Article Text

Abstract
Background: Maximal inspiratory pressure (MIP) is a measure of inspiratory muscle strength. The prognostic importance of MIP for cardiovascular events among elderly community dwelling individuals is unknown. Diminished forced vital capacity (FVC) is a risk factor for cardiovascular events which remains largely unexplained.
Methods: MIP was measured at the baseline examination of the Cardiovascular Health Study. Participants had to be free of prevalent congestive heart failure (CHF), myocardial infarction (MI), and stroke.
Results: Subjects in the lowest quintile of MIP had a 1.5-fold increased risk of MI (HR 1.48, 95% CI 1.07 to 2.06) and cardiovascular disease (CVD) death (HR 1.54, 95% CI 1.09 to 2.15) after adjustment for non-pulmonary function covariates. There was a potential inverse relationship with stroke (HR 1.36, 95% CI 0.97 to 1.90), but there was little evidence of an association between MIP and CHF (HR 1.22, 95% CI 0.93 to 1.60). The addition of FVC to models attenuated the HR associated with MIP only modestly; similarly, addition of MIP attenuated the HR associated with FVC only modestly.
Conclusions: A reduced MIP is an independent risk factor for MI and CVD death, and a suggestion of an increased risk for stroke. This association with MIP appeared to be mediated through mechanisms other than inflammation.
- CHF, congestive heart failure
- CVD, cardiovascular disease
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- MI, myocardial infarction
- MIP, maximal inspiratory pressure
- RV, residual volume
- respiratory muscles
- cardiovascular disease
- congestive heart failure
- stroke
- maximal inspiratory pressure
Statistics from Altmetric.com
- CHF, congestive heart failure
- CVD, cardiovascular disease
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- MI, myocardial infarction
- MIP, maximal inspiratory pressure
- RV, residual volume
Maximal inspiratory pressure (MIP) is a measure of diaphragmatic inspiratory muscle strength. In chronic obstructive pulmonary disease (COPD) a reduced MIP is a risk factor for respiratory and total mortality.1,2 The prognostic importance of MIP for the outcomes of cardiovascular morbidity and mortality among older community dwelling individuals is unknown.
A low MIP may indicate poor muscle strength in general and therefore it may be a marker of generalised poor health. Inflammation, malnutrition, mechanical stress, metabolic stress, oxidative stress, and drugs have all been related to reduced inspiratory and general muscle strength.3–7 Reduced MIP may therefore be a marker of the effects of these factors on muscle strength.
Diminished respiratory function as measured by forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), or peak expiratory flow (PEF) is associated with an increased risk of cardiovascular mortality and morbidity.8,9,10,11 The inverse relationship between these pulmonary function parameters and cardiovascular disease remains largely unexplained. MIP can be measured easily without the need for a full pulmonary function laboratory and might be an alternative to FVC, which is one of the standard pulmonary function tests, as a predictor of cardiovascular mortality and morbidity. If MIP is a risk factor, respiratory muscle strength tests done in the clinic may help to identify persons at increased risk of cardiovascular morbidity and mortality. In the Cardiovascular Health Study, a population based prospective cohort of older adults, MIP was measured in addition to the classical lung function parameters FEV1 and FVC.12,13
We hypothesised that reduced MIP is an independent risk factor for cardiovascular mortality and morbidity among older community dwelling individuals, and that it may in part account for the previously reported association between reduced FVC and cardiovascular disease (CVD). The a priori hypothesis was that a lower MIP would be associated with an increased risk of disease outcome, more strongly at low values of MIP. In addition, we evaluated several potential mechanisms through which MIP might be associated with morbidity and mortality. The richness of the Cardiovascular Health Study enabled us to consider the role of sex, age, weight, height, blood pressure, smoking, C-reactive protein (CRP), fibrinogen level, white blood cell count, and serum albumin in explaining an association of MIP with the cardiovascular outcomes.
METHODS
Study design and population
The Cardiovascular Health Study (CHS) is a multicentre, prospective, community based, epidemiological, observational study in the elderly, designed to investigate risk factors for cardiovascular death and morbidity.12
The cohort was recruited by sampling from Medicare enrollees at four field centres. The sampled individual and eligible household members were recruited. The eligible participants included non-institutionalised individuals aged 65 years and over. A cohort of 5201 individuals was enrolled beginning in 1989 and an additional cohort of 687 African Americans was added in 1992–3. Because MIP was only measured in 1989, the second cohort was not included in this analysis.
Details of the CHS have been published elsewhere.12 Briefly, at baseline interviews and questionnaires were used to obtain information on medications, functional status, physical activity, and medical history. Participants reported to the CHS field centre clinic after a 12 hour overnight fast for assessment of blood levels including CRP, fibrinogen, white blood cell count and serum albumin, blood pressure, and cognitive function, as well as anthropometric, electrocardiographic, echocardiographic, carotid artery ultrasound, and other objective measurements including pulmonary function tests. The latter included MIP, FVC, and FEV1 and were measured according to American Thoracic Society recommendations.14 Smoking was classified by self-report as current, former, or never smoker. Former smokers had not smoked during the 30 days preceding examination. Emphysema and chronic bronchitis were based on self-report of a current physician diagnosis. Left ventricular mass was determined from EKG.15 Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in metres.
Follow up and outcomes
Participants were contacted every 6 months and were asked about cardiovascular events and hospital admissions. Outpatient and hospital records were reviewed. All potential cardiovascular events were adjudicated by the CHS Events Committee as reported previously, and were also ascertained through HCFA records.16,17 The outcomes of interest included incident congestive heart failure (CHF), myocardial infarction (MI), stroke, and CVD death. This report examines events through June 2000.
Statistical analysis
Descriptive statistics and unadjusted cardiovascular event rates were calculated for men and women separately, as well as for the overall study population. MIP was modelled in quintiles, which were constructed for men and women separately. The quintile with the greatest MIP was the referent group. To investigate the continuous relationship between MIP and FVC, sex specific plots were constructed using LOWESS smoothing with a span of 15%.18
Separate Cox proportional hazards analyses were conducted to determine the association between MIP and the four outcomes of interest. Subjects were followed until the outcome event or censoring for death or end of follow up occurred. For each of the four outcomes parsimonious models were constructed by examining potential confounding variables and then eliminating variables that did not change the coefficient estimate of MIP by more than 10%. Age, sex, weight and height are known to be associated with MIP and cardiovascular disease, and therefore were always included in the models. All confounding variables that appeared in at least one of the four parsimonious models were combined so that the same model was used for all four outcomes.
For each outcome of interest three models were investigated: an unadjusted model that included only MIP and two models that adjusted for the confounding variables (in one model FVC was included, while in the other model it was excluded). Effect modification by sex, age (divided at the median of >71 or <71 years), and the presence or absence of obstructive lung disease was investigated in all models.
RESULTS
Of the 5201 participants in the first cohort, 783 were excluded because they had a history of stroke, MI, or CHF at study enrolment and a further 565 were excluded because they did not have MIP measured. Fourteen participants with MIP values below 10 cm H2O or above 180 cm H2O for women and 200 cm H2O for men were excluded because these values probably represent errors, leaving 3839 subjects for analysis.
Table 1 shows the characteristics of the study participants included in the analyses, as well as of the 565 subjects without MIP measurements. The mean (SD) age was 72.9 (5.4) years, 60% were women, and 95% were white. MIP values were normally distributed with a mean of 79.5 cm H2O for men and 54.8 cm H2O for women. The 565 subjects who did not have an MIP measurement had similar characteristics to the subjects included in the analyses. The median follow up period was 10.3 years. Incidence rates for CHF, MI, stroke and CVD death were 18.6, 12.7, 12.1, and 12.0 per 1000 person-years, respectively. Incidence rates for men exceeded those for women in all diseases as well as in CVD death. The largest sex difference in incidence rate was seen for incident MI.
Characteristics of 3839 study participants included in the analysis and 565 subjects in whom maximal inspiratory pressure (MIP) was not measured
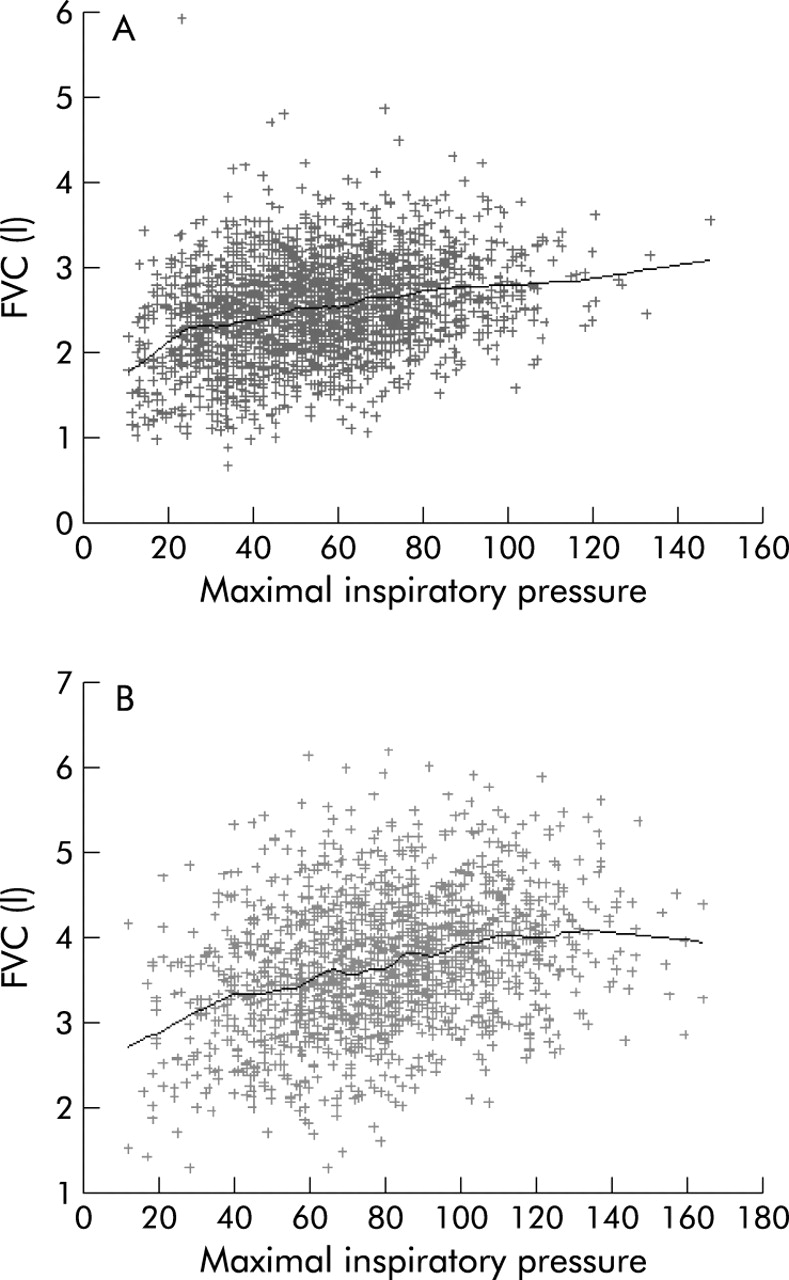
MIP was moderately correlated with FVC (r = 0.51). When analysing this relationship by visual inspection of scatter plots with LOWESS smoothing, it seemed that the increase in FEV1 per unit increase in MIP was most pronounced in those with the lowest MIP values, especially in women (fig 1A and B).

Scatter plots of the relationship between maximal inspiratory pressure and forced vital capacity (FVC) for (A) women and (B) men using LOWESS smoothing with a span of 15%.
MIP and FVC as risk factors for cardiovascular events
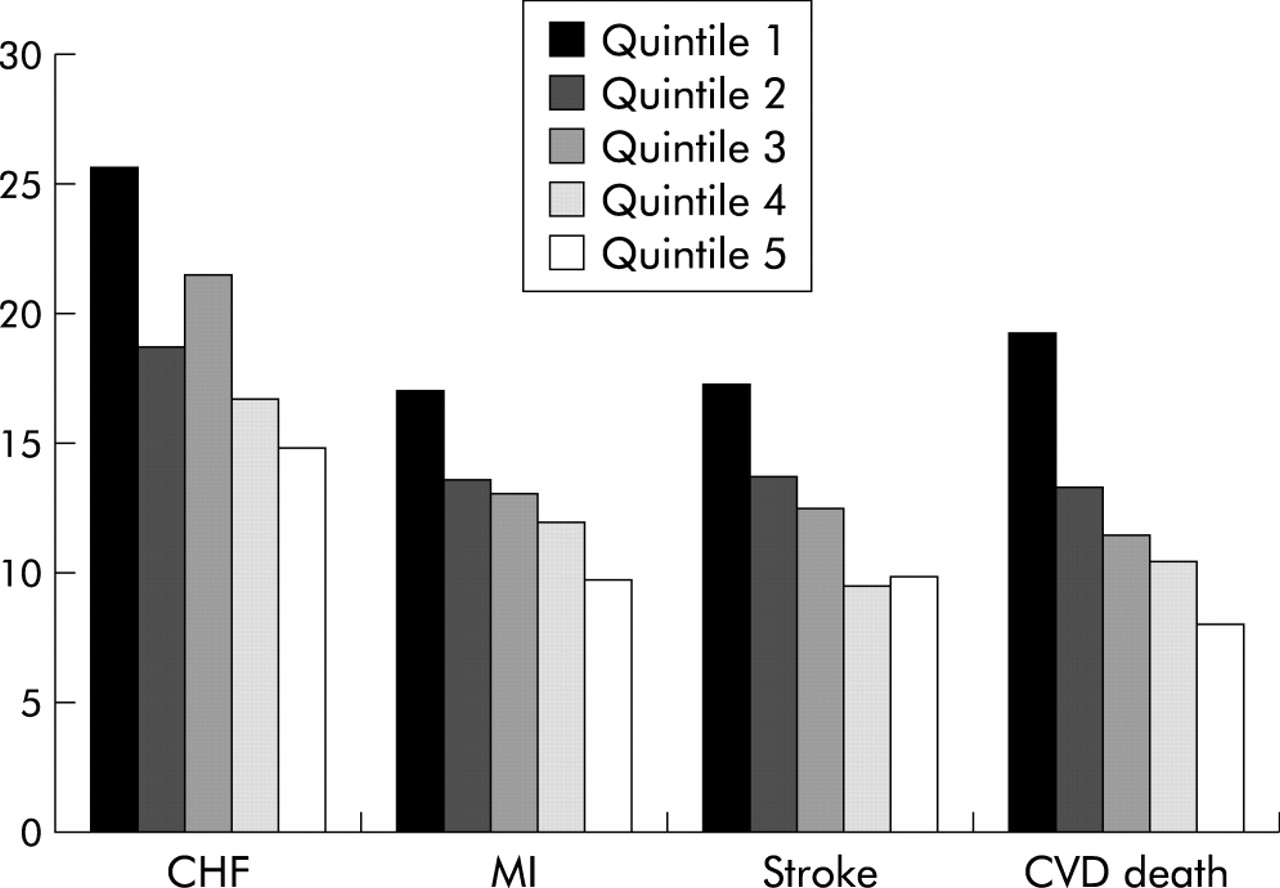
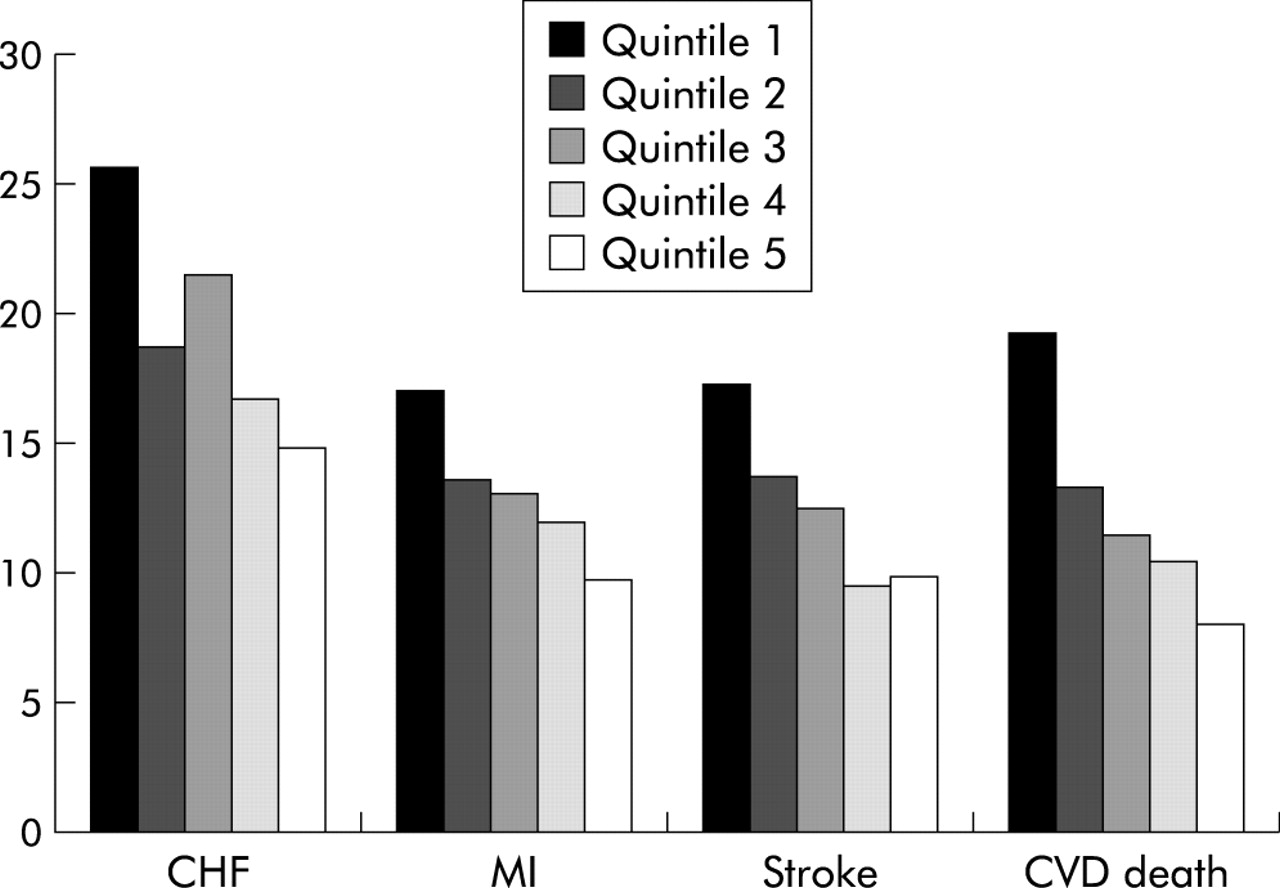
In unadjusted analyses, subjects in the lowest quintile of MIP had a 1.75-fold increased risk for incident CHF, MI and stroke, and experienced a 2.5-fold increased risk of CVD death compared with subjects in the highest quintile of MIP (table 2). There was a gradient in the event rates for the four outcomes of interest with the highest rates in the lowest quintile of MIP (fig 2). While systolic blood pressure, smoking status, maximal stenosis, HDL, and left ventricular mass were confounders in the relationship between MIP and at least one of the cardiovascular outcomes, asthma, bronchitis or emphysema were not and were therefore not included in the analyses. After adjustment for sex, age, weight, height, and the aforementioned confounders, subjects in the lowest quintile of MIP were at a 1.5-fold increased risk for MI and CVD death. The hazard ratio (HR) for the lowest quintile of MIP reached borderline significance in stroke (table 2). Adjustment for FVC attenuated these findings somewhat, so that 1 was included in the 95% confidence intervals. As a result no significant associations between MIP and disease outcome were observed in models that adjusted for FVC along with other confounders, although the HRs for the lowest quintile of MI, stroke and CVD death reached borderline significance.
Maximal inspiratory pressure (MIP): hazard ratios (HRs) with 95% confidence intervals (CI) for incident congestive heart failure (CHF), myocardial infarction (MI), stroke or cardiovascular disease (CVD) death
{kind=link}
{kind=link}
Age adjusted event rates per 1000 person-years by quintiles of maximal inspiratory pressure (MIP) for congestive heart failure (CHF), myocardial infarction (MI), stroke, and cardiovascular disease (CVD) death.
The results for FVC appear to be the same as MIP for MI and CVD death, but FVC is a stronger predictor for CHF while MIP may be slightly stronger than FVC for stroke (table 3). The association between FVC and CVD outcomes was modestly attenuated by the addition of MIP to the models, with the exception of the FVC-CHF association.
Forced vital capacity (FVC): hazard ratios (HRs) with 95% confidence intervals (CI) for incident congestive heart failure (CHF), myocardial infarction (MI), stroke or cardiovascular disease (CVD) death
Effect modification
No statistically significant interactions by sex, age, or the presence of obstructive lung disease were found.
Potential mechanisms
In cross sectional analyses, MIP was inversely related to levels of CRP, fibrinogen, and white blood cells and directly related to serum albumin (table 4). When added to the adjusted models, with or without FVC, none of these four inflammatory parameters changed the estimates for the HRs of MIP by more than 10% for all four outcomes under investigation.
Levels of C-reactive protein (CRP), fibrinogen, white blood cell (WBC) count and albumin by sex specific quintiles of maximal inspiratory pressure
DISCUSSION
In a community dwelling elderly population free of prevalent CHF, MI, and stroke, the lowest quintile of MIP was associated with an approximately 1.5-fold increase in the risk of MI and CVD death after adjustment for non-pulmonary function covariates. The results suggest a potential inverse relationship with stroke, but there was little evidence of an association of MIP and CHF. For the outcomes of MI, stroke and CVD death the risk associated with a reduced MIP is similar to that of a reduced FVC. Inclusion of FVC (modestly) attenuated the effect of MIP on outcome. Conversely, inclusion of MIP could explain a small part of FVC as a risk factor for MI, stroke, and CVD death. Thus, low respiratory muscle strength may, at best, play a small role in explaining the association between FVC and death. The association of MIP with the cardiovascular outcomes does not seem to be mediated by inflammatory factors.
MIP and FVC as risk factors for cardiovascular events
Many studies have shown that reduced pulmonary function, especially a reduced FVC, is a risk factor of cardiovascular events, but the association has remained unexplained since it was first reported in 1976.8 By including MIP in models already containing FVC, we found that the HRs of FVC were attenuated by 3–10% for MI, stroke, and CVD death. One possible explanation is that reduced inspiratory muscle strength affects the measurement of FVC, especially at its lowest level. FVC, a measure of maximal voluntary ventilation, is measured from residual volume (RV) where a patient has exhaled maximally to maximal inspiration, or vice versa. The volume at maximal inspiration is determined not only by lung volume, but also by the ability of the patient to overcome the elastic recoil of the lung. Because this elastic recoil force is relatively weak, this will only become important as a limiting factor when inspiratory muscle force is greatly reduced. This hypothesis seems to be supported by the fact that, in the lowest region of respiratory muscle strength, the greatest increase in FVC was found with each unit increase in MIP. Other evidence for the relationship between MIP and FVC comes from a study in patients with neuromuscular disorders, where respiratory muscle training led to increased MIP and stabilisation or improvement of FVC.19 Another study in patients with chronic cervical spinal cord injury showed both a strong increase in MIP and FVC following respiratory muscle training.20 These studies included patients with severely impaired respiratory muscle function. Other investigations found that inspiratory muscle training in patients with COPD increased MIP but did not affect pulmonary function parameters,21,22 perhaps because respiratory muscle function was still adequate to overcome the elastic recoil of the lung.
One limitation of this study is the lack of data on RV. Because MIP is measured from RV, a reduced MIP might also be caused by an increased RV which renders an unfavourable starting point for the MIP manoeuvre.
It is not clear why a reduced respiratory muscle function does not appear to be a risk factor for incident CHF. Although a reduced MIP was not a predictor of incident CHF, in patients with prevalent CHF a reduced MIP was an independent predictor of prognosis.23 However, in the first investigation, other pulmonary function parameters in addition to MIP, as well as other potential confounders such as left ventricular mass and carotid stenosis which may have attenuated the MIP association, were not included in the analytical models.
Potential mechanisms
In this cohort, MIP was correlated with cross sectional measures of inflammation. However, these markers of pathophysiological processes did not appear to explain the association between reduced respiratory muscle strength and incident cardiovascular events. Measurement error could reduce the power to identify the mechanism. Reduced respiratory muscle strength may be a marker of an underlying process which mediates its effect through a mechanism other than inflammation—such as mechanical, metabolic, or oxidative stress.6,7 Recently, Rantanen et al24 examined the association between muscle strength, assessed by handgrip strength testing, and total and cause-specific mortality in moderately to severely disabled elderly women. They also focused on the plausible contributing factors to this association. They concluded that, in older disabled women, handgrip strength was a powerful predictor of cause-specific and total mortality. However, similar to the results in the present study, potential mechanisms or chronic diseases failed to explain the association.
Other limitations of the study include missing data on MIP and a lack of diversity of the individuals sampled because MIP was not measured in the minority cohort added later. However, the subjects in the original CHS cohort without MIP measurement do not seem to be a selected group (as can be seen from table 1), and their exclusion does not seem to influence the results. Strengths of the study include the large sample size of well characterised healthy men and women, enabling us to look at various risk factors for incident cardiovascular events as well as at possible explanatory mechanisms.
Respiratory muscle strength is easy to measure without the need for a pulmonary function laboratory. Like MIP, peak inspiratory flow is a measure of inspiratory muscle strength. For the management of asthma and COPD, peak inspiratory flow meters are used to assess whether patients with obstructive airway disease can generate a sufficient peak inspiratory airflow to use inhalers with a relatively high internal resistance.25 Respiratory muscle strength can easily be assessed with this simple and inexpensive device, even during a short office visit, whereas the measurement of FVC and other pulmonary function parameters requires more training, a pulmonary function laboratory, and considerably more time and expense.
In conclusion, a reduced MIP was an independent risk factor for MI and CVD mortality, and was indicative of an increased risk for stroke as well. This association appeared to be mediated through mechanisms other than inflammation. Reduced MIP appeared to account for only a small portion of the association between FVC and CVD. Respiratory muscle strength is easily measured clinically and could serve as a “poor person’s” FVC to identify older persons without clinical cardiovascular disease who are at an increased risk of cardiovascular morbidity and mortality.
REFERENCES
Footnotes
-
Sources of support: National Heart, Lung, and Blood Institute
Linked Articles
- airwaves