Article Text

Abstract
Background: The epithelial reticular basement membrane (Rbm) of the airway wall thickens in patients with asthma. However, whether the thickening parallels whole airway wall thickening, which limits airflow, is unknown. The aim of this study was to examine the correlation between the bronchial Rbm thickening and whole airway wall thickening in asthma. In addition, the association of Rbm and whole wall thickening with airflow obstruction was examined.
Methods: Forty nine patients with asthma and 18 healthy control subjects took part in the study. The Rbm thickness was measured in bronchial biopsy specimens and whole airway wall thickness was assessed with high resolution computed tomographic (HRCT) scanning after pretreatment with oral steroids for 2 weeks and inhaled β2 agonist to minimise reversible changes of the airway walls. The percentage airway wall area (WA%; defined as (wall area/total airway area) × 100) and percentage airway wall thickness (WT%; defined as [(ideal outer diameter – ideal luminal diameter)/ideal outer diameter] × 100) were determined from HRCT scans to assess whole airway wall thickness. Spirometric tests were also performed.
Results: WA% and WT% were higher in patients with asthma than in healthy subjects. Both WA% and WT% were strongly correlated with Rbm thickness. Moreover, these three indices of airway wall thickness were inversely correlated with the percentage of predicted forced expiratory volume in 1 second in patients with asthma.
Conclusions: These findings indicate that Rbm thickening parallels whole airway wall thickening which can cause irreversible airflow obstruction in patients with asthma.
- subepithelial layer thickness
- airway wall thickness
- high resolution computed tomography
- asthma
Statistics from Altmetric.com
Remodelling of the airway wall in patients with asthma occurs through desquamation of the bronchial epithelium with proliferation of goblet cells,1–3 deposition of collagen in the reticular layer of the subepithelial area,1, 4–9 hyperplasia of mucous glands, hypertrophy and hyperplasia of bronchial smooth muscle,10–13 and hyperplasia of bronchial blood vessels.15 Although remodelling of the airway wall has usually been evaluated at necropsy after death from asthma,10–14 it has recently been assessed using bronchial biopsy specimens1, 4–9, 15, 16 and high resolution computed tomography (HRCT).17–20 Although biopsies can demonstrate several qualitative changes of the bronchial wall, they cannot assess precisely changes in airway smooth muscle or the thickening of the whole airway wall. Several studies have suggested that the thickening of the epithelial reticular basement membrane (Rbm) shown in bronchial biopsy specimens contributes to airflow obstruction, airway hyperresponsiveness, and respiratory symptoms.1, 4–16 However, whether the increase in Rbm thickness by only several micrometres can cause narrowing of the airway lumen is uncertain. Whole airway wall thickening can be measured with HRCT scanning, although this method cannot be used to identify which components—such as the Rbm or smooth muscle—of the airway wall are thickened. Confirmation that whole airway wall thickness parallels Rbm thickness and induces airflow obstruction in patients with asthma may help to clarify the pathogenesis of irreversible or refractory airflow obstruction. However, to date no studies have compared bronchial biopsy examinations with HRCT scanning for evaluating airway wall thickness in patients with asthma.
In this study we have measured Rbm thickness in bronchial biopsy specimens and measured whole airway wall thickness on HRCT scans from patients with asthma and healthy subjects. The relationship between Rbm thickness determined in bronchial biopsy specimens and whole airway wall thickness evaluated by HRCT scanning was studied and the effects of airway wall thickening on airflow obstruction in patients with asthma were evaluated.
METHODS
Subjects
Forty nine patients with mild to moderate asthma and 18 healthy control subjects matched for age and sex were examined. Asthma was diagnosed according to American Thoracic Society criteria21 with reversibility of forced expiratory volume in 1 second (FEV1) in response to a bronchodilator of >15% at the initial examination. Asthma severity was classified according to the Expert Panel Report on the guidelines for the diagnosis and management of asthma.22 All subjects were non-smokers and the presence of chronic bronchitis, emphysema, bronchiectasis, and inactive pulmonary tuberculosis were ruled out by chest radiography, computed tomographic (CT) scanning, and clinical symptoms. Patients with peptic ulcers, diabetes mellitus, or hyperlipidaemia were excluded. In all patients the variations in peak expiratory flow were less than 30% in the previous month and none had experienced severe asthma attacks or had been admitted to hospital for treatment. Thirty eight of the 49 patients with asthma inhaled beclomethasone dipropionate in a dose of 400–1600 μg per day (table 1). Control subjects had no history of wheezing, asthma, or smoking and had normal spirometric test results.
Subject characteristics
To minimise reversible changes such as inflammation and bronchospasm, all patients with asthma received 0.5 mg/kg prednisolone per day orally for 2 weeks and inhaled salbutamol sulfate (2 puffs) 15 minutes before undergoing respiratory function tests and HRCT. Oral prednisolone, 0.5 mg/kg/day for 7–14 days, has been recommended to control worsening chronic asthma.23 In our study we administered prednisolone (0.5 mg/kg/day for 14 days) as pretreatment because patients had mild to moderate asthma without severe symptoms upon entry. We believed pretreatment with oral prednisolone and an inhaled β2 agonist was sufficient to suppress latent inflammation and airway spasms. HRCT was performed during the end inspiratory phase after the respiratory function tests. In addition, bronchial biopsy specimens were taken in 22 of the 49 patients who consented to bronchoscopic examination after HRCT scanning.
The study was approved by the Showa University Ethics Committee and all subjects gave written informed consent.
Pulmonary function tests
Spirometric tests were performed with an Autospiro AS-300 spirometer (Minato Co, Osaka, Japan) to measure forced vital capacity, FEV1, and peak expiratory flow. Each measurement was repeated at least three times and the highest acceptable measurement was compared with normal predicted values.
HRCT scanning
The thoracic HRCT scan system (Siemens Somatom Plus4, Erlangen, Germany) was used as described previously19, 24 with the thin section (1 mm collimation) technique at 120 KVp, 250 mA, 1 second scan time, and 20 cm field of view at the end inspiratory phase. Scans were done at five selected levels: the superior margin of the aortic arch, the tracheal carina, 1 cm below the carina, the inferior pulmonary veins, and 2 cm above the diaphragm.19 The images were viewed at a window level of –450 Hounsfield units (HU) and a window width of 1500 HU to analyse airway wall thickness.19, 24
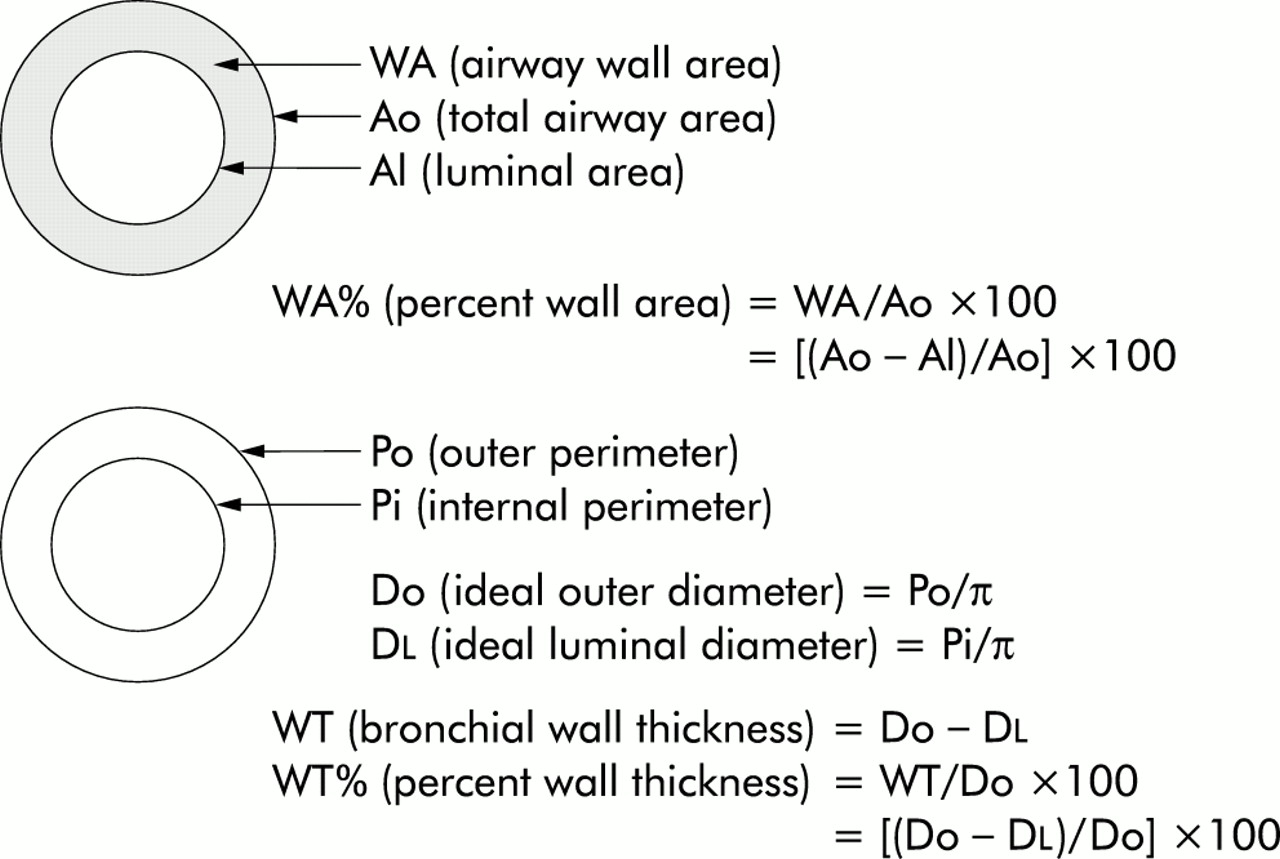
Airway wall dimensions were calculated using a validated method described by Okazawa and Awadh.17, 19 The CT images were printed at a magnification of ×10 that of standard prints and the outer and internal perimeters of bronchial cross sections were traced. The images of each bronchus examined were approximately perpendicular to the bronchial axis, at which the ratio of the diameter of the long axis to that of the short axis was less than 1.2. The traced images were scanned into a Macintosh personal computer (Apple Computer, Cupertino, CA, NIH image) and the outer perimeter (Po, mm), internal perimeter (Pi, mm), total airway area (Ao, mm2), and luminal area (Al, mm2) were measured. We also calculated ideal outer diameter (Do = Po/π) and ideal luminal diameter (Dl=Pi/π). Three or more bronchi with Dl of 3–5 mm in a single scanning slice were examined (a total 15 or more bronchi per subject). Because bronchial biopsies were taken from subsegmental bronchial bifurcations whose luminal diameters were also 3–5 mm, bronchi of this size were chosen.
Percentage wall area (WA%), defined as [(Ao – Al)/Ao] × 100, and percentage wall thickness (WT%), defined as [(Do – Dl)/Do] × 100, were calculated (fig 1). The measurements were performed by two radiology technicians in a blinded fashion. Mean values from 15 or more measurements per subject were calculated and compared in patients with asthma and healthy controls.

Indices of airway wall thickness on HRCT scan.
Bronchial biopsies
No patients had had an asthma attack before fibreoptic bronchoscopy (BF type 240, Olympus Co, Tokyo, Japan). Lidocaine (20 ml of 2% solution for local anaesthesia), atropine (0.5 mg intramuscularly), and midazolam (0.1 mg/kg by slow intravascular infusion) were used as premedication. At the start of bronchoscopy the subject's percutaneous oxygen saturation and pulse were monitored by pulse oximeter (Pulsox, Teijin Co, Tokyo, Japan) and respiratory rate and blood pressure were observed. Four or five biopsy specimens were taken from subsegmental bronchial bifurcations in the right lower lung in each subject. The luminal surfaces of the biopsy specimens were stained with eosin to ensure proper orientation for cross sectioning. Each specimen was fixed in 10% buffered formalin solution at room temperature, embedded in paraffin, subsequently sectioned at 5 μm thick with a microtome, and stained with haematoxylin-eosin. One measurable stained section was chosen from each biopsy specimen (total 3–5 stained sections from each subject used for measurement); sections from incorrectly oriented biopsies were discarded.
Rbm thickness was quantified by measuring the area of the whole Rbm (from the base of the bronchial epithelium to the outer limit of the reticular lamina) and the length of true basement membrane of the Rbm area using a computerised image (Apple Computer, Cupertino, CA, NIH image). Rbm thickness was calculated as Rbm area/length of basement membrane and the mean values of 3–5 measurements in 3–5 stained sections per subject were used for analysis. All measurements were performed by a single pathologist in a blinded fashion.
Statistical analysis
All statistical analyses were performed with StatView software, version 4.5 (Abacus Concepts, Berkeley, CA, USA) on a Macintosh computer. Values were expressed as mean (SD). Simple regression analysis was used to compare WA% or WT% with Rbm thickness or percentage predicted FEV1 (%FEV1). The Mann-Whitney U test was used to compare WA%, WT%, and %FEV1 between patients with asthma and healthy controls. Differences with p values of <0.05 were considered significant.
RESULTS
Subject characteristics
Characteristics of the 49 study subjects and 18 healthy controls, including age, sex, duration of asthma, dose of beclomethasone dipropionate, and respiratory function measurements, are shown in table 1. The mean %FEV1 (before pretreatment) differed significantly between the groups (p<0.05).
Differences in WA% and WT% between patients with asthma and healthy controls
The findings of HRCT scan measurements are shown in fig 2A and B. Both WA% and WT% were significantly higher in patients with asthma than in healthy controls (p<0.001). The mean (SD) WA% and WT% were 68.8 (5.7)% and 44.3 (5.0)% for patients with asthma and 55.3 (5.6)% and 35.0 (3.9)% for healthy controls. Neither WA% nor WT% was correlated with the age of the patients or with duration of asthma (data not shown). In addition, neither WA% nor WT% differed significantly among the five selected levels of the HRCT scan in patients with asthma or healthy controls. Furthermore, both WA% and WT% were significantly higher in patients with asthma than in healthy controls in slices from all lung levels (p<0.05; fig 3A and B). Figure 4 shows representative HRCT images of a healthy control (fig 4A) and a patient with asthma (fig 4B).

(A) WA% and (B) WT% in healthy controls and patients with asthma. Both WA% and WT% differed significantly between healthy controls (open circles) and patients with asthma (shaded circles) (p<0.0001). Error bars are expressed as mean (SD).

(A) WA% and (B) WT% in each slice of the HRCT scan in healthy controls (open squares) and patients with asthma (shaded squares). Level of slice: 1 = superior margin of the aortic arch; 2 = tracheal carina; 3 = 1 cm below the carina; 4 = inferior pulmonary veins; 5 = 2 cm above the diaphragm. In all slices both WA% and WT% differed significantly between healthy controls and patients with asthma (p<0.01). Neither WA% nor WT% differed between the five slice levels.

HRCT scan representing the airway wall in (A) a healthy control subject and (B) a patient with asthma. Note that the airway wall is thicker (arrow) in the asthmatic patient than in the healthy control.
Correlation between WA%, WT%, and Rbm thickness
Three indices of airway wall thickness (WA%, WT%, and thickness of the Rbm) were compared. Rbm thickness was positively correlated with both WA% (r=0.74, p<0.0001) and WT% (r=0.64, p=0.001; fig 5).

Correlation of bronchial Rbm thickness with WA% and WT%.
Correlation of %FEV1 with WA%, WT%, and Rbm thickness
To examine whether the three indices of airway wall thickness reflect airflow obstruction in patients with asthma they were compared with %FEV1 determined after inhalation of a β2 agonist. %FEV1 was negatively correlated with Rbm thickness (r=–0.66, p=0.001), WA% (r=–0.61, p<0.0001), and WT% (r=–0.53, p<0.0001; fig 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation of %FEV1 with Rbm thickness, WA%, and WT%.
DISCUSSION
Our study shows for the first time, to our knowledge, a strong positive correlation between Rbm thickness determined in biopsy specimens and whole airway wall thickness determined by HRCT scanning in patients with asthma. Furthermore, this thickening was correlated with a deterioration in respiratory function. Many investigators have reported a thicker Rbm in patients with asthma than in healthy subjects.1, 4–9 However, whether an increase in Rbm thickness of only a few micrometres can cause narrowing of the airway lumen or airflow obstruction has been unclear. Furthermore, the thickening does not explain why whole airway wall thickness on HRCT scans was 20% greater in patients with asthma than in healthy subjects. Our findings suggest that Rbm thickening appears simultaneously with hypertrophy or hyperplasia of other components of the airway wall which may cause respiratory function deterioration in patients with asthma. Previous studies have used Rbm thickening as an index of remodelling of the airway wall in asthma. Our findings also support the results of these previous reports. Furthermore, we found no difference in mean airway wall thickness in five HRCT slices obtained at different lung levels, which suggests that irreversible airway wall thickening occurs uniformly throughout the lung in asthma.
Three indices of airway wall thickness—Rbm thickness in bronchial biopsy specimens and WA% and WT% in HRCT scans—were significantly and negatively correlated with %FEV1. These findings suggest that the irreversible airway wall thickening induces airflow obstruction in patients with asthma. Previous studies have also shown that thickening of either the bronchial Rbm or the airway wall is correlated with disease severity, decreases in respiratory function, and airway hyperresponsiveness in patients with asthma.5, 6, 16, 19 Several recent studies have found that patients with asthma, even if they are receiving intensive treatment including inhaled steroids, had a greater decline in respiratory function with age than did healthy controls.25, 26 Our findings and those of these earlier studies suggest that some patients with asthma have irreversible or partially reversible airway obstruction which may cause refractory airway obstruction despite treatment with corticosteroids, bronchodilators, and other anti-inflammatory drugs. Such airway obstruction can be induced by structural alterations of the bronchi.
In contrast, other studies have reported that airway wall thickening is not correlated with airflow obstruction.1, 8, 9, 20, 27 In asthma, many factors in addition to irreversible airway wall thickening may contribute to airflow obstruction including airway wall oedema, inflammation, mucus secretion, and bronchial smooth muscle spasms. We used doses of oral steroids and inhaled β2 agonists before the trial which were sufficient to prevent the effects of reversible changes of the airway wall. For example, we rarely found eosinophils in bronchial biopsy specimens (data not shown). Pretreatment with anti-inflammatory agents and bronchodilators was needed to evaluate the irreversible airway wall thickening and to compare the thickness with respiratory function. Some previous studies may have measured both reversible and irreversible structural alterations when comparing airway wall thickness with respiratory function.
In conclusion, our findings show that whole airway wall thickening evaluated by HRCT scanning parallels bronchial Rbm thickening determined in biopsy specimens after pretreatment with oral steroids and inhaled β2 agonists. Thickening of the airway wall assessed either in biopsy specimens or by HRCT scanning is also correlated with airflow obstruction. Our findings suggest that Rbm thickening appears with hypertrophy or hyperplasia of other components of the airway wall in patients with asthma and that these irreversible changes of the airway wall may cause respiratory function deterioration and refractory airway obstruction.
REFERENCES
Footnotes
-
Informed consent was obtained from all subjects, and the human experimentation guidelines of the US Department of Health and Human Services and those of the Showa University Human Investigation Committee were followed.