Article Text

Abstract
Multiple-breath washout (MBW)-derived lung clearance index (LCI) is a sensitive measure of ventilation inhomogeneity in patients with cystic fibrosis (CF), but LCI measurement is time consuming. We systematically assessed ways to shorten LCI measurements.
In 68 school-aged children (44 with mild CF lung disease) three standard nitrogen (N2) MBWs were applied. We assessed repeatability and diagnostic performance of (1) LCI measured earlier from three MBW runs and (2) LCI measured at complete MBW (1/40th of starting N2 concentration) from two runs only.
Compared with the standard LCI from three complete MBW runs, the new LCI based on three N2MBW runs until 1/20th, or two complete runs until 1/40th, provided similar or better repeatability as well as sensitivity and specificity for CF lung disease. Alternative ways to measure LCI reduced test duration in children with CF by 30% and 41%, respectively.
LCI measurements can be reliably shortened in children. These new MBW protocols may advance the transition of LCI from research into clinical settings.
- Cystic Fibrosis
- Paediatric Lung Disaese
- Lung Physiology
Statistics from Altmetric.com
Multiple-breath washout (MBW)-derived lung clearance index (LCI) is a sensitive measure of increased ventilation inhomogeneity in cystic fibrosis (CF) lung disease.1 ,2 However LCI is rarely measured routinely due to time-consuming protocols, that is, at least three MBW runs with tracer gas washout until 1/40th of its starting concentration.3 In this prospective study, we systematically assessed ways to shorten LCI measurements in school-aged children with CF, and in healthy controls.
We used a previously described nitrogen (N2) MBW equipment (Exhalyzer D, Eco Medics AG, Switzerland)4 and measured standard LCI (LCIstd) in 80 children (50 with CF) aged 5.7–16.9 years. Alternative MBW outcomes were (1) mean LCI derived from empirically chosen earlier time points based on three MBW runs and (2) mean LCI from two complete runs. Quality criteria for alternative LCI were defined as (1) predictive value (R2) for LCIstd>90%, (2) coefficient of variation (CV) ≤7% and (3) sensitivity and specificity for CF lung disease within ±3% of LCIstd (detailed in the online supplementary (OLS)).
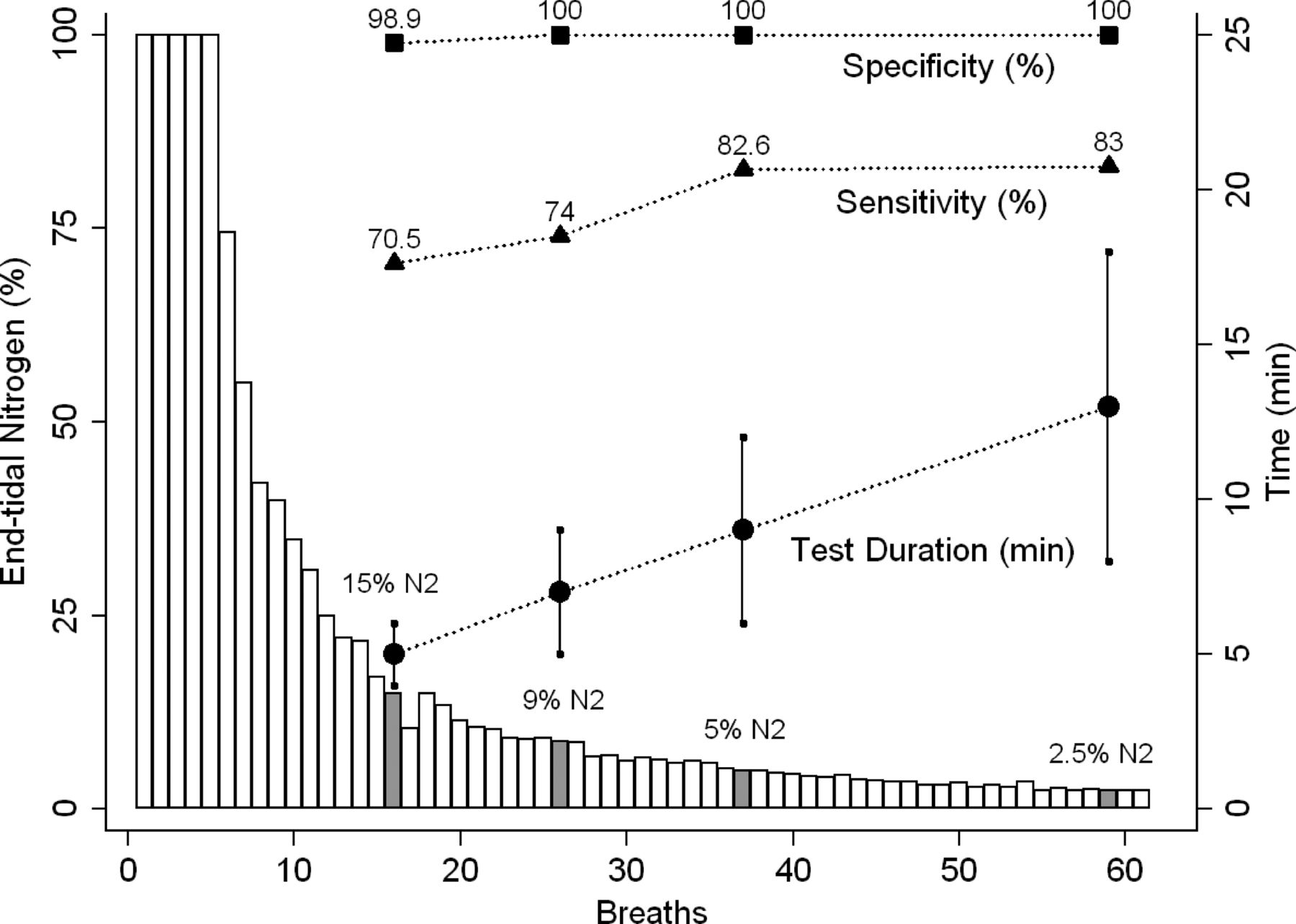
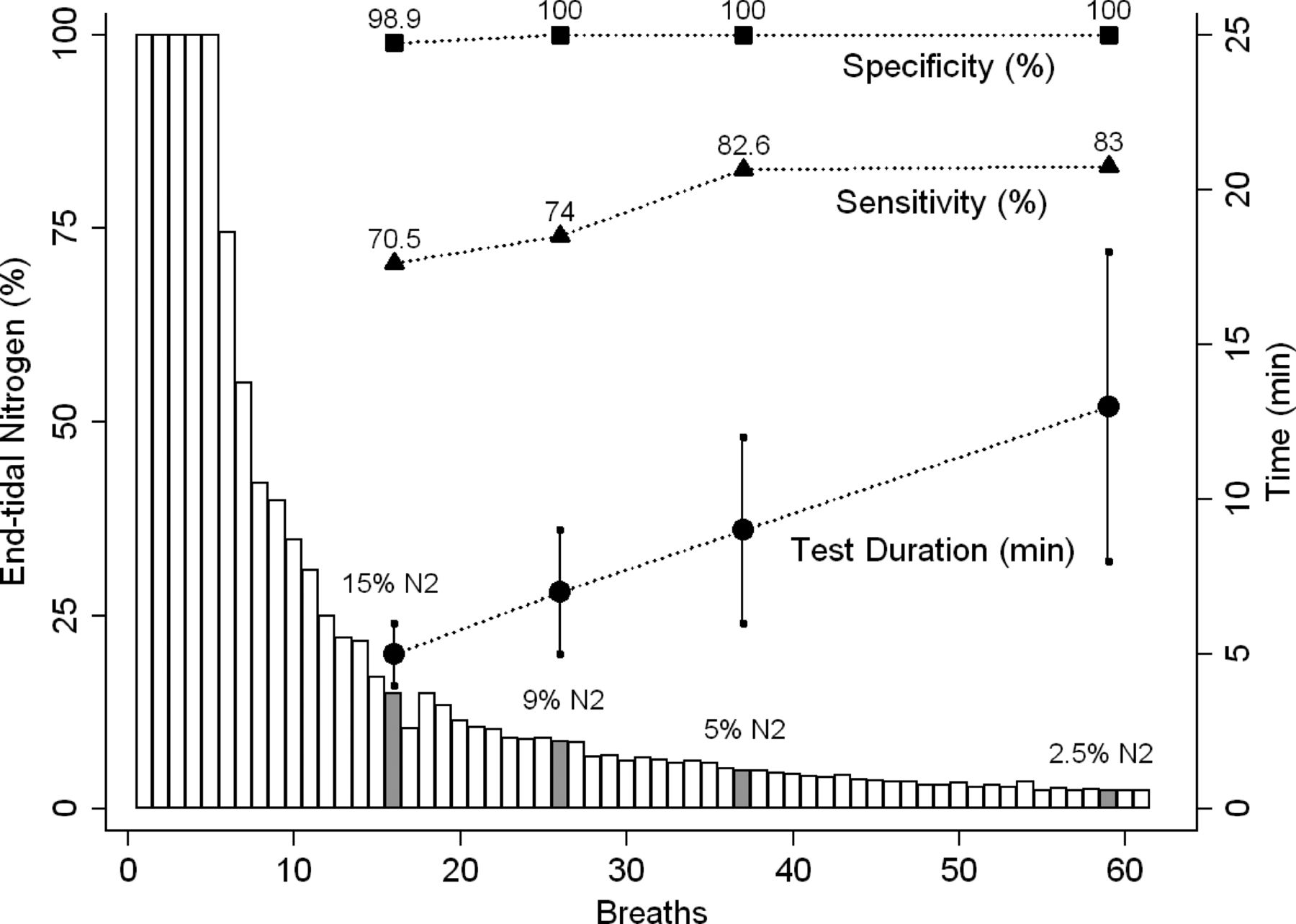
Technically acceptable triplicate N2MBW (n=204) were obtained in 68 (31 boys) children (44 with CF). N2MBW until 5% N2 (LCI5), that is, 1/20th of N2 starting concentration, was the earliest time point to meet all quality criteria (figure 1). LCI5 predicted 93% of LCIstd (table 1 and figure 1 OLS). CV of LCI5 was 5.1%, and 5.4% for LCIstd (table 2 OLS). LCI5 and LCIstd were both highly specific (100%), and provided a sensitivity of 82.6% and 83.0%, respectively, for CF lung disease (figure 1). Time savings were on average (95% CI) 3.7 (3.1–4.4) min. (30%) in CF. LCI from two complete runs also met the quality criteria and provided significant time savings (table 3 and figure 2 OLS). Detailed results and figures are given in the OLS.
{kind=link}
Diagnostic performance and duration of nitrogen multiple-breath washout. A typical example of a nitrogen multiple-breath washout (N2MBW) curve in a boy with cystic fibrosis schematically illustrates the course of diagnostic accuracy and test duration for the lung clearance index (LCI) measured at various time points (grey bars). End-tidal N2 concentration normalised to 100% (left y-axis) is plotted (white bars) against washout breaths (x-axis). By convention, N2MBW is performed until 1/40th (2.5% N2) of the N2 starting concentration to measure LCI. We calculated LCI at arbitrary earlier time points: 15%, 9% and 5% N2 (grey bars). Specificity (rectangles) and sensitivity (triangles) for CF lung disease increase over the washout. Mean±SD of test duration (right y-axis) are displayed as circles.
By convention, at least three MBW runs until 1/40th were recommended to measure LCI due to N2 sensor characteristics, estimated N2 blood gas exchange, and possibly due to lack of online quality control. We show that LCI measurements can be reliably shortened. Both new LCI measures may enhance feasibility and acceptance in younger children and in patients with more advanced lung disease. In children with predominantly mild CF lung disease, LCI based on two MBW runs seems attractive, as complete washout is usually achieved fast. This was confirmed in a retrospective study by Robinson et al5 where LCI of two complete runs adequately identified increased ventilation inhomogeneity in CF. LCI5 may be more applicable in advanced lung disease where complete N2MBW is time consuming. Further studies are needed to establish the applicability of shortened MBW for different populations and settings. Long-term repeatability and response to intervention need to be compared between shortened MBW protocols. Detailed discussion on methodological and physiological aspects are provided in the OLS.
Both new LCI measures based on three N2MBW runs until 1/20th, or two runs until 1/40th, significantly shorten MBW in children without compromising diagnostic performance for increased ventilation inhomogeneity in mild CF lung disease. These data support the transition of LCI measurement from research into clinical routine.
Acknowledgments
The authors would like to thank all children and their families for their participation in the study. The authors would like to express their thankfulness to Urs Frey, Per Gustafsson and Paul Robinson for their valuable input, and to Carmen Casaulta, Martin Schoeni and Nicolas Regamey for their patient care. We express our gratitude to Elisabeth Kieninger, Anne Schmidt, Elena Proietti, Oliver Fuchs, Sandra Luescher, Nicole Martin Santschi and Ruth Stauffer Lacorcia, for their valuable work and support.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
Footnotes
-
Contributors SY and FS contributed equally. Conceived and designed the experiments: FS SY CA MR PL. Performed the experiments: FS SY CA. Analysed the data: SY FS. Contributed reagents/materials/analysis tools: MR. Wrote the paper: FS SY. Qualified as the guarantor of the paper, took responsibility for the integrity of the work as a whole, from inception to published article: PL.
-
Funding The work for this report was funded by the Swiss Society for Cystic Fibrosis (CFCH), the Bernese Lung Association (Lungenliga Bern) and the Gottfried und Julia Bangerter-Rhyner-Stiftung. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
-
Competing interests None of the five authors has any conflicts of interest to disclose.
-
Patient consent Obtained.
-
Ethics approval Ethics Committee of the Canton of Bern, Switzerland (Kantonale Ethikkommission Bern).
-
Provenance and peer review Not commissioned; externally peer reviewed.