

Abstract
BACKGROUND: The benefits of inspiratory muscle training (IMT) for patients with COPD are documented in the literature, but its isolated effect or association with other interventions, the best training methods, and what type of patient benefits the most are not clear. We sought to assess the effects of IMT on respiratory muscle strength, pulmonary function, dyspnea, functional capacity, and quality of life for subjects with COPD, considering IMT isolated or association with other interventions, presence of inspiratory muscle weakness, training load, and intervention time.
METHODS: We searched the MEDLINE, EMBASE, PEDro, Cochrane CENTRAL, and LILACS databases in June 2018. We also performed a manual search of references in the studies found in the database search and included in this analysis. We included randomized controlled trials that investigated the above-mentioned outcomes and assessed IMT, either isolated or associated with other interventions, in comparison with a control group, placebo, or other interventions, in subjects with COPD. We used the GRADE approach to evaluate the quality of the evidence.
RESULTS: Of 1,230 search results, 48 were included (N = 1,996 subjects). Isolated IMT increased PImax (10.64 cm H2O, 95% CI 7.61–13.66), distance walked in 6-min-walk test (34.28 m; 95% CI 29.43–39.14), and FEV1 (0.08, 95% CI 0.02–0.13). However, there was no improvement in dyspnea and quality of life. The presence of inspiratory muscle weakness did not change the results; higher loads (60–80% of PImax) promoted a greater improvement in these outcomes, and a shorter intervention time (4 weeks) improved PImax, but longer intervention times (6–8 weeks) are required to improve functional capacity. IMT associated with other interventions only showed an increase in PImax (8.44 cm H2O; 95% CI 4.98–11.91), and the presence of inspiratory muscle weakness did not change this result.
CONCLUSIONS: Isolated IMT improved inspiratory muscle strength, functional capacity, and pulmonary function, without changing dyspnea and quality of life. Associated IMT only increased inspiratory muscle strength. These results indicate that isolated IMT can be considered as an adjuvant intervention in patients with COPD.
Introduction
COPD is one of the major causes of chronic morbidity and mortality worldwide.1 Prognosis of patients with COPD is influenced by the severity and recurrence of exacerbation, with yearly mortality rates of 11% for patients who need hospitalization, 5–50% for patients on mechanical ventilation, and rising as high as 37% in case of hospitalization for exacerbation recurrence.2 Strategies are required that aim to reduce the disease progression and thus improve patients’ prognosis as well as reduce costs of health care and the global and socioeconomic burden of the disease.3
Individuals with COPD present with limitations in exercise capacity due to multiple factors, including ventilation, gas exchange, cardiovascular disease,4 and abnormalities in peripheral muscles.5 Inspiratory muscle dysfunction also occurs in these patients and is associated with dyspnea and reduced exercise capacity.6,7 Thus, pulmonary rehabilitation is recommended as an efficient intervention in cardiorespiratory management, generating improvements in exercise performance, with reductions in dyspnea in patients with different degrees of disease severity.8 As a pulmonary rehabilitation strategy, inspiratory muscle training (IMT) optimizes lung capacity and, consequently, improves physical conditioning.9
Gosselink et al10 conducted a systematic review with meta-analysis, including 32 randomized controlled trials (RCTs) on IMT effects in subjects with COPD. The authors made general and subgroup analyses with regard to training modality (strength of resistance and if pulmonary rehabilitation was added) and subject characteristics. The authors concluded that IMT improves inspiratory muscle strength, functional capacity, dyspnea, and quality of life. In subjects with inspiratory muscle weakness, inclusion of IMT in pulmonary rehabilitation programs improved inspiratory muscle strength and tended to improve exercise performance.10
Recently, Beaumont et al11 published a new systematic review on the subject. The authors reviewed 43 studies (37 meta-analyses), including RCTs, nonrandomized controlled trials, and observational studies published until 2017, and they noted the effects of IMT when isolated or associated with pulmonary rehabilitation, considering the presence of respiratory muscle weakness. They observed that IMT improved inspiratory muscle strength, quality of life, exercise capacity, and dyspnea, although there was no additional effect on pulmonary rehabilitation. According to the authors, the presence of respiratory muscle weakness seemed not to affect results, although they suggest further investigations of this intervention regarding dyspnea and quality of life.
Based on the results reported by Gosselink et al10 and Beaumont et al,11 a new systematic review including only RCTs and approaching important clinical issues for this type of training and this type of population is necessary. This systematic review will assess IMT effects on respiratory muscle strength, pulmonary function, dyspnea, functional capacity, and quality of life in patients with COPD, considering 4 factors: (1) IMT isolated or associated to other interventions; (2) the presence of inspiratory muscle weakness; (3) training load; and (4) intervention time.
Methods
This systematic review and meta-analysis followed recommendations proposed by the Cochrane Collaboration12 and the PRISMA Statement.13 The study protocol was registered in PROSPERO (CRD42017080337).
Eligibility Criteria
We included RCTs that assessed the effect of IMT, whether isolated or associated with other interventions, that compared treated subjects with a control group (ie, no intervention), placebo, or other intervention (eg, pulmonary rehabilitation, exercise, breathing exercises, or usual care); subject criteria included a diagnosis of COPD by spirometry, consistent with the GOLD criteria (FEV1/FVC < 70%), during both exacerbation and out-patient clinic care. The following outcomes were considered: respiratory muscle strength, pulmonary function, functional capacity, dyspnea, and quality of life. Studies with incomplete data or lacking data description were excluded.
Search Strategy
We searched the following electronic databases: MEDLINE (accessed via PubMed), EMBASE, Cochrane CENTRAL, PEDro, and LILACS. A manual search was also conducted in references of studies already published on the subject. The research terms used individually or combined include “pulmonary disease, chronic obstructive” (MeSH and entry terms) and “breathing exercises” (MeSH and entry terms) associated with a list of sensitive terms for searches of RCTs as prepared by Robinson and Dickersin.14 There were no restrictions as to year and language. The search occurred in June 2018. The full search strategy used for PubMed can be seen in supplementary materials at http://www.rcjournal.com.
Selection of Studies and Data Extraction
The titles and abstracts of all papers identified with the search strategy were independently assessed by 2 reviewers with a checklist containing inclusion and exclusion criteria. Studies that did not meet the eligibility criteria were excluded, and those that met the criteria or raised questions were selected for assessment of the whole text. The same independent reviewers assessed and selected these articles. Disagreements between reviewers were resolved by consensus. When the studies did not present the data required for meta-analysis, the corresponding author was contacted. In cases when the data were not available, the paper was excluded from the study. Data were extracted through a standardized form containing information on the methodological characteristics of the studies, subjects, interventions, and outcomes. The outcomes extracted were: respiratory muscle strength (ie, maximum inspiratory pressure [PImax] and maximum expiratory pressure), pulmonary function, (FVC, vital capacity, and FEV1), functional capacity (ie, distance walked in the 6-min-walk test [6MWT] and maximum oxygen consumption [ ]), dyspnea (Borg scale), and quality of life (St George Respiratory Questionnaire score).
]), dyspnea (Borg scale), and quality of life (St George Respiratory Questionnaire score).
Risk of Bias Assessment
The risk of bias was assessed independently by 2 reviewers using the Cochrane Collaboration tool, considering the following characteristics for all included studies: generation of appropriate sequence, allocation concealment, patient and therapist blinding, description of losses and exclusions, and analysis of intention to treat. Studies without clear descriptions of these items were considered not clear or not informed.
Data Analysis
The meta-analysis was conducted using the random-effects model, and the effect size used was the mean difference, determined by the difference between the means at the baseline moment and at the end of the study for each group. These data were expressed as weighted mean differences among groups and standard deviation of the difference.13 A 95% CI was considered statistically significant. Statistical homogeneity across studies was assessed using the inconsistency test (I2), where values > 25% and > 50% were considered to indicate moderate and high heterogeneity, respectively.15 All analyses were made using Review Manager 5.3 (Cochrane Collaboration) and Stata 14 (StataCorp, College Station, Texas). Heterogeneity across studies was explored with 2 strategies: (1) executing the meta-analysis again, removing 1 paper at a time to check whether any individual study explained heterogeneity; (2) sensitivity analyses to assess sub-groups of studies with higher probability of producing valid intervention estimates, based on relevant prespecified clinical information that influence IMT effects on results (eg, association of interventions with IMT, intervention duration, inspiratory load, and whether the studies included patients with inspiratory muscle weakness, denoted as PImax < 60 cm H2O). In addition, meta-regression analyses were performed for outcome with high number of studies included (ie, PImax and 6MWT) and including main covariates (ie, inspiratory load, intervention duration, and weakness).
Summary of Evidence: GRADE Criteria
The quality of the evidence was assessed using the GRADE approach, as recommended by the Cochrane Handbook for Systematic Reviews of Interventions (Internet tool available at https://gradepro.org).12 For each outcome, the quality of the evidence was based on 5 factors: risk of bias; inconsistency; indirectness; imprecision; and potential for publishing bias. Quality was reduced by one level for each factor not met. The GRADE approach resulted in 4 levels of evidence quality: high, moderate, low, and very low.16
Results
Description of the Studies
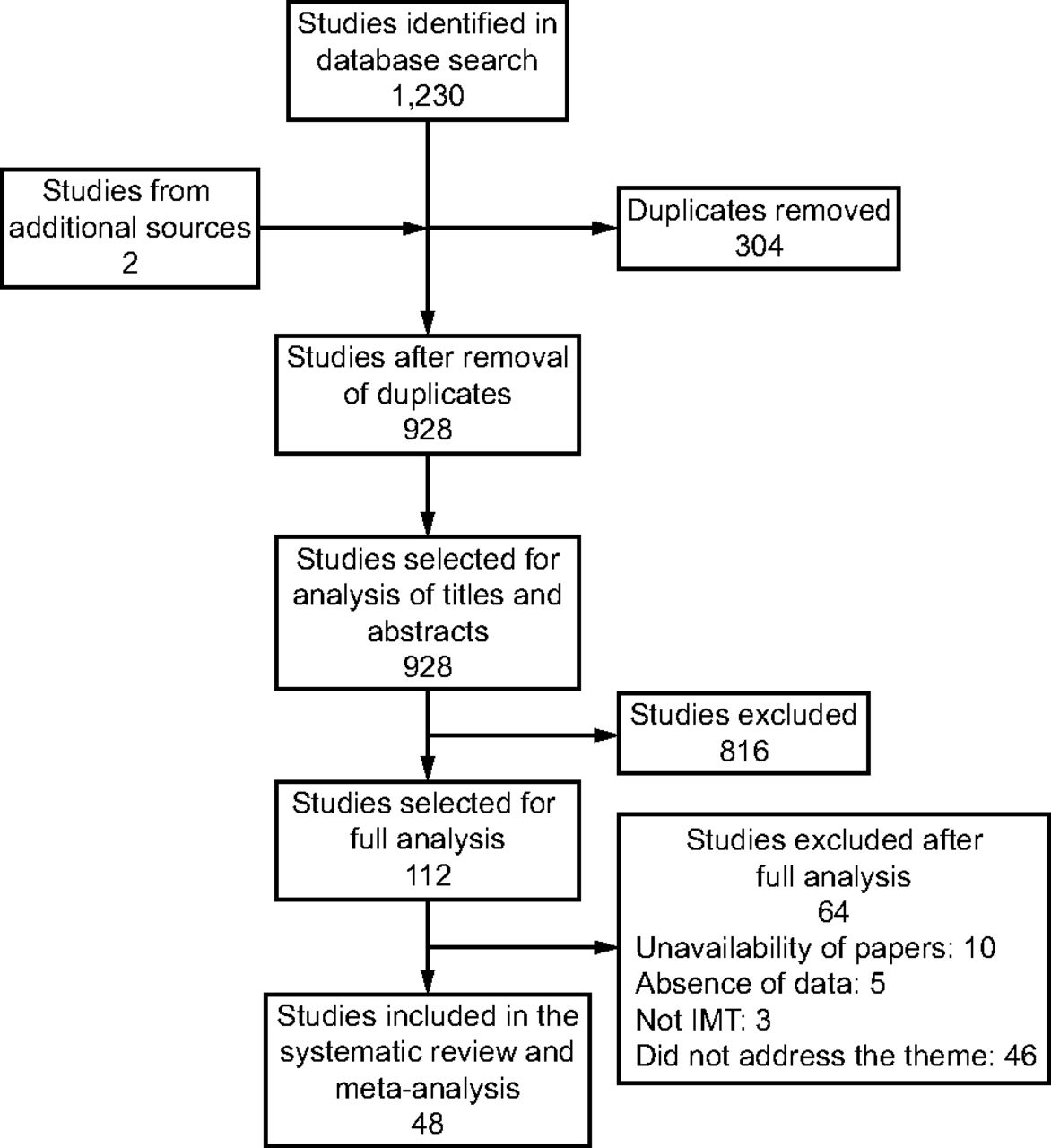
The search strategy resulted in 1,230 abstracts, of which 112 were considered potentially relevant and were selected for detailed analysis. A total of 48 studies met the eligibility criteria and were included in the systematic review and in the meta-analysis (N = 1,996 subjects) (Fig. 1); 39 studies (n = 943 subjects) only assessed isolated IMT.17-55 Of these, 25 studies (n = 631 subjects) included subjects with respiratory muscle weakness.17-19,22-28,31-34,37,38,40,41,43,45-49,52 Various loads for IMT were 15% of PImax,42,46,48 30% of PImax,17,28,31,33,38,40,43,51 load progression of 5–35% of PImax,23,24 load progression up to 40–50% of PImax,21,39,53 load progression up to 60% of PImax,18,20,22,24-28,30,34,37,45,47,49,50,52,54-56 70% of PImax,44 and 80% of PImax.36 Belman et al19 and Oh35 used PFLEX equipment, and the load used for IMT was not clear. Leelarungrayub et al32 used Portex equipment, and load/resistance was set by the tube diameter (ie, 6 mm, 4 mm, and 2 mm) (can be seen in supplementary materials at http://www.rcjournal.com).

Flow chart. IMT = inspiratory muscle training.
Nine studies (n = 965 subjects) assessed IMT in association with some other type of intervention.57-65 These other interventions were pulmonary rehabilitation,58,62,64,65 resis-tance/aerobic training with cycle ergometer,59-61,63 or conventional physical therapy.57 In 4 studies (n = 153 subjects), the associated IMT was conducted in subjects with respiratory muscle weakness.57,58,60,63 The loads used for IMT associated with other interventions varied: 30% of PImax,59,63 30–60% of PImax,61,62,64,65 70% of PImax,58,60 and 60–80% of PImax.57 For isolated IMT, most studies used IMT with low or no load, and the control group was IMT placebo. For studies that assessed IMT in association with another intervention, most studies used low-load IMT or pulmonary rehabilitation as control groups (can be seen in supplementary materials at http://www.rcjournal.com).
Risk of Bias
Of the studies included in this systematic review, 15.2% reported allocation concealment, 17.4% reported blinding of therapists, and 30.4% used the principle of intention to treat for statistical analyses, characterizing a high risk of bias for these items. Still, 34.8% used patient blinding, and 39.1% used blinding for outcome appraisers, which carry moderate bias risk. Finally, 80.4% of the included studies described losses in follow-up and exclusions, and 65.2% reported randomization in subject assignment, which carry moderate risk of bias (see the supplementary materials at http://www.rcjournal.com).
Effects of Interventions
Maximum Inspiratory Pressure.
Of the 39 papers included that conducted isolated IMT, 36 studies17-27,29-34,36-41,43-55 assessed PImax (n = 889 subjects). Significant improvement occurred in PImax when IMT was compared to the control groups (10.64 cm H2O, 95% CI 7.61–13.66, I2: 46%) (Fig. 2). Based on the GRADE approach, the quality of evidence for this result was considered low due to methodological limitations, imprecision, and inconsistency of results (Table 1). Considering the 24 studies that only included subjects with inspiratory muscle weakness,17-19,22-27,31-34,37,38,40,41,43,45-49,52 there was significant improvement for this outcome (9.60 cm H2O, 95% CI 5.74–13.46, I2: 40%). In addition, considering studies that included subjects without respira-tory muscle weakness,20,21,29,30,36,39,44,50,51,53-55 significant improvement was also observed for this outcome (13.61 cm H2O, 95% CI 12.45–14.78, I2: 0%). The assessment of studies that used up to 35% of PImax training loads showed improvement in this outcome (8.30 cm H2O, 95% CI 1.38–15.21, I2: 0%); the same behavior was observed for loads between 40% and 50% (11.20 cm H2O, 95% CI 5.86–16.54, I2: 0%), and a slightly superior gain was observed for loads between 60% to 80% of PImax (10.99 cm H2O, 95% CI 6.65–15.33, I2: 68%). Gains observed with shorter intervention times were equivalent to gains obtained with longer interventions: ≤ 4 weeks (11.62 cm H2O, 95% CI 5.32–17.91, I2: 0%); 6–8 weeks (11.69 cm H2O, 95% CI 8.14–15.25, I2: 39%); 16 weeks (15.75 cm H2O, 95% CI 5.03–26.47, I2: 0%); and no difference was observed for 10 weeks and 12 weeks (8.84 cm H2O, 95% CI −0.71 to 18.39, I2: 66%). When included in meta-regression, these covariates were not significantly associated with the heterogeneity observed through the studies (data not shown).

A: PImax for treatment with isolated IMT against control group. PImax = maximum inspiratory pressure; IMT = inspiratory muscle training.
Quality of Evidence
In the analysis of studies that assessed IMT associated with other interventions, we identified 8 papers57-60,62-65 that assessed PImax (n = 985 subjects), and significant improvement was observed in this outcome (8.44 cm H2O, 95% CI 4.98–11.91, I2: 0%) (Fig. 3). The quality of evidence was considered moderate based on methodology limitations, imprecision, and inconsistency of results (Table 1). Considering the 4 studies that only included subjects with inspiratory muscle weakness57,58,60,63 (8.44 cm H2O, 95% CI 0.60–16.28, I2: 0%) and studies including subjects without respiratory muscle weakness (8.46 cm H2O, 95% CI 4.58–12.34, I2: 0%), there was significant improvement in both situations. Studies that used IMT loads between 60% and 80% of PImax obtained significant improvement (10.08 cm H2O, 95% CI 1.05–19.11, I2: 0%). Significant improvement in PImax was also observed in studies with interventions that lasted 3–4 weeks (8.51 cm H2O, 95% CI 4.59–12.42, I2: 0%) and 10–12 weeks (10.97 cm H2O, 95% CI 0.95–20.99, I2: 0%).

PImax for treatment with associated IMT against control group. PImax = maximum inspiratory pressure; IMT = inspiratory muscle training.
FVC.
We identified 10 studies18,19,24,26,32,33,39,52,53,55 that conducted isolated IMT and assessed FVC, and no significant improvement was observed (−0.28, 95% CI −0.62 to 0.07, I2: 85%) (see the supplementary materials at http://www.rcjournal.com). Based on the GRADE approach, the quality of evidence for this result was very low due to methodology limitations and inconsistency of results (Table 1). No change in this result was found for the 6 studies that only included patients with inspiratory muscle weakness18,19,26,32,33,52 (−0.10, 95% CI −0.42 to 0.23, I2: 42%), and the same occurred for subjects without respiratory weakness (−0.62, 95% CI −2.01 to 0.77, I2: 94%). In the analysis of IMT loads up to 35% of PImax (−0.04, 95% CI −0.92 to 0.84, I2: 0%) and intervention durations of 4–5 weeks (−1.22, 95% CI −6.17 to 3.72, I2: 0%) and 6–8 weeks (−0.30, 95% CI −0.68 to 0.07, I2: 90%), no significant difference was observed between IMT and controls.
FEV1.
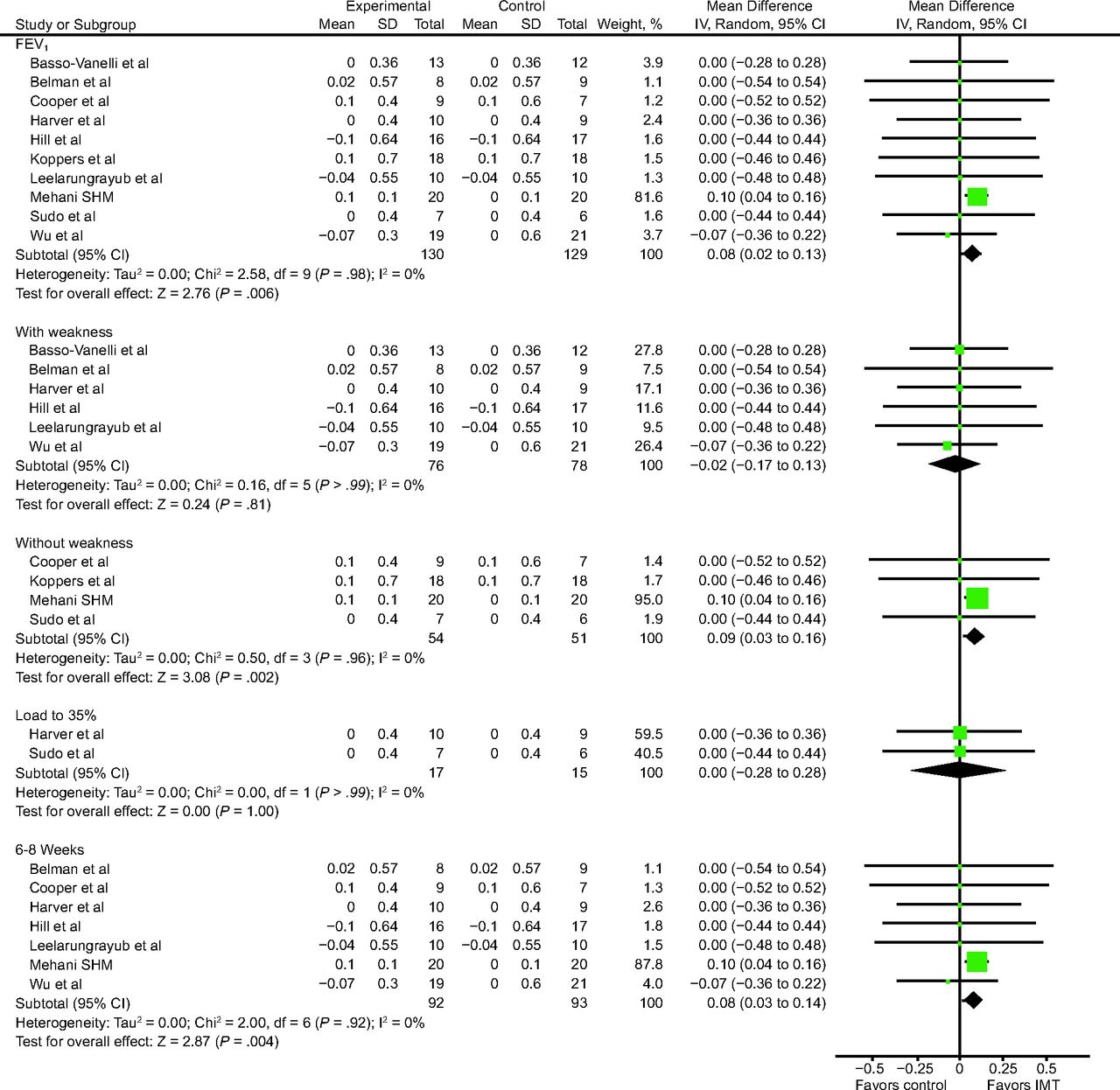
We identified 10 studies18,19,24,26,29,32,42,52,53,55 that conducted isolated IMT and assessed FEV1 (n = 259 subjects). The comparison between IMT and control groups revealed an improvement in FEV1 (0.08, 95% CI 0.02–0.13, I2: 0%) (Fig. 4). Based on the GRADE approach, the quality of evidence for this result was moderate due to methodology limitations and inconsistency of results (Table 1). For the 6 studies that only included subjects with inspiratory muscle weakness,18,19,24,26,32,52 there was no significant difference (−0.02, 95% CI −0.17 to 0.13, I2: 0%). However, in the analysis of subjects without muscle weakness, there was improvement of this outcome (0.09, 95% CI 0.03–0.16, I2: 0%). No improvement of this outcome was found in the analysis of IMT loads up to 35% of PImax (0.00, 95% CI −0.28 to 0.28, I2: 0%), and improvement occurred according to intervention duration of 6–8 weeks (0.08, 95% CI 0.03–0.14, I2: 0%).

FEV1 for treatment with isolated IMT against control group. IMT = inspiratory muscle training.
Vital Capacity.
Three studies29,33,42 that analyzed isolated IMT and assessed vital capacity (n = 73), and no improvement was observed compared to the control groups (−0.08, 95% CI −0.81 to 0.64, I2: 0%). Based on the GRADE approach, the quality of evidence for this result was low due to methodology limitations and inconsistency of results (Table 1).
Distance Walked in 6MWT.
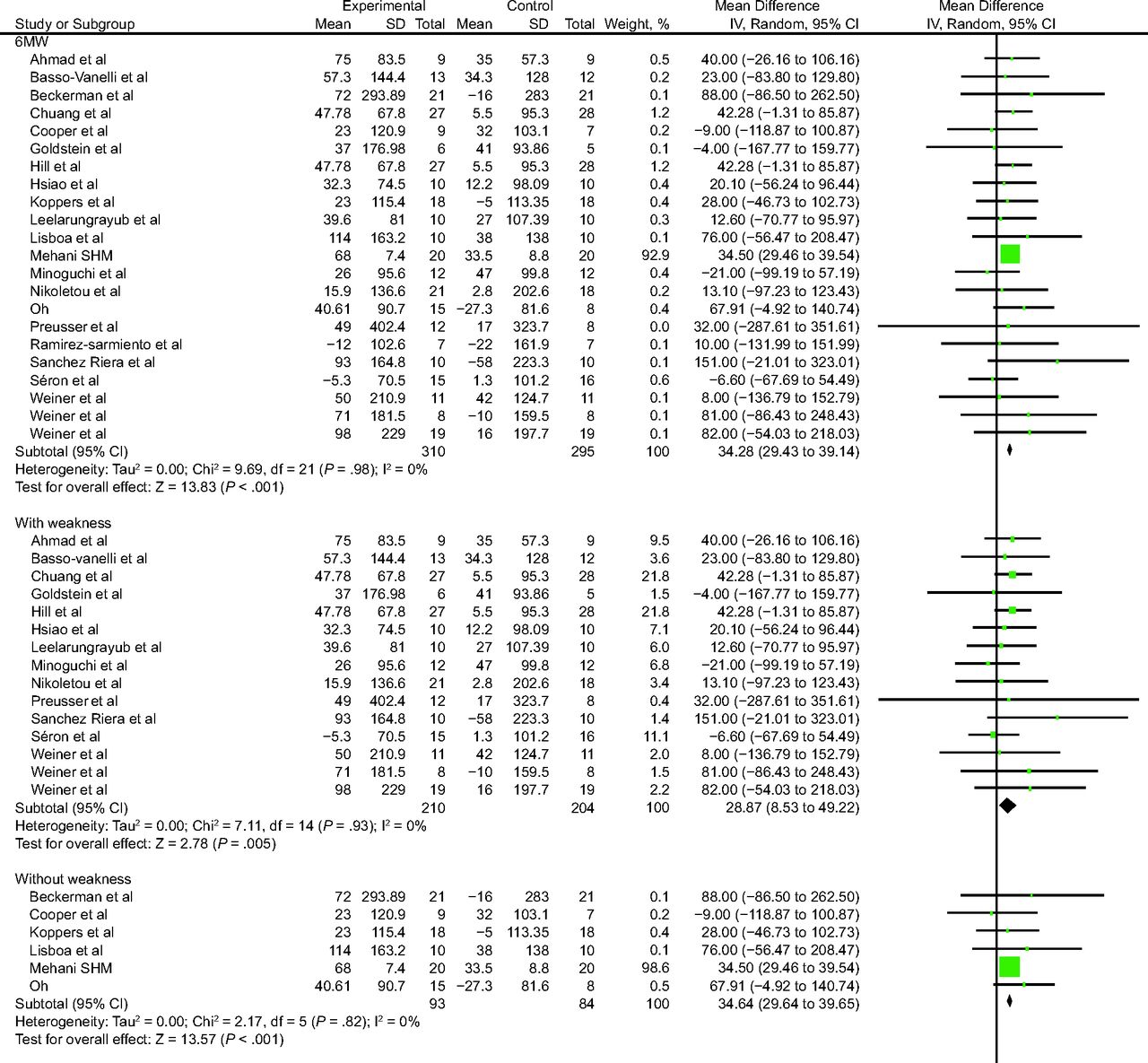
We identified 22 studies17,18,20,22,23,26,27,29,32-35,37,39-41,46-48,51,53,55 that analyzed isolated IMT and assessed distance walked in 6MWT (n = 605 subjects) with significant improvement (34.28 m, 95% CI 29.43–39.14, I2: 0%) (Fig. 5). Based on the GRADE approach, the quality of evidence for this result was low due to methodology limitations and inconsistency of results (Table 1).

6MWT for treatment with isolated IMT against control group. IMT = inspiratory muscle training; 6MWT = 6-min-walk test.
There was significant improvement for this outcome in the 15 studies that only included subjects with inspiratory muscle weakness17,18,22,23,26,27,32-34,37,40,41,46-48 (28.87 m, 95% CI 8.53–49.22, I2: 0%), and the increase was higher in subjects without respiratory muscle weakness (34.64 m, 95% CI 29.64–39.65 I2: 0%). When IMT loads of 40–50% of PImax were analyzed, there was no significant improvement (21.94 m, 95% CI −10.74 to 54.62, I2: 0%); however, this outcome showed improvement in IMT loads superior to 60–80% (34.72 m, 95% CI 29.72–39.73, I2: 0%). In relation to intervention duration, no improvement was observed for this outcome in studies that carried out the intervention for 4 weeks (20.76 m, 95% CI 12.24 to 53.77, I2: 0%), and the same occurred for interventions that lasted 10–12 weeks (59.05 m, 95% CI 14.88 to 132.97, I2: 0%. The results were different for interventions of 6–8 weeks, which showed significant improvement (34.46 m, 95% CI 29.54–39.38, I2: 0%). In meta-regression analyses, no tested covariates were able to explain the heterogeneity observed (data not shown).
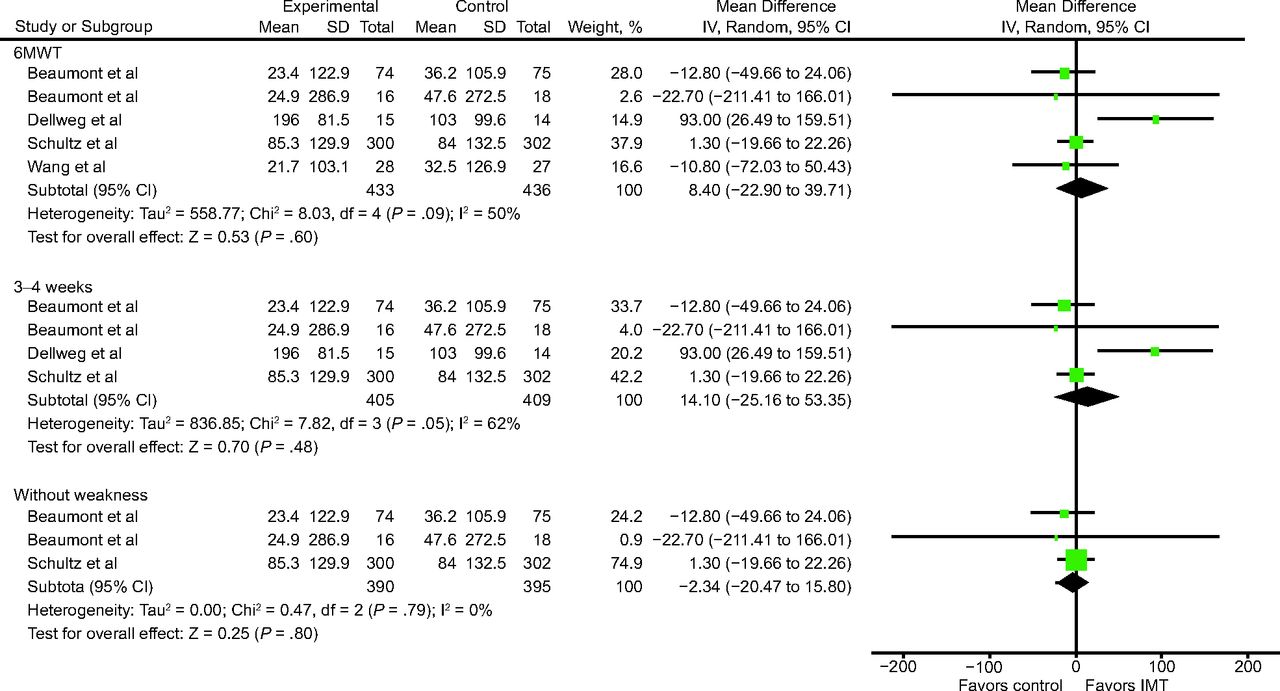
While analyzing studies that performed IMT associated with other interventions, 5 studies57,62-65 assessed 6MWT(n = 869 subjects), and no significant difference was observed for this outcome (8.40 m, 95% CI −22.90 to 39.71, I2: 50%) (Fig. 6). Based on GRADE, quality of evidence for this outcome was considered moderate due to methodology limitations, imprecision and inconsistency of results (Table 1). No improvement was observed for this outcome in studies that carried out the intervention for 3 to 4 weeks (14.10 m [95% CI: −25.16 to 53.35; I2: 62%]). In sensitivity analysis of studies that included subjects without inspiratory muscle weakness,62,64,65 significant improvement was observed in 6MWT in favor of the control group when compared to IMT (−2,34 m [95% CI: −20.47 to 15.80; I2: 0%]).
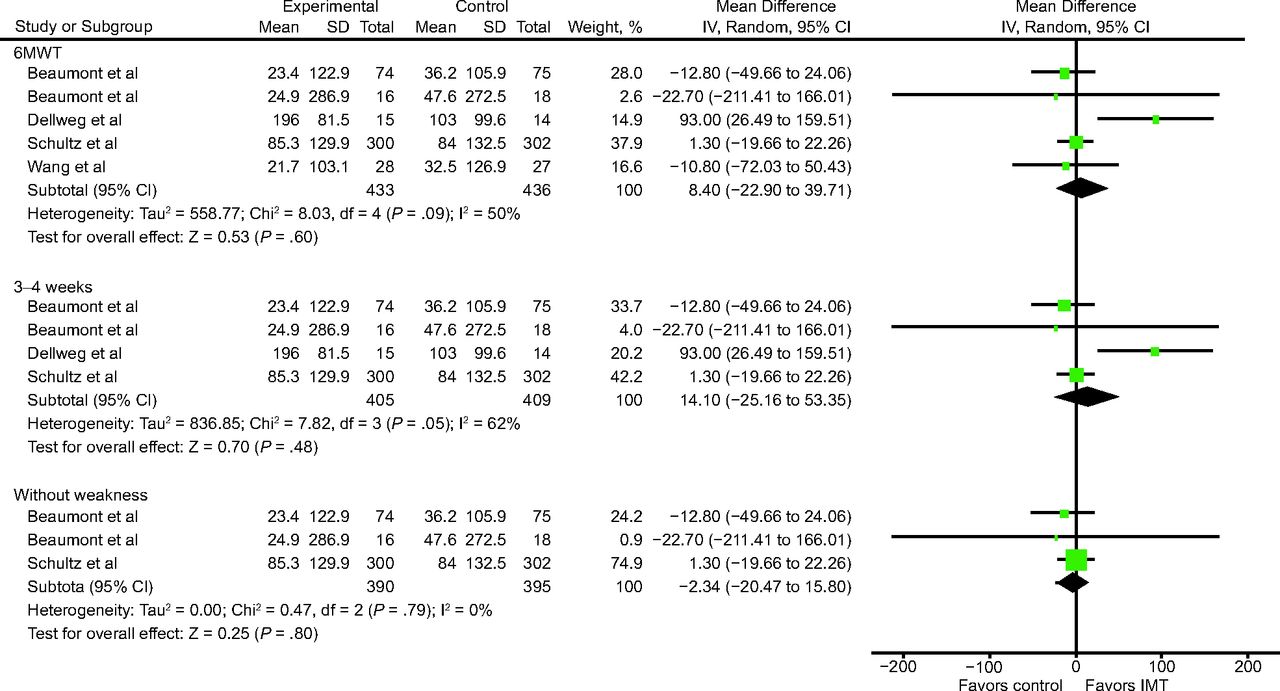
6MWT for treatment with associated IMT against control group. IMT = inspiratory muscle training; 6MWT = 6-min-walk test.
Maximum Oxygen Consumption.
Three studies36,40,44 that analyzed isolated IMT assessed maximum oxygen consumption ( ) (n = 82 subjects), and no difference was observed for this outcome (0.12 mL/kg/min, 95% CI −0.14 to 0.39, I2 0%). Based on the GRADE approach, the quality of evidence for this result was considered very low due to methodology limitations and inconsistency of results (Table 1). In 3 studies58-60 that conducted IMT associated with other intervention and assessed
) (n = 82 subjects), and no difference was observed for this outcome (0.12 mL/kg/min, 95% CI −0.14 to 0.39, I2 0%). Based on the GRADE approach, the quality of evidence for this result was considered very low due to methodology limitations and inconsistency of results (Table 1). In 3 studies58-60 that conducted IMT associated with other intervention and assessed  (n = 96 subjects), no difference was observed (−0.02 mL/kg/min, 95% CI −0.22 to 0.19, I2: 0%). All studies included subjects that had respiratory muscle weakness. Based on the GRADE approach, the quality of evidence for this result was considered low due to methodology limitations and inconsistency of results (Table 1).
(n = 96 subjects), no difference was observed (−0.02 mL/kg/min, 95% CI −0.22 to 0.19, I2: 0%). All studies included subjects that had respiratory muscle weakness. Based on the GRADE approach, the quality of evidence for this result was considered low due to methodology limitations and inconsistency of results (Table 1).
Dyspnea.
We identified 12 studies29,30,32,33,35,36,40,41,46-48,51 that conducted isolated IMT and assessed dyspnea with the Borg scale (n = 280 subjects), and no significant difference was observed (−0.37, 95% CI −1.21 to 0.47, I2: 58%) (see the supplementary materials at http://www.rcjournal.com). Based on the GRADE approach, the quality of evidence for this result was considered very low due to methodology limitations and inconsistency of results (Table 1). The studies that only assessed subjects with inspiratory muscle weakness32,33,40,46-48 reported significant improvement for this outcome and an absence of heterogeneity (0.59, 95% CI −0.00 to 1.18, I2: 0%). For subjects without respiratory muscle weakness, no improvement was observed for this outcome (−1.27, 95% CI −2.67 to 0.12, I2: 69%)]. The analysis of studies with IMT loads of 40–50% (0.45, 95% CI −0.36 to 1.26, I2: 38%) and 60–80% (0.18, 95% CI −0.93 to 1.29, I2: 0%) showed no significant improvement for this outcome. Studies with intervention durations of 4 weeks (−0.83, 95% CI −1.88 to 0.22, I2: 20%) and 6–8 weeks (−0.26, 95% CI −1.29 to 0.76, I2: 67%) reported no significant improvement.
Quality of Life.
We identified 2 studies17,20 that conducted isolated IMT and assessed quality of life (n = 60 subjects) with loads of 60–80%, and no significant difference was observed for this outcome (18.85, 95% CI −8.00 to 45.70, I2: 0%) (see the supplementary materials at http://www.rcjournal.com). Based on the GRADE approach, the quality of evidence for this result was considered very low due to methodology limitations and inconsistency of results (Table 1).
Discussion
Summary of Evidence
This systematic review and meta-analysis indicates that isolated IMT improves inspiratory muscle strength, functional capacity, and pulmonary function, without difference in dyspnea and quality of life. IMT associated with other interventions, on the other hand, presented increases only in inspiratory muscle strength.
Significant improvement in the distance walked in the 6MWT was observed only for isolated IMT; in subjects without respiratory muscle weakness, the increase was higher. In addition, this improvement can be considered to be a clinically relevant difference for patients with COPD, for whom one of the major limitations is functional capacity.
With regard to  , dyspnea, and quality of life, there was no significant difference. Moreover, gains were higher in studies that included subjects with inspiratory muscle weakness, conducted IMT for ≥ 8 weeks, and had control groups that received placebo IMT without load40 or with very low inspiratory load.20,24-27,30,31,35-37,41-43,46-49,60,61 This may be due to the higher level of deficiency in subjects included, longer duration of intervention, and the comparison of an IMT group with a control group that received placebo IMT without inspiratory load. Two studies indicated that dyspnea and distance walked on the 6MWT are inversely proportional, which probably correlates with improvement in exercise capacity.66,67
, dyspnea, and quality of life, there was no significant difference. Moreover, gains were higher in studies that included subjects with inspiratory muscle weakness, conducted IMT for ≥ 8 weeks, and had control groups that received placebo IMT without load40 or with very low inspiratory load.20,24-27,30,31,35-37,41-43,46-49,60,61 This may be due to the higher level of deficiency in subjects included, longer duration of intervention, and the comparison of an IMT group with a control group that received placebo IMT without inspiratory load. Two studies indicated that dyspnea and distance walked on the 6MWT are inversely proportional, which probably correlates with improvement in exercise capacity.66,67
This meta-analysis observed divergent results for functional capacity. We noted a significant increase in distance walked in the 6MWT (with isolated IMT), which did not occur for maximum  . This result may be explained by the fact that maximum and submaximum tests have different physiological determinants and the potential for postintervention improvement.68 Moreover, in the maximum
. This result may be explained by the fact that maximum and submaximum tests have different physiological determinants and the potential for postintervention improvement.68 Moreover, in the maximum  analysis, there was a small number of subjects and, according to the GRADE approach, the quality of evidence for this result was considered very low due to methodology limitations, imprecision, and inconsistency of results.
analysis, there was a small number of subjects and, according to the GRADE approach, the quality of evidence for this result was considered very low due to methodology limitations, imprecision, and inconsistency of results.
We also observed that IMT significantly improved PImax compared to control groups. Several studies noted that PImax is reduced in subjects with COPD,10 and that IMT has a beneficial effect on this outcome.17,18,32,57 Improvement in inspiratory muscle function may have reached respiratory discharge with restoration of unbalance between inspiratory muscles capacity to sustain the activity and inspiratory loads. There is evidence that respiratory muscle weakness, observed in subjects with COPD, is improved. Moreover, this variable is directly correlated to  , which suggests that respiratory muscle weakness contributes to the deficit in exercise capacity under COPD.69
, which suggests that respiratory muscle weakness contributes to the deficit in exercise capacity under COPD.69
Another important aspect concerns the loads analyzed in these studies, which ranged from 30% to 60% of PImax. In the study by Basso-Vanelli et al,18 which started IMT with initial load of 10 cm H2O and progressed to 60% of PImax after intervention, there was significant improvement in both groups with regard to respiratory muscle resistance and strength, thoracic-abdominal mobility and distance walked in the 6MWT. There was also reduction of dyspnea at 6MWT peak.
Corroborating the above mentioned results, Beckerman et al20 observed, while using IMT load of 15–60% of PImax, statistically significant increases in inspiratory muscle strength and distance walked in the 6MWT by the end of the third month of training and reduction of dyspnea by the end of 9 months of training in the intervention group, but these increases were not seen in the control group. By the end of one year of training, these changes were maintained.
Strengths and Limitations
This meta-analysis of RCTs was conducted to quantitatively express the results and to assess the quality of evidence for each outcome analyzed. We noted that the RCTs included were methodologically limited because none of them presented in full the items observed in the bias risk assessment. Another limitation is that few studies evaluated IMT for an intervention time > 10 weeks, making it difficult to discuss our results and reinforcing the need for further studies evaluating the effect of IMT in the long term. Nevertheless, there were reasonably large numbers of studies and subjects, which makes our study relevant.
According to the GRADE approach, all results, except for FEV1 outcome (IMT isolated), PImax, and 6MWT (IMT associated), which were considered moderate, presented low or very low quality of evidence. This indicates that any estimate of effect is very uncertain, and it is likely that new research will improve the confidence to estimate the effect.
Comparisons with Other Reviews
Gosselink et al10 performed a systematic review on this subject. However, this work included 32 RCTs that used IMT in subjects with COPD, whereas the present review included 46 papers that used IMT in subjects with COPD. Additionally, Gosselink et al10 limited their search for papers in English, whereas the current review did not have language limitations. Moreover, the meta-analyses analyzed here considered the type of device used, dyspnea outcome with the Borg scale, exercise capacity with the 6MWT, and quality of life with the St George Respiratory Questionnaire for subjects with COPD, which Gosselink et al10 did not do. For these reasons, some studies included in in the meta-analysis by Gosselink et al10 were excluded from our review because they did not meet our eligibility criteria or presented incomplete data, which hampered statistical analyses.
The systematic review carried out by Beaumont et al,11 which verified IMT effects in subjects with COPD regarding dyspnea, quality of life, exercise capacity, and inspiratory muscle strength, included 43 studies, with 37 meta-analyses, but the search was limited to studies in English and French. The number of studies included was similar to that of this review, although Beaumont et al11 included nonrandomized controlled trials and cohort studies in addition to RCTs, which may compromise the quality of the evidence. Our review generates a higher level of evidence against already existing evidence.
We observed that all of above-mentioned reviews assessed PImax and functional capacity with the 6MWT, with positive results for these outcomes, which corroborate our review. Our review assessed outcomes associated to with pulmonary function (ie, FVC, FEV1, maximum  , and vital capacity), and the results are inconclusive because we found differences only for FEV1. Quality of life showed positive results as assessed in both previous reviews10,11; this differs from our results, which did not present significant improvement for this outcome. Both previous reviews10,11 assessed dyspnea and found positive results; however, we noted dyspnea improvement only in studies of subjects with inspiratory muscle weakness, showing significant improvement for this outcome and absence of heterogeneity. For most outcomes presented in this review, the evidence level is still low or very low, which indicates the need for more studies on the subject.
, and vital capacity), and the results are inconclusive because we found differences only for FEV1. Quality of life showed positive results as assessed in both previous reviews10,11; this differs from our results, which did not present significant improvement for this outcome. Both previous reviews10,11 assessed dyspnea and found positive results; however, we noted dyspnea improvement only in studies of subjects with inspiratory muscle weakness, showing significant improvement for this outcome and absence of heterogeneity. For most outcomes presented in this review, the evidence level is still low or very low, which indicates the need for more studies on the subject.
Conclusions
Isolated IMT is an effective treatment modality to improve inspiratory muscle strength, functional capacity, and pulmonary function in patients with COPD, without changes in dyspnea and quality of life. The presence of inspiratory muscle weakness did not change the results. Higher loads promoted a greater improvement of these outcomes. Shorter intervention times increased inspiratory muscle strength, but longer intervention times were required to increase functional capacity. Associated IMT only showed increases in inspiratory muscle strength. This analysis indicates that isolated IMT can be considered as an adjuvant intervention in patients with COPD.
Footnotes
- Correspondence: Graciele Sbruzzi PT ScD, Rua Felizardo, n° 750, Jardim Botânico, Porto Alegre 90690200, Brazil. E-mail: graciele.sbruzzi{at}ufrgs.br
Ms Figueiredo presented a version of this paper at the Universidade Federal do Rio Grande do Sul, in November 2018, in Porto Alegre, Brazil.
This study was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}