Article Text

Abstract
Background Neural respiratory drive (NRD) measured from the diaphragm electromyogram (EMGdi) reflects the load/capacity balance of the respiratory muscle pump and is a marker of lung disease severity. EMGdi measurement is invasive, but recording the EMG from the parasternal intercostal muscles using surface electrodes (sEMGpara) could provide a non-invasive method of assessing NRD and disease severity.
Objectives To test the hypothesis that NRD measured by sEMGpara correlates with EMGdi, to provide an index of disease severity in cystic fibrosis (CF) and to relate to exercise-induced breathlessness.
Methods 15 patients with CF (mean forced expiratory volume in 1 s (FEV1) 53.5% predicted) and 15 age-matched healthy controls were studied. sEMGpara and EMGdi were recorded at rest and during exercise. sEMGpara was recorded using surface electrodes and EMGdi using a multipair oesophageal electrode catheter. Signals were normalised using the peak EMG recorded during maximum respiratory manoeuvres and expressed as EMG%max. The respiratory pattern, metabolic data, oesophageal and gastric pressures and Borg scores were also recorded.
Results Mean (SD) resting sEMGpara%max and EMGdi%max were higher in patients with CF than in controls (13.1 (7)% and 18.5 (7.5)% vs 5.8 (3)% and 7.5 (2)%, respectively, p<0.001). In the patients with CF, resting sEMGpara%max and EMGdi%max were related to the degree of airways obstruction (FEV1) (r=−0.91 and r=−0.82, both p<0.001), hyperinflation (r=0.63 and r=0.56, both p<0.001) and dynamic lung compliance (r=−0.53 and r=−0.59, both p<0.001). During exercise, sEMGpara%max and EMGdi%max were strongly correlated with breathlessness in the patients with CF before (r=0.906, p<0.001) and after (r=0.975, p<0.001) the onset of neuromechanical dissociation.
Conclusion sEMGpara%max provides a non-invasive marker of neural drive, which reflects disease severity and exercise-induced breathlessness in CF.
- Cystic fibrosis
- exercise
- respiratory measurement
- respiratory muscles
Statistics from Altmetric.com
Introduction
Cystic fibrosis (CF) is characterised by a chronic progressive and irreversible loss of pulmonary function, with the main cause of death being respiratory failure. A predominant clinical feature of CF is airways obstruction, precipitated by abnormal mucus production and the persistent negative cycle of infection and inflammation.1 2 Forced expiratory volume in 1 s (FEV1) and the rate of its decline in CF are currently the best independent predictors of survival.3–5 Maintenance of lung function is an important therapeutic goal in the treatment and management of CF.
Physiological abnormalities associated with CF include increased airway resistance and altered chest wall and respiratory muscle geometry as a consequence of hyperinflation.6 7 In severe disease there is also a restrictive defect. The diaphragm electromyogram (EMGdi) provides a sensitive real-time breath-by-breath measure of neural respiratory drive (NRD) which reflects the load on the respiratory muscles.8 When expressed as a percentage of the maximum EMG obtained from volitional manoeuvres (EMGdi%max), it has been shown to be a marker of disease severity in chronic obstructive pulmonary disease (COPD).8
The measurement of NRD in patients with CF could provide useful information regarding disease severity and progression, and potentially be a useful objective measure of the effect of treatments. Measurement of NRD using EMGdi is invasive, which limits its clinical application. The parasternal intercostal muscles are obligatory inspiratory muscles9 and recording the EMG from these muscles using surface electrodes (sEMGpara) could provide a non-invasive method to assess NRD. Increased parasternal intercostal EMG activity has been observed in children with asthma10 and during loaded breathing in healthy subjects and patients with COPD.11
We hypothesised that NRD, measured by sEMGpara, would reflect NRD as measured by EMGdi in healthy subjects and patients with CF. Measurement of NRD using EMGdi and non-invasively with sEMGpara could provide accurate information on disease severity and correlate with pulmonary function tests. We further hypothesised that the alterations in lung mechanics that occur in patients with CF during exercise would lead to progressive attenuation of the translation of NRD to ventilation (neuromechanical dissociation), and NRD would be more closely correlated with breathlessness than respiratory pressures or flow.
Methods
Additional detail on the methods is provided in the online data supplement.
Subjects
Healthy adult subjects and clinically stable patients with CF were studied. The study was approved by King's College Hospital ethics committee and all participants provided written informed consent.
Measurements
sEMGpara and EMGdi were recorded at rest and during exercise in all subjects. sEMGpara was recorded using bipolar surface electrodes.11 EMGdi was recorded from the crural diaphragm using a multipair oesophageal electrode catheter consisting of nine consecutive coils forming five recording electrode pairs.8 EMG signals were amplified and band pass filtered (10 Hz to 3 kHz) and acquired by computer with analogue to digital sampling at 2 kHz. Peak root mean square per breath was calculated and averaged over 1 min. EMG recordings at rest and during exercise were normalised to the EMG signal obtained during a maximal volitional manoeuvre. Four different maximal volitional manoeuvres were performed: inspiratory capacity (IC), maximal static inspiratory pressure (PImax), maximal sniff pressure and maximal voluntary ventilation for 15 s (MVV).8 Each manoeuvre was repeated five times and, irrespective of manoeuvre, the numerically largest EMG signal was used for normalisation.
Respiratory flow was measured using either a mouthpiece during resting tidal breathing or via a full-face mask during exercise attached to a pneumotachograph. Airway pressure was measured using a differential pressure transducer. Transdiaphragmatic pressure (Pdi) was measured using a dual pressure transducer tipped catheter with the proximal pressure transducer positioned in the mid oesophagus (oesophageal pressure, Poes) and the distal transducer in the stomach (gastric pressure, Pgas). Flow and pressure signals were recorded and displayed in real time on a computer. Tidal volume was obtained by digital integration of the flow signal and Pdi by digital subtraction of Poes from Pgas. The diaphragm (PTPdi) and oesophageal (PTPoes) pressure–time product12 13 and tension time index (TTI)14 15 were measured.
Protocol
On the day of testing, spirometry16 and respiratory muscle strength17 were measured in all subjects. Lung volumes were also measured in the patients with CF. The EMG and pressure catheters were inserted and EMGdi and sEMGpara were measured in conjunction with respiratory flow at rest and during the standardised maximal spontaneous volitional manoeuvres. In 10 healthy subjects the four maximal respiratory manoeuvres used to normalise the parasternal intercostal EMG were repeated on two separate occasions at least 24 h apart.
Subjects performed an incremental cycle exercise test to exhaustion on an electrically braked cycle ergometer and metabolic data were recorded. Work rate was increased by 25 watts in the patients with CF and 50 watts in the healthy subjects every 3 min, starting with unloaded cycling. Subjects maintained 50–60 revolutions/min. IC measured from the functional residual capacity and breathlessness measured using the modified Borg scale were recorded at the end of each minute.18
Data analysis
All data except the Borg score and work rate were normally distributed and expressed as mean and SD. Work rate and Borg scores were expressed as median and interquartile range (IQR). Differences between healthy subjects and patients with CF were assessed using unpaired t tests for all variables except work rate and Borg scores which were compared using the Mann–Whitney test. The association between sEMGpara%max, EMGdi%max and lung function was examined using Pearson correlation coefficients. The associations between Borg breathlessness scores and measured variables during exercise were examined using Spearman correlation coefficients. Reproducibility of sEMGpara was assessed by paired t test, coefficient of variation and Bland–Altman analysis.19 Bland–Altman analysis was also used to investigate the relationship between the degree of diaphragm and parasternal EMG recruitment during exercise. Statistical analysis of the data was performed using Graph Pad Prism V.5.02 for Windows (San Diego, California, USA). A p value <0.05 was considered statistically significant, except for correlation analysis to investigate the relationship between Borg breathlessness scores and measured variables for which a p value <0.01 was used to allow for the number of comparisons performed.
Results
Subjects
Fifteen patients of mean (SD) age 24 (5.5) years with CF (FEV1 53.5 (24)% predicted) and 15 healthy subjects of mean (SD) age 25 (3) years were studied. The anthropometric characteristics, lung volumes, respiratory muscle strength and resting levels of NRD for the healthy subjects and patients with CF are summarised in tables 1 and 2.
Anthropometric characteristics and pulmonary function variables for healthy subjects and patients with cystic fibrosis
Respiratory muscle strength and resting levels of neural respiratory drive measured in healthy subjects and patients with cystic fibrosis (CF)
Rest
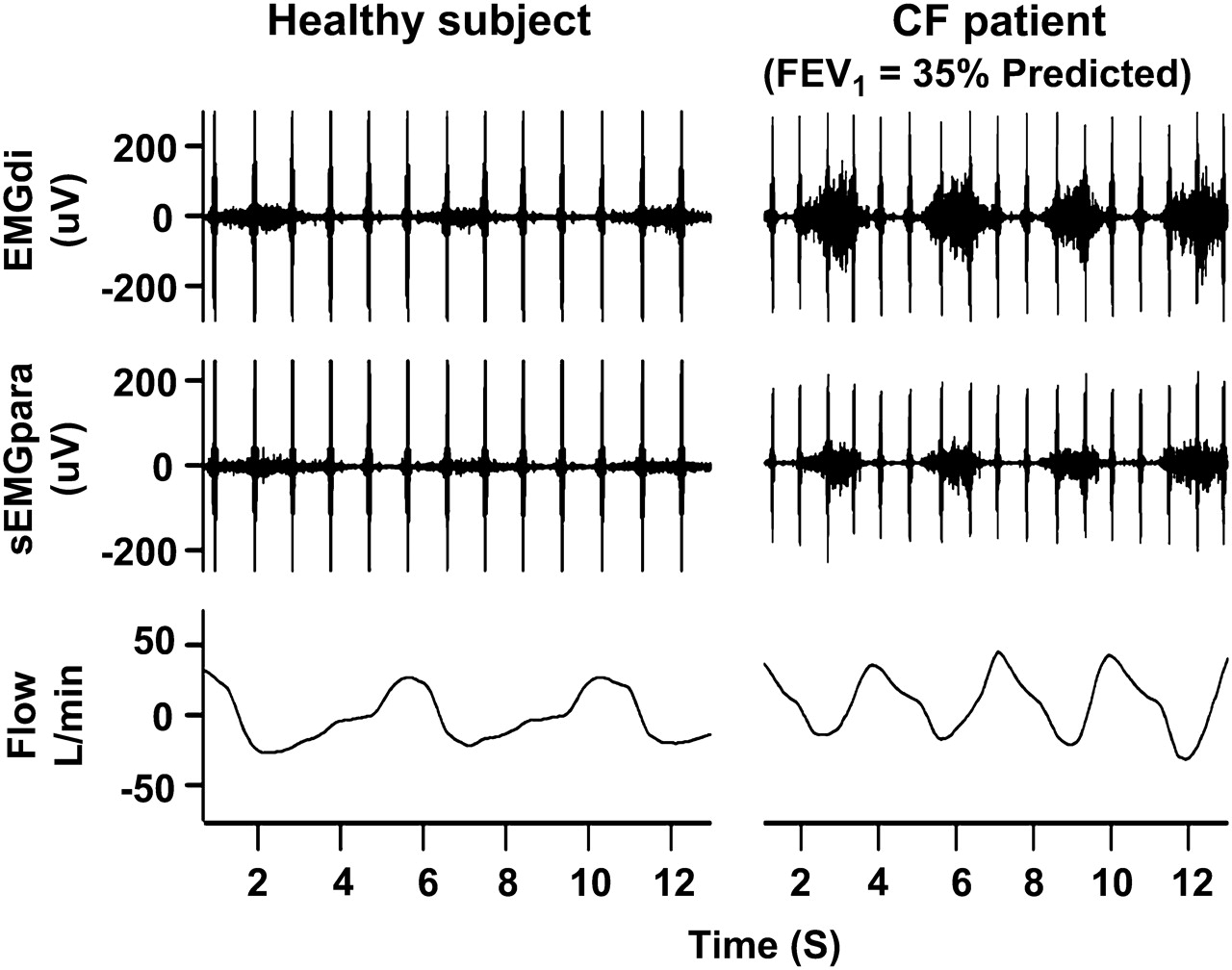
Clear phasic inspiratory activity of sEMGpara and EMGdi was observed during tidal resting breathing in all subjects (figure 1). Resting sEMGpara%max and EMGdi%max were higher in patients with CF than in healthy controls (table 2; figure 2). The patients with CF generated a smaller tidal volume percentage predicted VC per unit sEMGpara% max and EMGdi% max than the healthy controls at rest (table 2).
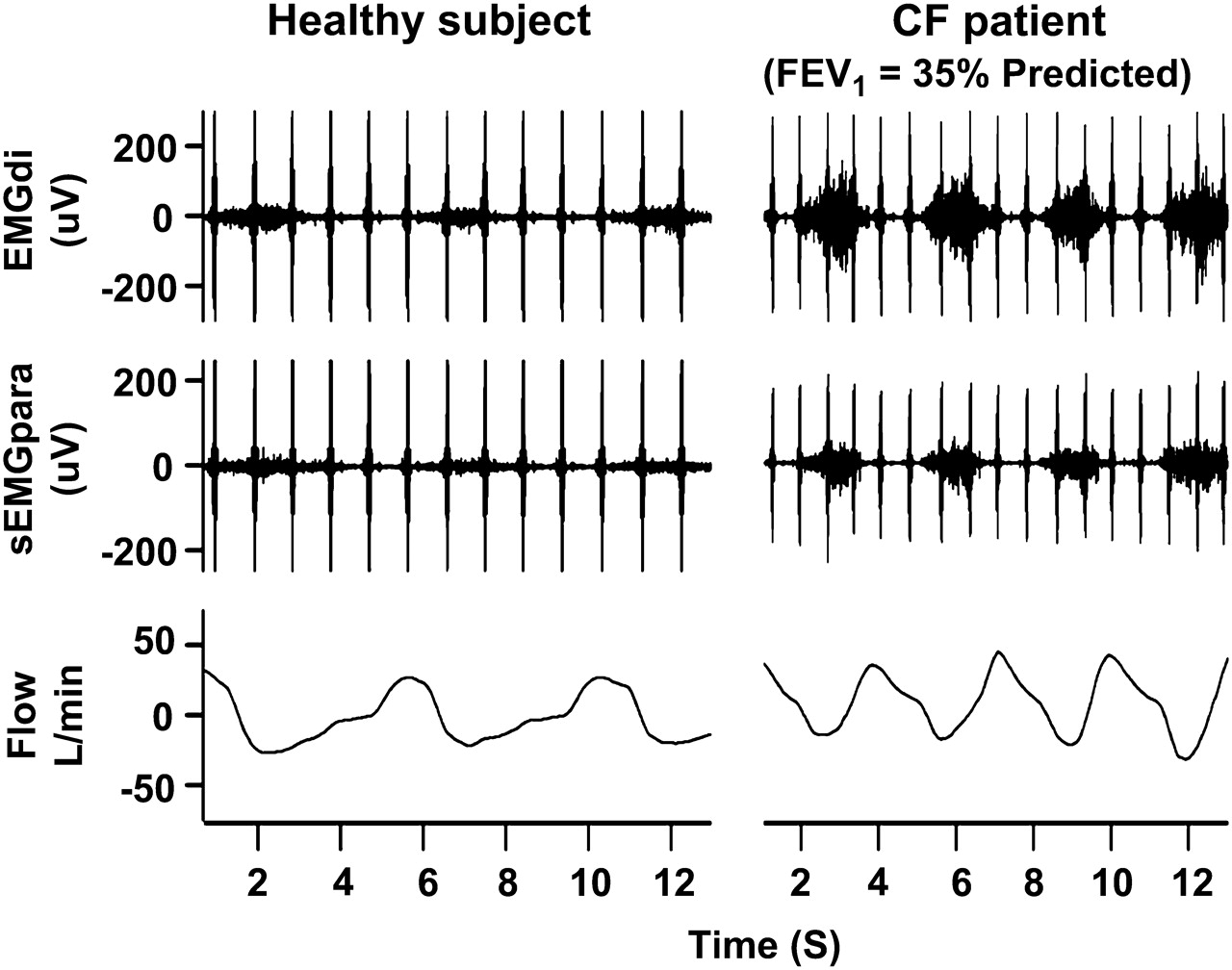
Representative trace of diaphragm electromyogram (EMGdi), surface parasternal intercostal EMG (sEMGpara) and respiratory flow (inspiration negative) recorded during resting tidal breathing in a healthy subject and a patient with cystic fibrosis (CF). FEV1, forced expiratory volume in 1 s.

Neural respiratory drive measured as (A) parasternal electromyogram (EMG) activity normalised to the maximal EMG evoked during maximal inspiratory manoeuvres (sEMGpara%max) and (B) diaphragm EMG activity normalised to the maximal EMG evoked during maximal inspiratory manoeuvres (EMGdi%max) during resting tidal breathing in 15 patients with cystic fibrosis (CF) and 15 healthy subjects. Comparisons made using the unpaired t test. Horizontal bars are means.
Resting sEMGpara% max was correlated with resting EMGdi%max for all subjects (r=0.829, p<0.001). In the patients with CF, resting sEMGpara%max and EMGdi%max were best correlated with FEV1% predicted (r=−0.829, p<0.001; r=−0.739, p<0.002; table 3; figure 3).
Association between sEMGpara%max, EMGdi%max recorded during tidal resting breathing and lung function measured in 15 patients with cystic fibrosis
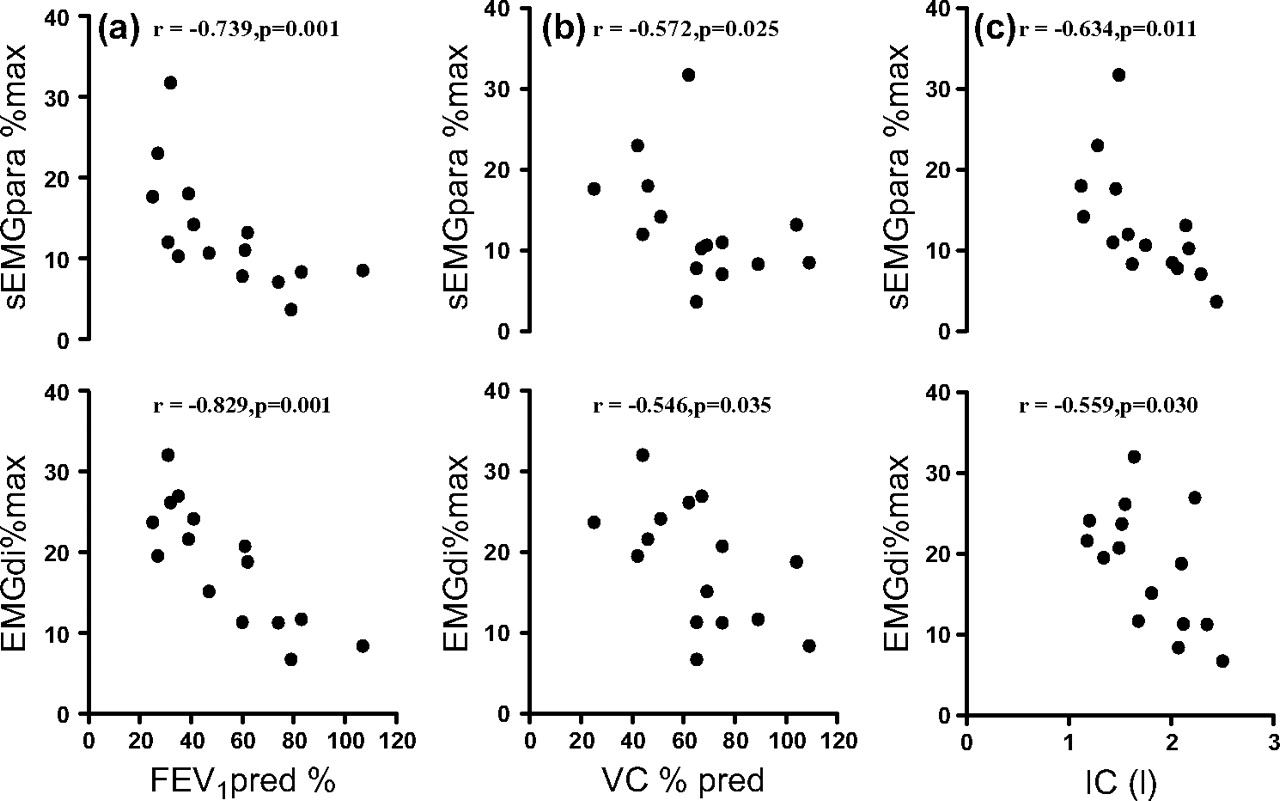
Relationships between normalised surface parasternal intercostal electromyogram (sEMGpara%max), diaphragm EMG (EMGdi%max) and (A) forced expiratory volume in 1 s percentage predicted (FEV1% pred), (B) vital capacity percentage predicted (VC% pred) and (C) inspiratory capacity (IC) in 15 patients with cystic fibrosis.
Reproducibility
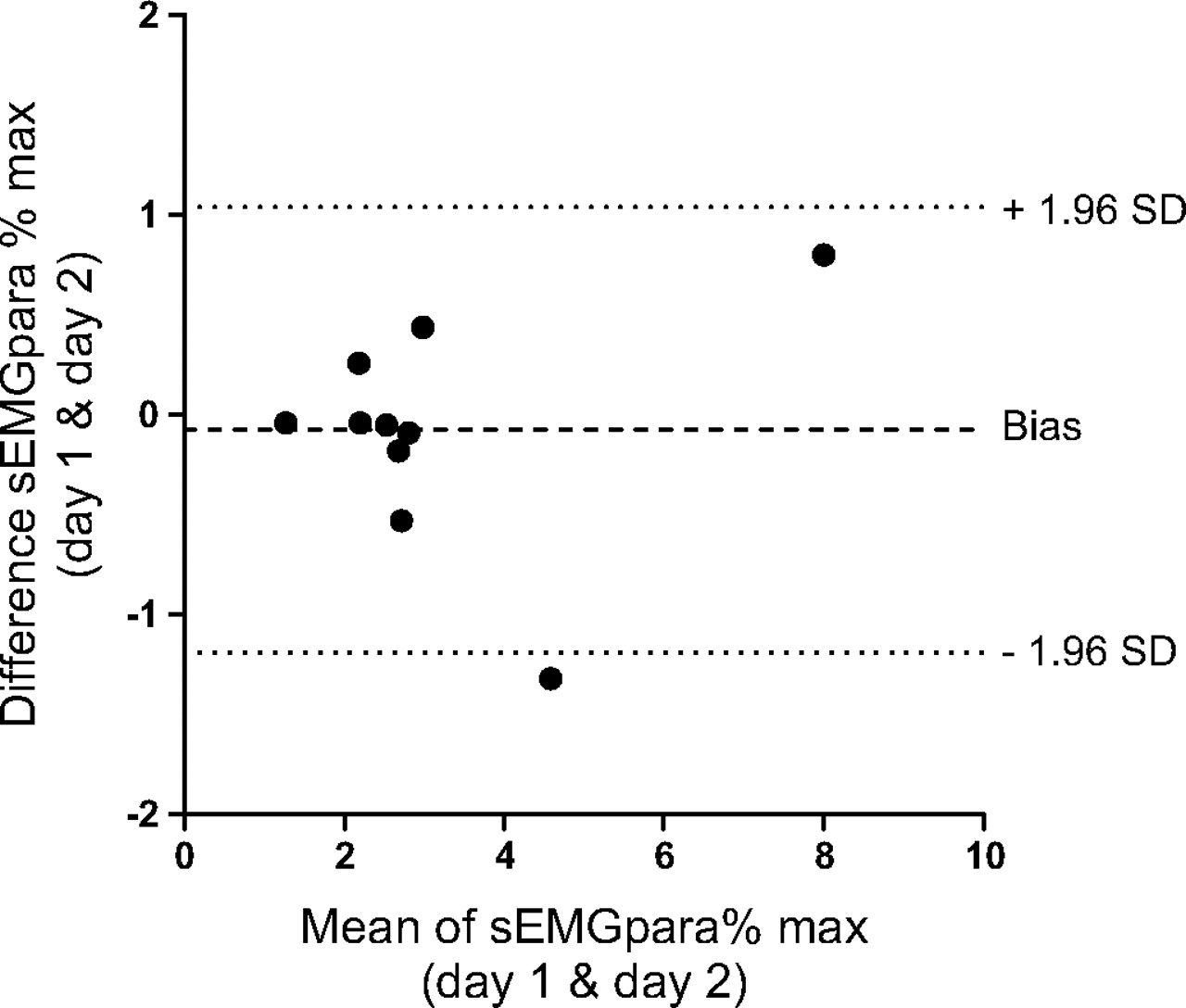
There was no significant difference in the raw values (μV) of sEMGpara measured at rest and during the maximal inspiratory manoeuvres on the two separate occasions. The mean inter-occasion coefficient of variation for the raw resting sEMGpara was 0.05 (0.04) μV and the normalised sEMGpara%max was 0.05 (0.04)%. The mean inter-occasion coefficients of variation for the four maximal respiratory manoeuvres were: PImax 0.08 (0.06); sniff 0.06 (0.03); total lung capacity 0.11 (0.06) and MVV 0.12 (0.06). On both occasions maximal parasternal EMG activity was elicited in eight of the healthy subjects by the sniff manoeuvre and in two by PImax. The mean (SD) inter-occasion difference for all healthy subjects for resting sEMGpara%max was 0.07 (0.5)% with 95% limits of agreement −1.19% to 1.04%. A greater degree of inter-occasion variability in resting sEMGpara%max was observed in two healthy subjects in whom resting NRD was markedly greater than the rest of the cohort (figure 4).19 The inter-occasion variability in resting sEMGpara%max in these two subjects was 0.12 and 0.05.
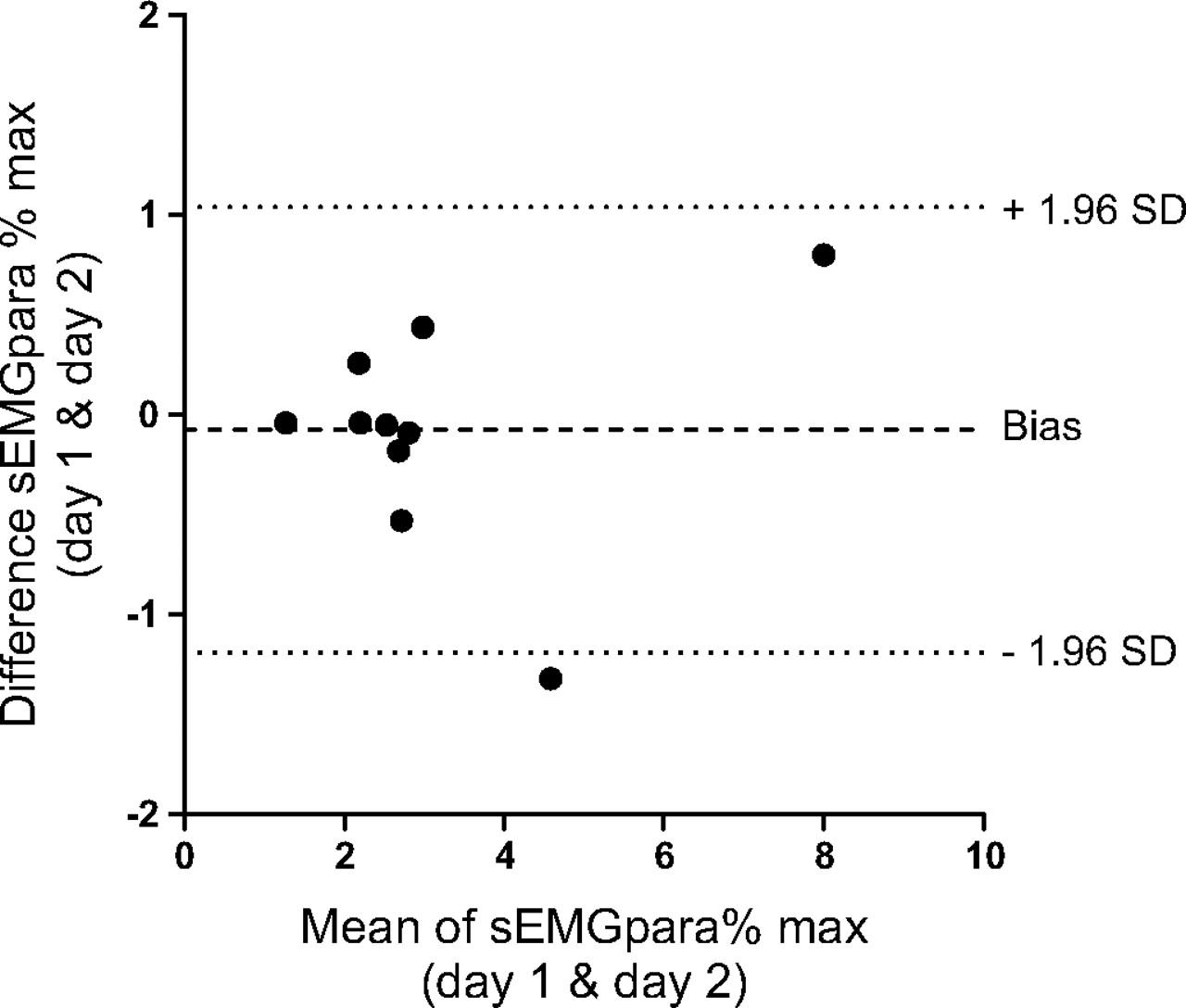
Bland–Altman analysis of the reproducibility of the normalised resting surface parasternal intercostal electromyogram (sEMGpara%max) on two different occasions in 10 healthy subjects (bias −0.075%, SD of bias 0.57%, 95% limits of agreement −1.19% to 1.04%).
Exercise
Exercise time was similar in the healthy subjects and patients with CF (21 (4) min vs 20.5 (5) min, p=0.690). The healthy subjects achieved a higher maximum work rate (250 (250–275) watts vs 125 (100–150) watts, p<0.001) and peak oxygen consumption/kg (38.5 (11) vs 28 (8) ml/min/kg, p=0.008) than the patients with CF.
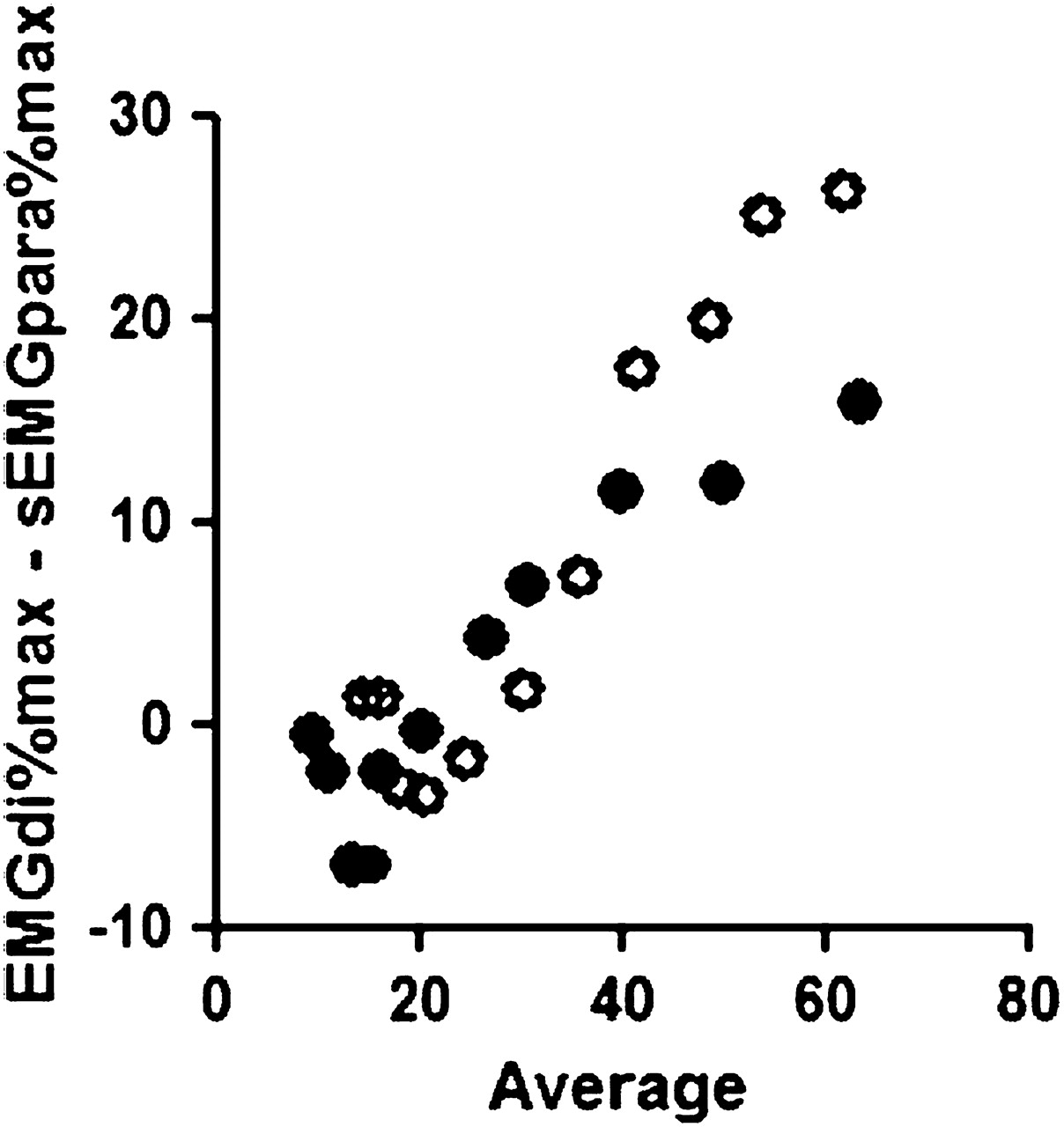
In both groups the phasic sEMGpara and EMGdi activity progressively increased with exercise intensity. There was no difference between healthy subjects and patients with CF in end exercise NRD as measured by sEMGpara%max (48.6 (20)% vs 55.3 (27)%, p=0.440) or EMGdi%max (74.9 (18.5)% vs 71.2 (15)%, p=0.550). To assess whether the sEMGpara%max could be used as a surrogate maker of the neural drive to the diaphragm, Bland–Altman analysis was performed (figure 5). Our results indicate that the magnitude of change in the diaphragm during exercise was significantly greater than that of the parasternal intercostal muscles and therefore the two measures of NRD are not interchangeable.

Bland–Altman analysis of the degree of diaphragm electromyogram (EMGdi%max) and parasternal intercostal electromyogram (sEMGpara%max) activation during exercise in healthy subjects (open circles) (bias 2.7%, SD of bias 7.7, 95% limits of agreement −12% to 18%) and patients with cystic fibrosis (solid circles) (bias 8.4%, SD of bias 11.5%, 95% limits of agreement −14% to 31%).
In the healthy subjects sEMGpara%max was strongly correlated with EMGdi%max measured during exercise (r=0.964, p<0.001) and increased in tandem with diaphragm pressure–time product (PTPdi), minute ventilation (MV) and breathlessness (figure 6). Borg breathlessness scores were correlated with all measured variables (table 4).
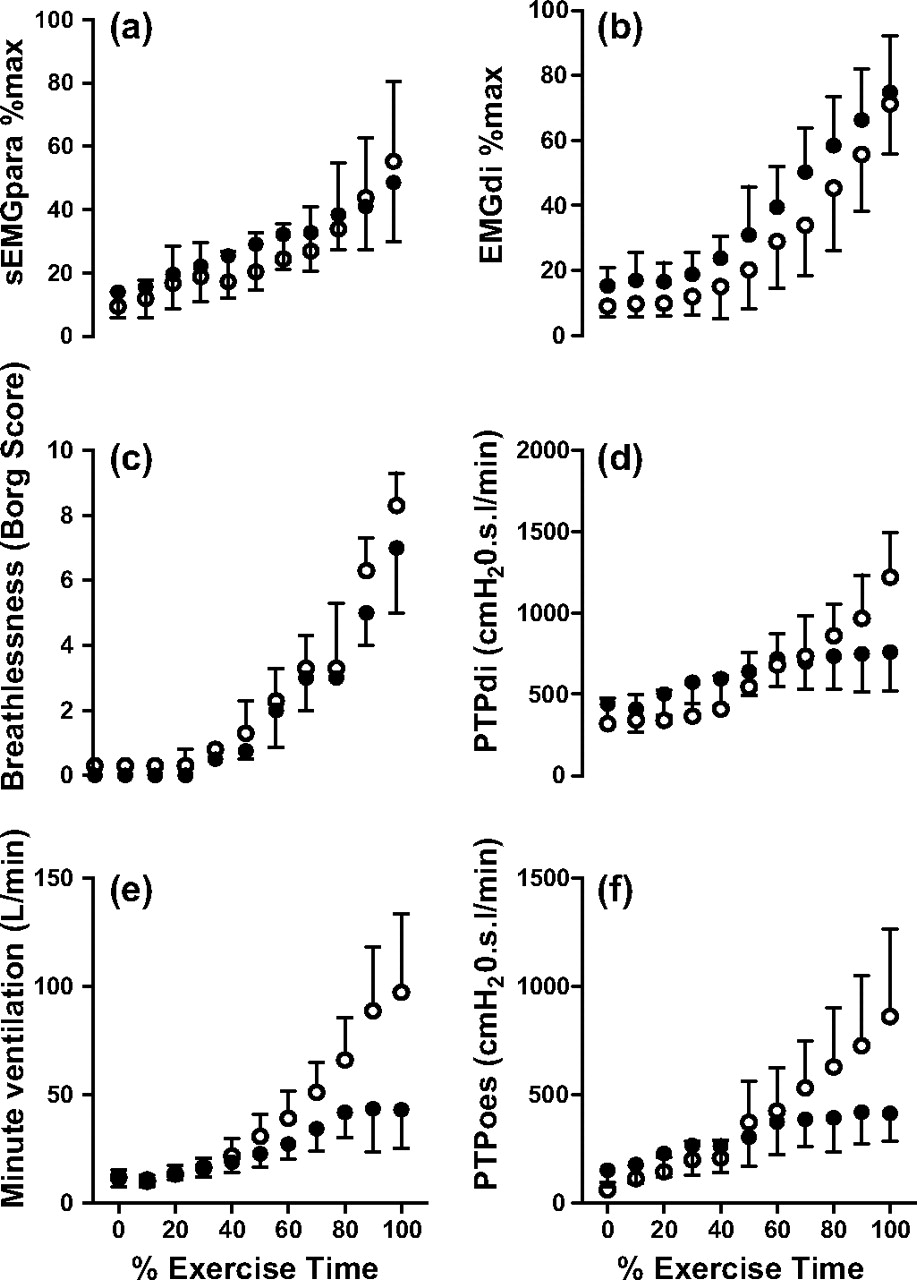
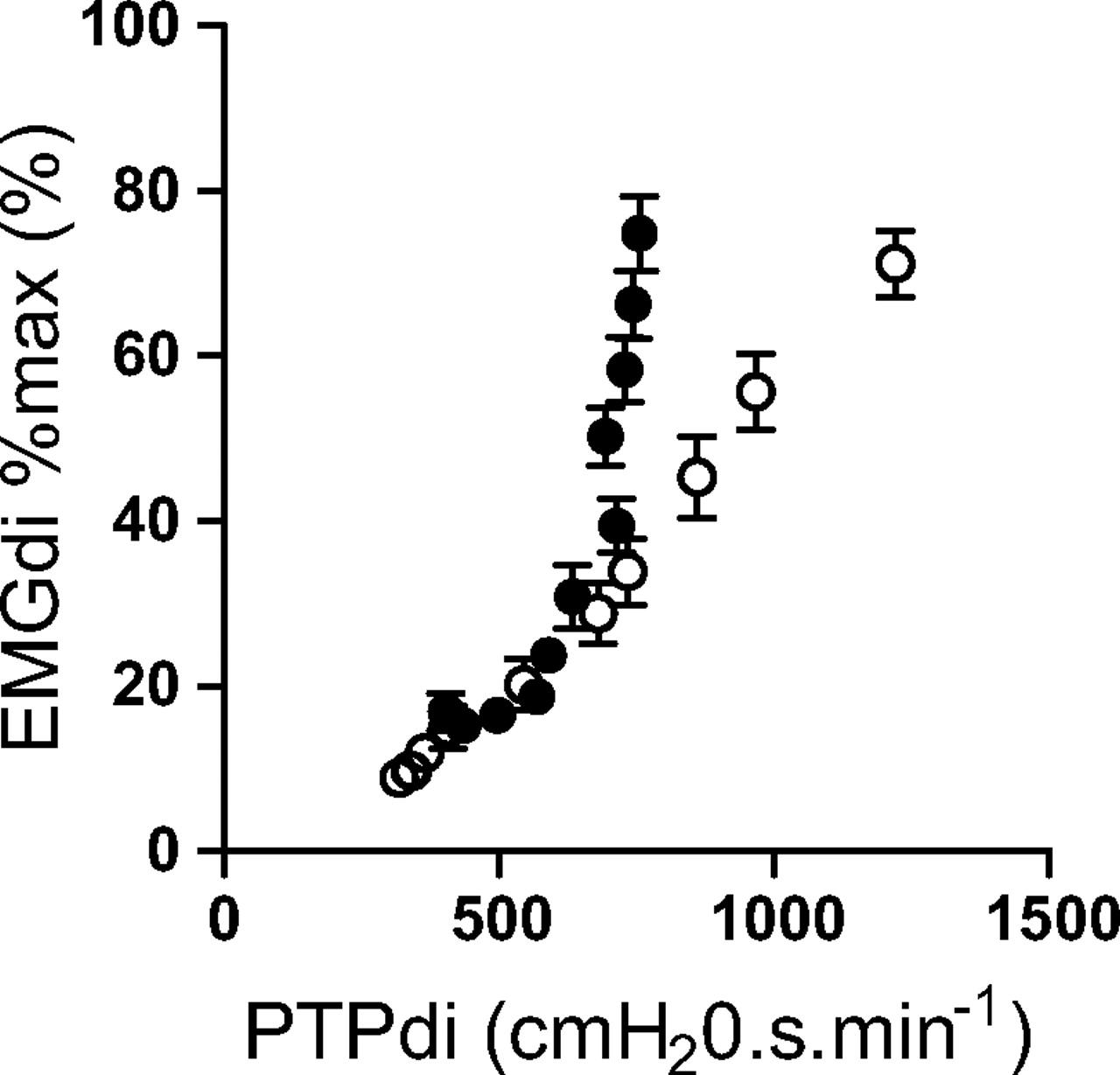
(A) Normalised surface parasternal intercostal electromyogram (sEMGpara%max), (B) normalised diaphragm electromyogram (EMGdi%max), (C) Borg scores, (D) diaphragm pressure–time product (PTPdi), (E) minute ventilation (MV) and (F) oesophageal pressure–time product (PTPoes) measured during exercise to exhaustion in 15 healthy subjects (open circles) and 15 patients with cystic fibrosis (closed circles). Data are expressed as mean and SD, with the exception of Borg scores which are expressed as median and interquartile range.
Association between Borg breathlessness scores and measured variables during exercise to exhaustion in 15 healthy subjects
In the patients with CF, sEMGpara%max was strongly correlated with EMGdi%max (r=0.955, p<0.001) measured during exercise and increased in parallel with Borg breathlessness scores but not PTPdi, PTPoes or MV (figure 6), indicating neuromechanical dissociation (figure 7). Unlike the healthy subjects, the patients with CF became progressively more hyperinflated during exercise as shown by the decrease in IC from the start to the end of exercise (CF: 1.9 (0.5) l at start vs 1.4 (0.4) l at end, p=0.019; healthy subjects: 3.2 (0.85) l at start vs 3.4 (0.75) l at end, p=0.678). Significant increases were observed in end expiratory lung volume in the patients with CF early in exercise at a median (IQR) work rate of 25 (0–25) watts (p=0.008)20 21 which occurred at approximately the eighth minute of exercise (40% of total exercise time).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Normalised diaphragm electromyogram (EMGdi%max) plotted against diaphragm pressure–time product (PTPdi) reflecting neuromechanical coupling during exercise to exhaustion in 15 healthy subjects (open circles) and 15 patients with cystic fibrosis (closed circles). Data are expressed as mean and SD.
To investigate the relationship between NRD, ventilatory variables and breathlessness in the patients with CF, we subdivided the exercise data into two phases—before and after the onset of neuromechanical dissociation. The onset of neuromechanical dissociation was defined as an increase of <10% in the PTPdi between exercise time points. This point occurred at approximately 70% of the total exercise time. Following the onset of neuromechanical dissociation, EMGdi%max and sEMGpara%max remained strongly correlated with breathlessness (tables 5 and 6).
Association between Borg breathlessness scores and measured variables during exercise in 15 patients with cystic fibrosis before the onset of neuromechanical dissociation (rest to 60% of total exercise time)
Association between Borg breathlessness scores and measured variables during exercise in 15 patients with cystic fibrosis following the onset of neuromechanical dissociation (70% of total exercise time to exhaustion)
Discussion
The main finding of this study is that sEMGpara%max and EMGdi%max provide similar NRD data in healthy subjects and patients with CF both at rest and during exercise. Patients with the most severe disease had the greatest sEMGpara%max and EMGdi%max. During high levels of exercise, sEMGpara%max and EMGdi%max were strongly correlated with breathlessness in the patients with CF following the onset of neuromechanical dissociation due to dynamic hyperinflation.
Critique of the method
A limitation of surface EMG recordings is the inherently poor between-subject and between-occasion reproducibility owing to variations in electrical contact and electrode position relative to the underlying muscle. One of our healthy subjects had a sEMGpara%max inter-occasion coefficient of variation of 0.12; on closer examination this was found to be due to variability in their maximal evoked EMG rather than variation in their resting level of sEMGpara. This highlights the importance of familiarising subjects with the normalising techniques and ensuring that truly maximal volitional efforts are made. Normalising the parasternal intercostal EMG to that evoked during a maximal respiratory manoeuvre provides a reproducible non-invasive measure of the load on the respiratory muscles relative to their capacity which is comparable between patients on different occasions.
In this study there was increased sEMGpara%max and EMGdi%max at rest in the patients with CF compared with the healthy subjects. This increased EMG activity reflected the increased motor neuron firing frequency in response to the load on the inspiratory muscles as a consequence of the disease. This has previously been demonstrated in the parasternal intercostal muscles22 and the diaphragm23 using invasive needle electrodes in patients with COPD.
Electromyography using surface electrodes can be directly affected by underlying levels of subcutaneous fat. Neither our patients nor the controls were overweight, but we accept that sEMGpara%max cannot be assumed to be a reliable technique in overweight patients based on our present data, although we have previously shown that EMGdi%max is an appropriate technique in obese subjects.24
Significance of the findings
As is well documented in COPD, the respiratory muscles of patients with CF are subject to an increased load due to airways obstruction. Hyperinflation as a consequence of gas trapping places these patients on the upper flattened portion of the pressure-volume curve, increasing the elastic work of breathing and causing the development of intrinsic positive end expiratory pressure, so imposing a load that needs to be overcome with each breath.6 Reduction in inspiratory muscle length and altered geometry as a consequence of hyperinflation reduce the ability of the inspiratory muscles to generate negative pressure.25 We have shown that this increased load in patients with CF is reflected in an increased sEMGpara%max and EMGdi%max and that NRD is proportional to the degree of airway obstruction (FEV1), hyperinflation (IC and RV/TLC) and dynamic lung compliance. This suggests that sEMGpara%max and EMGdi%max are good measures of respiratory disease severity in CF, and could potentially be of value in monitoring disease progression and assessing prognosis. NRD measures the load on the respiratory muscle pump and therefore it may better reflect overall lung disease severity than individual pulmonary function tests which only measure particular aspects of changing lung pathology (ie, FEV1 and airway obstruction).
This is the first study to describe levels of NRD in patients with CF quantified by both surface EMG recording from the parasternal intercostal muscles and transoesophageal EMG of the diaphragm. NRD measured as EMGdi%max has been reported as 9.0 (3.4)% in healthy subjects8 and between 27.9 (9.9)%8 and 43.4 (22)%26 in patients with COPD, depending on disease severity. The mean FEV1 in the patients with COPD studied by Jolley et al8 was 34.8% predicted while those studied by Sinderby et al26 was 28% predicted. Our measurements of EMGdi%max in healthy subjects (7.5 (2)%) and patients with CF (18.5 (7.5)%) are in keeping with these findings. The lower EMGdi%max observed in our patients with CF reflects their lesser disease severity in terms of lung function. In the current study, NRD measured non-invasively from sEMGpara%max was 5.8 (3)% in healthy subjects and 13.1 (7)% in patients with CF and was strongly correlated with EMGdi%max.
De Troyer et al suggested that activation of the parasternal intercostal muscles and the diaphragm depends on a common neural pathway or, alternatively, that their activation depends on different parallel pathways that are normally activated together.27 Furthermore, Gandevia et al have shown that, during tidal resting breathing, the timing of peak EMG activity for the diaphragm and parasternal intercostal muscle located in the second intercostal space is similar.28 In the current study although EMGdi%max and sEMGpara%max were strongly correlated at rest and during exercise, the pattern and the magnitude of recruitment was different between the diaphragm and parasternal intercostal muscles.
There was a marked contrast in the respiratory mechanics observed during exercise in the patients with CF compared with the healthy cohort. The work of breathing as indicated by the PTPdi in the patients with CF reached a plateau at approximately 70% of total exercise time, while NRD measured from sEMGpara%max and EMGdi%max continued to increase progressively up to the point of exercise termination. The plateau in PTPdi therefore cannot be attributed to central inhibition but rather to the inability of the diaphragm to generate pressure.29 The force-generating capacity of a muscle is dependent on its length.30 The dynamic hyperinflation that occurred during exercise in the patients with CF, as indicated by the fall in IC, acts to shorten the inspiratory muscles and alters their mechanical advantage, uncoupling NRD from pressure generation.29–31 It has been contended that hyperinflation is less detrimental to the parasternal intercostal muscles than the diaphragm.32 NRD as measured by sEMGpara%max and EMGdi%max was more closely correlated to breathlessness than mechanical outputs following the onset of neuromechanical dissociation.
Conclusion
sEMGpara%max provides a reproducible and non-invasive measure of NRD in healthy subjects and patients with CF. NRD is increased in patients with CF, reflecting disease severity, and is closely related to exercise-induced breathlessness. Potentially, sEMGpara%max could be a useful monitoring tool to assess disease progression and may prove to be a more sensitive measure than conventional lung function or exercise testing. It could also provide useful information on the effect of treatments.
References
Supplementary materials
Web Only Data thx.2010.142646
Files in this Data Supplement:
Footnotes
Funding CCR is supported by a Medical Research Council (London, UK) PhD studentship.
Competing interests None.
Ethics approval This study was conducted with the approval of King's College London.
Provenance and peer review Not commissioned; externally peer reviewed.