiratory trigger (*) and early expiration (**).
Respiratory parameters were recorded by Servo-i software. The trends in EAdi(max), breathing frequency, and inspiratory pressure were recorded and compared in min 2–6 and in min 25–29 in each mode.
Statistical Methods
All results were expressed in terms of mean ± SD. Statistical analysis was performed using SPSS 20.0 software (SPSS, Chicago, Illinois). The Wilcoxon rank-sum test was used to compare the age and the weight between the groups. The Student t test was used to compare the quantitative variables between the beginning and the end of each mode. The analysis of variance test was used to compare the differences of averaged values (Δ) between the beginning and the end of each period for each mode. Significance level was set at P < .05 for all tests.
Results
Subjects
Ten cardiac subjects were included in the study: 5 in the CPAP-1 group, and 5 in the NIV-NAVA-1 group. The main characteristics of the included subjects are summarized in Table 1. There were no significant differences in demographic data. The median ages in the CPAP-1 group and NIV-NAVA-1 group were, respectively, 4.0 wk (interquartile range 2.5–10.5 wk) and 8.0 wk (IQR 4.5–15.5 wk) (P = .52). The median weights were, respectively, 3.7 kg (IQR 2.6–4.6 kg) and 3.9 kg (IQR 3.2–4.4 kg) (P = 1.00).
Main Clinical Characteristics of the Subjects
Synchronization and Respiratory Patterns
In NIV-NAVA mode, a total of 1,422 respiratory cycles were analyzed (including 454 occurring during continuous effort periods). The analysis of curves showed a synchronization rate of 99.3% for all respiratory cycles: abnormal dT was present in only 10/1,422 cycles. Asynchronies were infrequent and found at the following rates: double triggering 1.5%, ineffective efforts 0.3%, and pneumatic auto-triggering 1.8%.
The continuous efforts represented 10.9% of the respiratory cycles (118/1,086 cycles), with a mean of 3.8 cycles in each continuous effort. The pneumatic inspiratory triggers and early expirations were, respectively, present at a rate of 3.4% (37/1,086 cycles) and 25% (272/1,086 cycles). The discontinuous inspirations represented 31.1% of the respiratory cycles (338/1,086 cycles). Some curves were not interpretable for a period of 92 s for a total recording time of 1,800 s (5.1%).
Respiratory Parameters
Pre-extubation mean EAdi(max) was 8.80 ± 4.44 μV in the CPAP-1 group and 9.87 ± 6.62 μV in the NIV-NAVA-1 group. Mean CPAP level, PEEP, and NAVA level were, respectively, 5.40 ± 0.55 cm H2O, 5.20 ± 0.45 cm H2O, and 0.86 ± 0.37 cm H2O/μV in the CPAP-1 group and 5.00 ± 0.71 cm H2O, 4.80 ± 0.84 cm H2O, and 0.98 ± 0.30 cm H2O/μV in the NIV-NAVA-1 group.
The respiratory trends indicated a significant decrease in EAdi(max) during the nasal CPAP-1 period (P < .001). The breathing frequency decreased significantly during the nasal CPAP-2 and NIV-NAVA-1 periods (P < .05). The inspiratory pressure increased significantly during the NIV-NAVA-1 and NIV-NAVA-2 periods (P < .05) (Table 2). Because of the great variability of respiratory parameters, the Δ values between the beginning (min 2–6) and the end (min 25–29) were compared. They showed no significant difference between the groups.
Effects of Nasal CPAP or NIV-NAVA on Respiratory Parameters
When comparing all CPAP periods with all NIV-NAVA periods, the only significant differences were a greater EAdi(max) in the beginning of the CPAP periods compared with the beginning of the NIV-NAVA periods (respectively, 16.97 ± 7.68 μV and 10.55 ± 5.60 μV, P < .001) and a greater breathing frequency at the end of the NIV-NAVA periods compared with the end of the CPAP periods (respectively, 51.64 ± 12.02 breaths/min and 40.35 ± 11.39 breaths/min, P < .001) (Table 3).
Comparisons of the Respiratory Parameters Between CPAP Periods and NIV-NAVA Periods
Feasibility and Safety
EAdi signal and correct placement of esophageal NAVA catheters was easy to obtain in all subjects. All subjects could be ventilated in NAVA mode and achieved the 30-min ventilation period without premature arrest of the NIV-NAVA mode. No subject needed to be re-intubated. No major side effects were associated with the use of nasal CPAP or NIV-NAVA. However, the feeding channel of one esophageal NAVA catheter was defective, so the child could not be fed. No nasal wounds were observed. Furthermore, there was >70% leakage.
Discussion
This study shows that the use of the electric activity of the diaphragm to allow synchronization between the patient and the ventilator is effective with normal delays of synchronization in 99.3% of the cycles. Asynchronies (pneumatic auto-triggering, double triggering, and ineffective efforts) are rare. The EAdi signal is responsible for the inspiratory triggering in 93.3% of the cycles, whereas pneumatic inspiratory trigger, auto-triggering, and double triggering occurred in the other cycles. This study highlights the existence of typical respiratory patterns.
The analysis of dT enabled us to verify whether the pressure curves and the flow were synchronized in-time with the EAdi curve. Previous studies showed a small delay known as the neuro-ventilatory normal delay. This delay is explained by the neuro-ventilatory coupling of the patient who corresponds to the time between the start of the activation of the diaphragm and the start of the appearance of the pressure.16 It corresponds to the time required to reach the neurological trigger of 0.5 μV and varies from cycle to cycle with an approximate value of 65 ms. When the delay exceeded the normal neuro-ventilatory delay (that we arbitrarily set at 100 ms), the ventilator was defined as out of sync with the patient. Abnormal dT was present only in 10/1,422 cycles. However, the arbitrary definition of this abnormal delay could be challenged.
Noninvasive bi-level ventilation is difficult to achieve in infants and children. Pressure-support ventilation does not offer good synchronization in these patients. Previous studies with small numbers of patients and short study periods confirmed the superiority of NIV-NAVA mode compared with pressure support mode in infants and children (< 5 y old).11 Our results show good synchronization and patient-ventilator interactions in NIV-NAVA mode in small infants weighing < 5 kg. This can offer better comfort for the patient because the ventilator tends to mimic the normal shapes of patient breathing and allows normal variations of respiration. However, the comfort of our subjects was difficult to assess because of their young age, absence of accurate comfort scales, and the short term of the study. Furthermore, the time of extubation always remains a challenging period for small patients after cardiac surgery, with some discomfort due to the increased work of breathing and the respiratory distress often present at this time. Previous studies suggest that improved synchronization by means of the EAdi results in greater comfort for pediatric patients,3 but synchronization alone cannot guarantee patient comfort. Bi-level ventilation can also lead to greater discomfort because of the increased gas flow through the nasal cannula during inspiratory periods. On the other hand, synchronized inspiratory support could probably decrease the patient's respiratory work and, therefore, increase comfort. An additional study, with longer comparison periods and accurate tools to measure patient comfort, would be interesting.
The Miniflow interface with nasal prongs allowed us to perform NIV-NAVA on all of our subjects, despite high leakage levels, inherent to that type of interface. The use of the EAdi signal allows the inspiratory trigger to be reliable, even with significant leakage. The diversity of the shapes of infant faces and the diversity of available nasal or facial interfaces makes it difficult to compare patients receiving NIV. One strength of our study is the use of the same interface for all subjects.
Previous studies reported typical neural respiratory patterns by analyzing EAdi waveforms obtained via esophageal sensors in intubated17 and spontaneously breathing infants.18 They showed that infants tend to maintain some electrical diaphragmatic activity during the expiratory periods. This tonic EAdi is believed to help the child maintain end-expiratory lung volumes, by creating an auto-PEEP. This was confirmed by the observation of the increase in this tonic activity while the PEEP was set at 0 cm H2O in ventilated patients.17 We also found this expiratory tonic activity to be frequent in our subjects: respiratory cycles with continuous efforts represented 10.9% of the respiratory cycles. Given the fact that, in our study, the initial PEEP after extubation was set at 4–6 cm H2O and could not be changed after the adaptation phase, we could not evaluate the effect of the level of PEEP on these continuous efforts.
Discontinuous inspiration was present in 31.1% of the respiratory cycles. We hypothesize that this particular aspect of the inspiratory curve of the EAdi signal is linked to the crying of the infant and reflects the activity of the diaphragm during sobbing, but we were not able to demonstrate this effect.
When looking to the evolution of EAdi(max), results showed that EAdi(max) was lower in NIV-NAVA periods compared with CPAP periods (with significant results at the beginning of the periods). After extubation, EAdi(max) increased less in NIV-NAVA-1 than in nasal CPAP-1. Similarly, during the ventilatory mode changes, the EAdi(max) decreased when switching from nasal CPAP-1 to NIV-NAVA-2, whereas it increased when switching from NIV-NAVA-1 to nasal CPAP-2. This evolution of EAdi(max) was expected because of the pressure support delivered by this mode, compared with nasal CPAP. Our results tend to show that NIV-NAVA decreased the work of breathing more rapidly than nasal CPAP. However, the evolution of the other respiratory parameters is not clear enough to allow recommendations for the best NIV strategy after extubation in infants recovering from cardiac surgery. NIV-NAVA does not seem to be superior to nasal CPAP, based on an analysis of the evolution of the breathing frequency. Some subjects showed a significant increase in inspiratory pressure during the NIV-NAVA periods, which was related to a nonsignificant increase inEAdi during the same period. This could be related to a non-measurable increase in discomfort at the beginning of the NIV-NAVA mode because of the increased gas flow through the nasal cannula. A longer period might show a reverse tendency, after adaptation of the child to this new mode.
Because of important coefficients of variation for each parameter in each mode, we also compared the Δ values between the beginning and the end of each mode for each parameter and did not find any significant difference. The small sample size may influence these results. Nevertheless, our clinical impression was that at least two subjects actually benefited from this mode, thereby avoiding re-intubation, but this is not confirmed by their respiratory parameters.
Our study has several limitations. The first is the small number of subjects and the short analysis periods, although we examined 1,422 respiratory cycles in total. A second limitation could be related to the systematic use of NIV after extubation in all subjects. Some of them probably did not actually need this ventilatory support. The lower acuity level of some subjects can make it difficult to show a significant difference in respiratory parameters, but the main objective of the study was to show the feasibility of NIV-NAVA after cardiac surgery in infants weighing < 5 kg. Furthermore, the design of our study, with the same subjects ventilated in different modes at different times, makes it difficult to discriminate the effects of each mode on respiratory parameters and the natural evolution of the underlying respiratory conditions of those subjects. Another study with more subjects and a different design could help us to propose more accurate ventilation strategies. Nevertheless, our study is, to our knowledge, the first to show good synchronization with the NIV-NAVA mode in infants weighing < 5 kg after cardiopulmonary bypass for congenital cardiac surgery.
Conclusions
In our population of infants weighing < 5 kg who underwent cardiac bypass surgery, bi-level noninvasive ventilation in NIV-NAVA mode allows good synchronization after extubation. The evolution of EAdi(max) shows a better reduction of the work of breathing by this mode compared with nasal CPAP, but more studies, with more subjects, longer ventilation times, and comfort assessment are needed to evaluate the benefits for the patients. Furthermore, our study confirms the existence of typical respiratory patterns in infants, such as continuous efforts and discontinuous inspiration. The actual significance of these patterns needs to be assessed.
Footnotes
- Correspondence: Laurent Houtekie MD, University Hospital Saint-Luc, Pediatric Intensive Care Unit, 10 avenue Hippocrate, 1200 Brussels, Belgium. E-mail: laurent.houtekie{at}uclouvain.be.
The authors have declared no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}