Article Text

Abstract
Tracheobronchial foreign body aspiration is a serious medical problem, with clinical manifestations ranging from acute asphyxiation to insidious lung damage, as demonstrated by the three presented cases. Patient 1 aspirated during dinner, emergency bronchoscopy retrieved pieces of food, and she fully recovered the following day. Patient 2 presented with recurrent pneumonia and a right lower lobe lung abscess. After right lower lobectomy, pathology revealed a foreign object in the right main stem bronchus, a peanut aspirated one year earlier. Patient 3 became unresponsive several days after spinal surgery. The differential diagnosis included myocardial infarction, stroke, and foreign body aspiration. The patient died and necropsy revealed a foreign body in the right main stem bronchus (cooked meat). Thus, foreign body aspiration is not always suspected clinically, and the pathologist may play an important role in making the diagnosis. Histological identification of the aspirated material may be necessary for definitive diagnosis. Therefore, sections of commonly aspirated foods are presented, together with a 10 year history of aspirated objects received by this institution’s surgical pathology department.
- aspiration pneumonia
- bronchial obstruction
- foreign body aspiration
Statistics from Altmetric.com
Tracheobronchial foreign body aspiration is an important problem in the USA, being responsible for 17 537 visits to emergency departments by children under 14 in 2001, and 160 deaths in this age group.1 Clinical presentation in both children and adults may range from acute life threatening asphyxiation to recurrent infection with insidious lung damage.2,3,4 Often, there is no clear history of aspiration and the material retrieved from the airways is not readily recognised as foreign.5 The following cases demonstrate three common presentations and outcomes of foreign body aspiration, and exemplify the role of the pathologist in diagnosis.
“Often, there is no clear history of aspiration and the material retrieved from the airways is not readily recognised as foreign”
CASE 1
A 93 year old woman with dementia became cyanotic and apneic during dinner at her nursing home residence. The Heimlich manoeuvre was performed and suctioning of the oral pharynx retrieved the aspirated material, which was recognised as two pieces of chicken. The patient had continued respiratory distress and was immediately brought to the emergency department, where her oxygen saturation was 93% on 10 litres/minute of oxygen by nasal canula. A chest radiograph showed a collapsed left lower lobe, and emergency bronchoscopy removed two pieces of “food stuff” from the left main stem bronchus. She promptly recovered and was discharged two days later, with a swallowing study recommended as an outpatient. Two tan/white, firm, irregular shaped soft tissues were received in surgical pathology. Microscopically, sections showed degenerated skeletal muscle admixed with adipose tissue (fig 1). Given the clinical scenario, the gross and microscopic appearances of the specimen were felt to be consistent with the aspiration of chicken.

Retrieved bronchial specimen (chicken) in patient 1. Note the degenerated muscle fibres with lack of prominent cross striations and nuclei (haematoxylin and eosin stained).
CASE 2
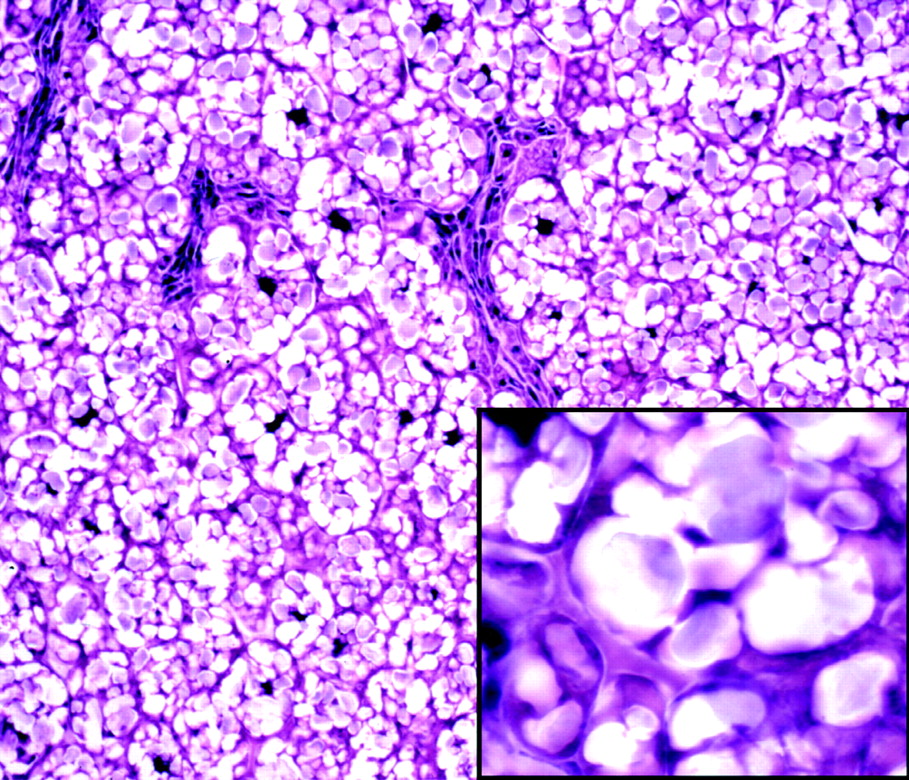
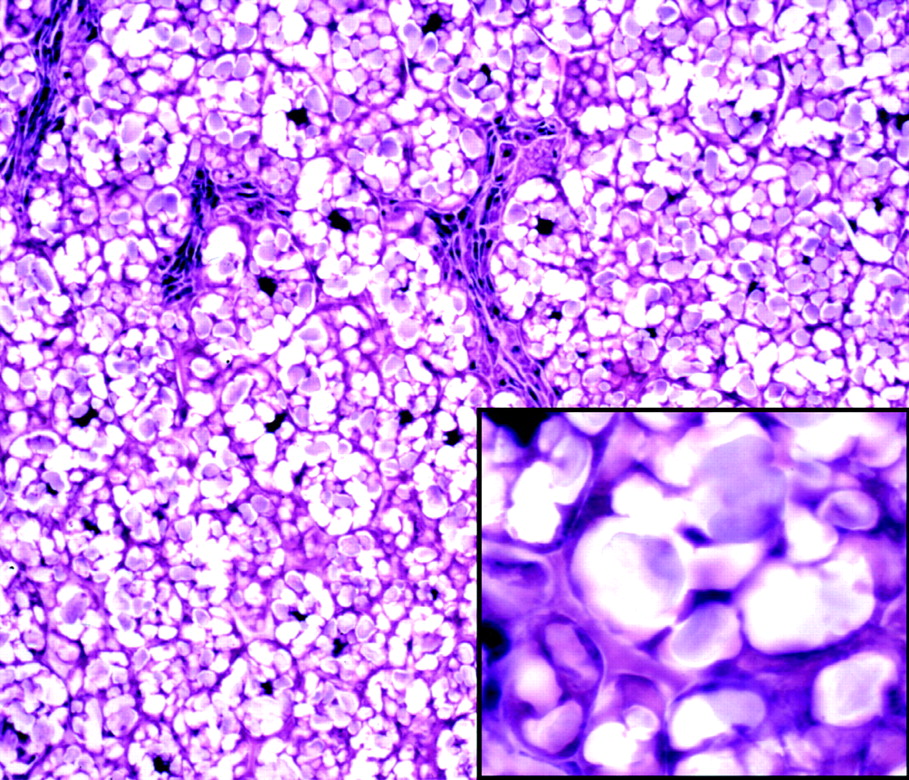
A 66 year old man with endstage renal disease, diabetes mellitus, and hypertension presented with recurrent pneumonia and a right pleural effusion for several months. He was admitted to the hospital with radiological findings of a pulmonary abscess involving the right lower lobe. A right lower lobectomy was performed. The gross specimen contained a peripheral abscess measuring 1.5 × 1.0 × 0.9 cm, in addition to extensive thick white/yellow exudate in most of the airways. Within the lumen of the right lower lobe bronchus was a tan/brown, firm, ovoid foreign object measuring 0.8 × 0.6 × 0.6 cm. Additional history obtained at this admission revealed a possible aspiration event of a peanut M&M® one year earlier. The gross and histological appearances of the specimen retrieved from the bronchus of this patient were compared with a formalin fixed paraffin wax embedded peanut M&M® to enable definitive comparative identification and diagnosis (fig 2A,B).

(A) The foreign object identified in the bronchus of patient 2. Patient history suggests this object was a peanut M&M® (haematoxylin and eosin stained). The patient’s specimen was compared with sections of a known formalin fixed peanut M&M® (B) for accurate identification. The chocolate candy coating was dissolved in formalin before sectioning, leaving only the peanut centre, seen above. Note the numerous hyaline globules within the cells (haematoxylin and eosin stained).
CASE 3
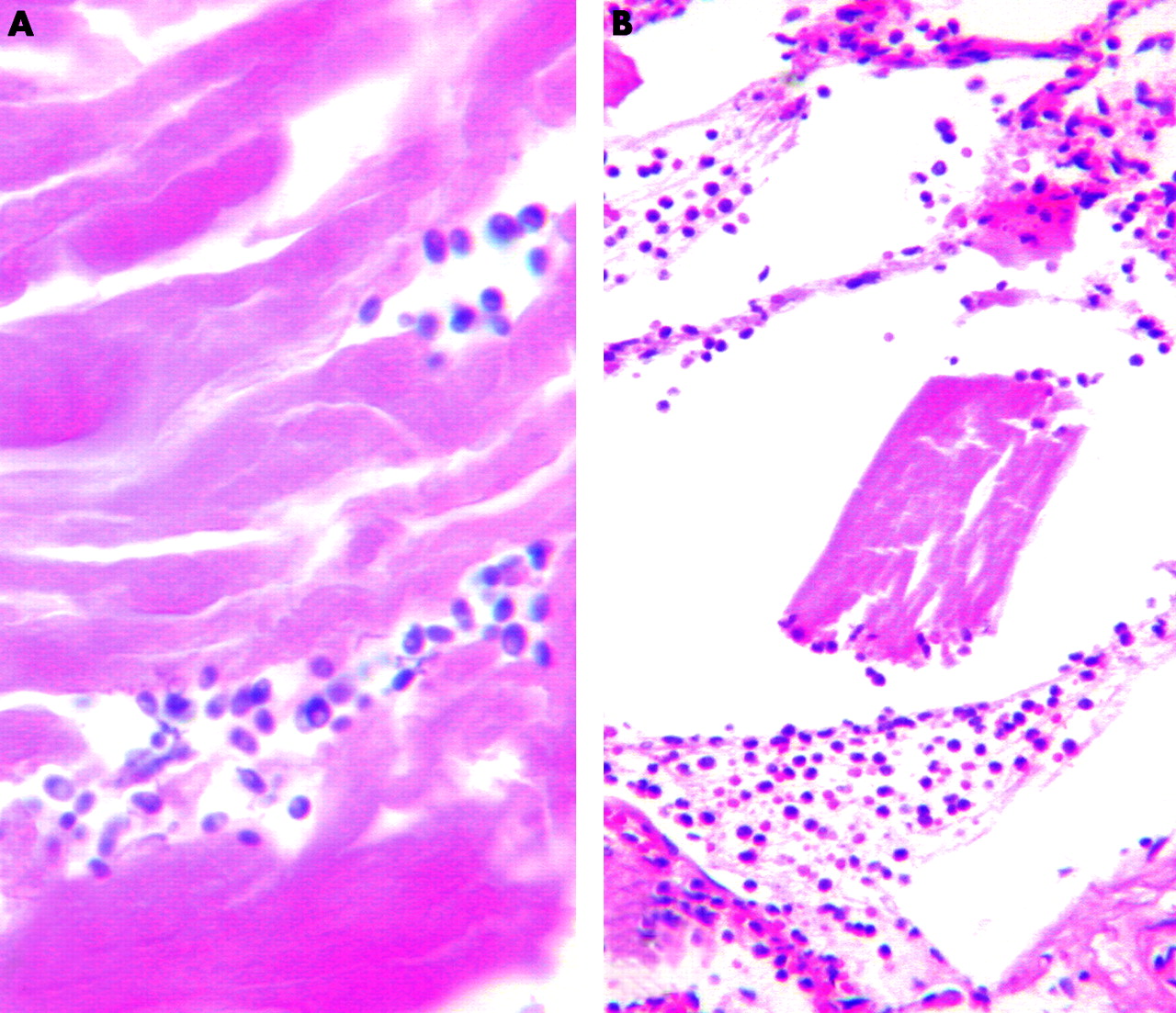
A 91 year old woman with spinal stenosis was admitted for surgical repair of a cerebral spinal fluid leak following spinal fusion and fixation. Following repair, the patient became hypotensive, and developed changes in her mental status. Two days later, she became unresponsive while being fed. Immediate intubation and resuscitation were performed, but the patient remained unresponsive, and support was withdrawn the following day. Postmortem examination revealed a 500 ml serosanguinous right pleural effusion with bilateral pulmonary congestion. The right lower lobe was consolidated and a tan/yellow, firm, irregular shaped foreign object measuring 1.0 × 1.0 × 0.8 cm was identified in the right main stem bronchus. Microscopically, the object comprised necrotic smooth and skeletal muscle with numerous associated yeast forms, consistent with unidentified cooked meat (fig 3A). The right lower lobe also contained smaller fragments of necrotic muscle fibres within scattered alveolar spaces (fig 3B). These smaller fragments were accompanied by squamous epithelial cells and acute bronchopneumonia.
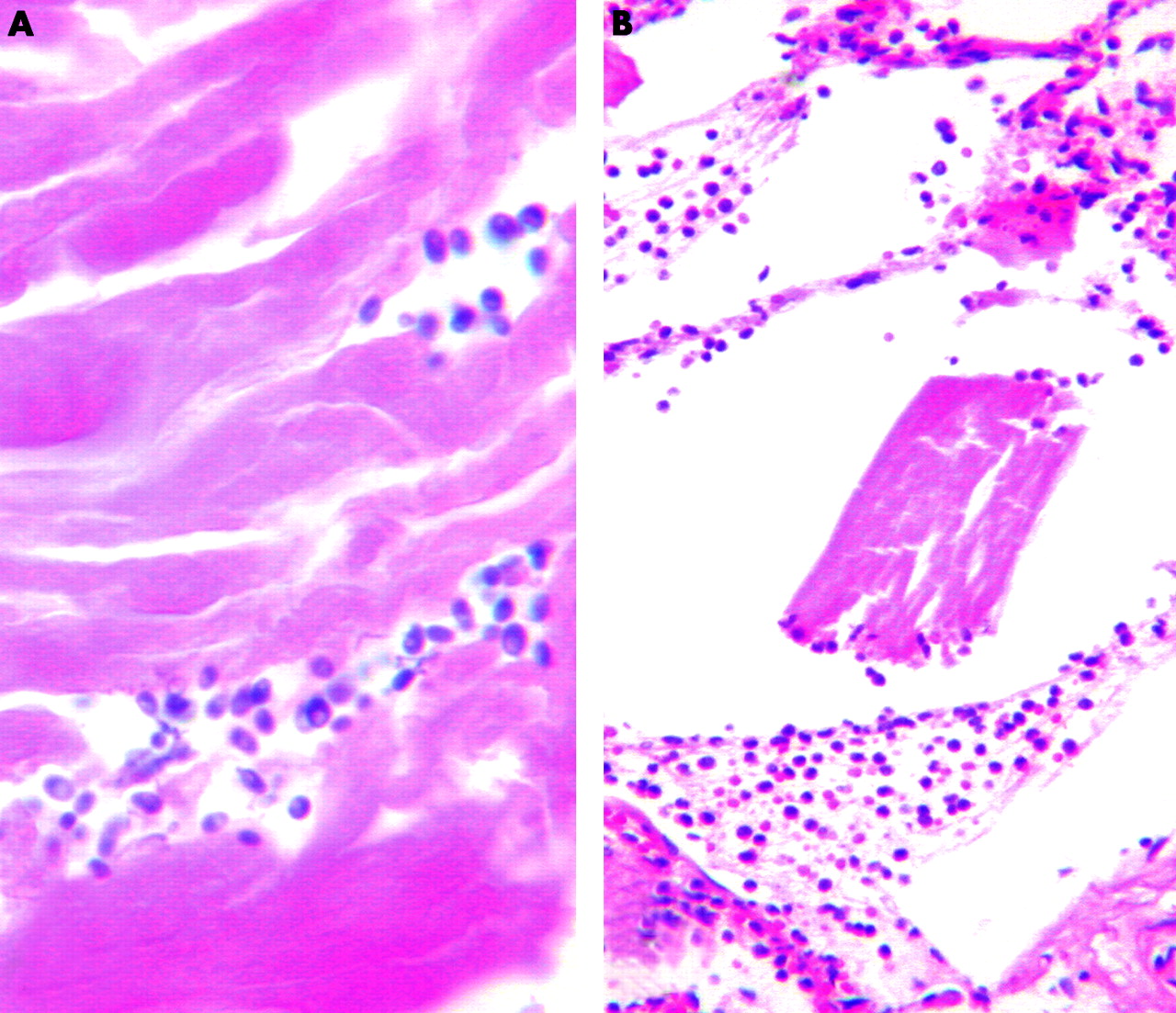
(A) A section from the bronchial foreign body in patient 3, comprising necrotic smooth and skeletal muscle with numerous admixed yeast forms, consistent with cooked meat (haematoxylin and eosin stained). (B) Smaller muscle fragments and acute inflammation were identified within this patient’s alveoli (haematoxylin and eosin stained).
DISCUSSION
Tracheobronchial foreign body aspiration has a range of possible outcomes, including immediate resolution, recurrent pulmonary disease, and death. Not uncommonly, there is no history of aspiration and positive identification of the foreign body is necessary for diagnosis.5 Confirming the occurrence of aspiration is important for patient management so that steps can be taken to prevent recurrence. Confirmation and specific identification of the foreign body may also be important for medicolegal purposes.
In the first case described above, the aspiration event was witnessed, and histological examination of the aspirated material served to confirm the diagnosis. As a result, the patient was recommended for swallowing studies, with possibly future dietary modifications.
The second case presented a considerably greater diagnostic dilemma because the history of aspiration was not known initially. The surgical specimen demonstrated features of longstanding infection and inflammation, but because of in vivo degeneration, the material located within the bronchus was not readily identified as foreign. Histological examination was necessary to recognise the object as plant material, and comparison with sections of a known formalin fixed peanut was useful for definitive comparative identification. It is interesting to note the histological similarities of the two specimens, despite the specimen being in the patient’s bronchus for several months.
Case 3 also presented a diagnostic challenge because of the abrupt nature of the patient’s presentation. The clinical differential diagnosis included asphyxia from aspiration, acute myocardial infarction, and cerebral vascular accident. As with case 2, the material located in the bronchus was not grossly identifiable and histological examination was necessary to confirm its foreign nature. In this instance, the bronchial material was most consistent with cooked meat.
These three cases demonstrate the potential diagnostic challenges of diagnosing tracheobronchial aspiration. The pathologist can greatly assist the clinician in making the correct diagnosis by identifying the retrieved foreign bronchial material. This necessitates a basic knowledge of the histological appearance of commonly aspirated foods. In certain instances, such as in medicolegal cases, the pathologist may be called upon for an accurate identification of the aspirated food.
“The pathologist can greatly assist the clinician in making the correct diagnosis by identifying the retrieved foreign bronchial material”
Table 1 outlines the aspirated foreign bodies received in this institution’s pathology department within the past 10 years. The results coincide with published data, showing the peanut to be the most commonly aspirated object in children, who comprise the largest population of patients with tracheobronchial aspiration.4–6 Vegetable matter and inorganic objects such as toy parts are also commonly aspirated objects in children, whereas adults aspirate food particles, medication tablets, dental pieces, and a variety of other inorganic substances.4–7
Foreign bodies received between 1992 and 2002
To examine the histological appearance of these commonly aspirated foodstuffs, several items including a peanut M&M™, cooked lentil, fresh blueberry and melon seeds, and cooked hotdog were fixed in 10% formalin for 24 to 48 hours, and then processed routinely and stained with haematoxylin and eosin (figs 2B, 4, 5A,B, and 6).
Lentil bean with nutrient material (starch) in cell compartments (haematoxylin and eosin stained).

(A) Blueberry and (B) watermelon seeds (haematoxylin and eosin stained). After sectioning, each seed consisted mainly of an outer shell (shown) with most of the centre being empty. Note the blue/purple pigmented plastids in the blueberry.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Hotdog with degenerated muscle tissue (arrow) and plant material (arrowhead) admixed with fat and connective tissue (haematoxylin and eosin stained).
As seen in fig 6 (hotdog), plant material is easily recognised as foreign because of its unique rigid double cell walls. Seeds, beans, and fruits also have a characteristic appearance, with rigid regular partitions containing nutrient material (figs 4, 5). The clear spaces within cell partitions in the lentil (fig 4) contain starch and are periodic acid Schiff positive.8 An atlas containing histological sections of many other food items is currently available.9
Take home messages
-
Tracheobronchial foreign body aspiration is a serious medical problem, with clinical manifestations ranging from acute asphyxiation to insidious lung damage
-
Foreign body aspiration is not always suspected clinically, and the pathologist may play an important role in making the diagnosis
-
Histological identification of the aspirated material may be necessary for definitive diagnosis
Striated muscle, bone, and cartilage may be recognised as foreign when combined with the clinical scenario, including location of the material (for example, within a bronchus) and a history of suspected aspiration. The presence of oral mucosa, colonising yeast, and/or oral flora may support the diagnosis of aspiration, when present in the airways and alveoli. This is possible with both conventional histology and cytology.10 These above features assist the pathologist in the diagnosis of foreign body aspiration.
In summary, foreign body aspiration may present a diagnostic challenge for the clinician and pathologist alike. Therefore, it must be included in the differential diagnosis when a patient has a history of recurrent lung disease or acute apnea. Furthermore, pathologists in surgical or postmortem practice may be well served by a general knowledge of commonly aspirated food histology. Through awareness and familiarity, the pathologist may play a crucial role in diagnosis and aid in subsequent patient management.