Article Text

Abstract
Background: Reactive nitrogen species (RNS) are thought to be one of the important factors in the pathogenesis of chronic obstructive pulmonary disease (COPD). A study was undertaken to examine the effects of theophylline and fluticasone propionate (FP) on RNS production in subjects with COPD.
Methods: Sixteen COPD subjects participated in the study. Theophylline (400 mg/day orally) or FP (400 μg/day inhalation) were administered for 4 weeks in a randomised crossover manner with a washout period of 4 weeks. Induced sputum was collected at the beginning and end of each treatment period. 3-nitrotyrosine (3-NT), which is a footprint of RNS, was quantified by high performance liquid chromatography with an electrochemical detection method as well as by immunohistochemical staining.
Results: Theophylline significantly reduced the level of 3-NT in the sputum supernatant as well as the number of 3-NT positive cells (both p<0.01). FP also reduced 3-NT formation, but the effect was smaller than that of theophylline. Theophylline also significantly reduced the neutrophil cell counts in the sputum (p<0.01), while FP treatment had no effect on the number of inflammatory cells in the sputum, except eosinophils.
Conclusions: Theophylline reduces nitrative stress and neutrophil infiltration in COPD airways to a larger extent than inhaled corticosteroid.
- COPD, chronic obstructive pulmonary disease
- FEV1, forced expiratory volume in 1 second
- FP, fluticasone propionate
- FVC, forced vital capacity
- HDAC, histone deacetylase
- HPLC/ECD, high performance liquid chromatography with electrochemical detection
- IL, interleukin
- 3-NT, 3-nitrotyrosine
- RNS, reactive nitrogen species
- chronic obstructive pulmonary disease
- nitrative stress
- 3-nitrotyrosine
- inhaled corticosteroid
- theophylline
- histone deacetylase
- peroxynitrite
Statistics from Altmetric.com
- COPD, chronic obstructive pulmonary disease
- FEV1, forced expiratory volume in 1 second
- FP, fluticasone propionate
- FVC, forced vital capacity
- HDAC, histone deacetylase
- HPLC/ECD, high performance liquid chromatography with electrochemical detection
- IL, interleukin
- 3-NT, 3-nitrotyrosine
- RNS, reactive nitrogen species
- chronic obstructive pulmonary disease
- nitrative stress
- 3-nitrotyrosine
- inhaled corticosteroid
- theophylline
- histone deacetylase
- peroxynitrite
Airway inflammation is the pathophysiological feature of chronic obstructive pulmonary disease (COPD). Although a number of cells and mediators are involved in the pathophysiology of COPD, neutrophilic airway inflammation1–4 and oxidative stress5,6 in the lung are thought to play an important part in its development.
Reactive oxygen/nitrogen species (ROS/RNS) have a potent pro-inflammatory action7 causing airway inflammation,8 and therefore are thought to be one of the important factors in the pathogenesis of COPD, which results in airway epithelial injury, neutrophil migration and protease/antiprotease imbalance.9 3-Nitrotyrosine (3-NT) is a footprint of RNS. We have previously shown that the number of 3-NT positive cells and the level of 3-NT are increased in COPD airways, and these increases are correlated with the airflow limitation of COPD.10,11 These data strongly suggest that ROS/RNS could have a key role in the pathogenesis of COPD, and that a reduction in ROS/RNS would lead to an anti-inflammatory effect.
More recently we have shown that inhaled corticosteroid can cause a small but significant reduction in RNS production in COPD airways.12 On the other hand, a recent paper has reported that theophylline reduces the number of neutrophils via a reduction of interleukin (IL)-8 in COPD airways.13 However, it is still unclear whether theophylline can suppress nitrative stress in COPD airways.
This study was undertaken to assess the anti-inflammatory effects of oral theophylline and inhaled corticosteroid in COPD using a crossover design. Neutrophilic airway inflammation and production of RNS were quantified by measuring 3-NT immunoreactivity in induced sputum. In addition, in order to evaluate the production of RNS in COPD airways in more detail, the levels of 3-NT were measured using high performance liquid chromatography (HPLC) with electrochemical detection (HPLC/ECD) analysis.
METHODS
Subjects
Sixteen patients with COPD regularly visiting Wakayama Medical University Hospital were recruited after giving informed consent. All patients satisfied the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria.14 None of the patients had either asthma or atopy. The study was approved by the local ethics committee. All patients had a smoking history of at least 10 pack-years. The basal lung function of the patients is shown in table 1. All patients were stable and had had no exacerbation including viral or bacterial infection for at least 3 months before the study. None of the patients had been treated with inhaled or oral corticosteroid for at least 4 weeks before the study.
Characteristics of study subjects
Study design
The study was a randomised crossover design to compare the effects of theophylline 200 mg twice daily with fluticasone propionate (FP) 200 μg twice daily. Each treatment was administered for 4 weeks with a 4 week washout period between treatments. All patients were assessed at the start and end of the treatment period (fig 1). Nitrotyrosine immunoreactivity, differential cell counts, and protein bound 3-NT levels in induced sputum were measured at that time.

Study design.
Lung function testing
Lung function was evaluated using a dry rolling seal spirometer (System 7; Minato Medical Science, Osaka, Japan). Before and after treatment with theophylline or FP, forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) were measured. Each measurement was performed 15 minutes after inhalation of 400 μg salbutamol via a metered dose inhaler.
Sputum induction and processing
Sputum was induced and processed as described in previous studies.10,15 Briefly, after 15 minutes pretreatment with 400 μg salbutamol, all patients inhaled 4% hypertonic saline using an ultrasonic nebuliser (UN-701; AICA Co Ltd, Tokyo, Japan). Contamination of saliva was eliminated by visual inspection and examination with an inverted microscope. Hypertonic saline inhalation was performed for 15–30 minutes until the sputum volume was approximately 1 ml. The sputum sample was immediately treated with dithiothreitol (4 mg/g sputum) to dissociate the sulfide bonds of the mucus. Cell viability was determined by the trypan blue exclusion method. The total and absolute number of cells per ml processed sputum was calculated using a haemocytometer. 100 μl of the cell suspension adjusted to 1.0×106/ml were centrifuged in a Cytospin 4 cytocentrifuge (ThermoShandon, ThermoBioAnalysis, Tokyo, Japan) at 30g for 5 minutes. The preparation was stained with Hansel’s stain (Torii Pharmaceutical, Tokyo, Japan) to assess the cell differential counts and stored at −80°C until immunocytochemical analysis.
Immunocytostaining
Samples were immunostained with antisera against 3-NT as described in previous studies.10 Briefly, the preparation was fixed in 4% paraformaldehyde fixative solution for 30 minutes. Endogenous peroxidase activity was blocked by incubation in 0.3% hydrogen peroxide in phosphate buffered saline (PBS) for 15 minutes at room temperature. After washing in PBS, the preparations were incubated with anti-nitrotyrosine rabbit polyclonal IgG (1:100 dilution; Upstate Biotechnology, Lake Placid, NY, USA) for 12 hours at 4°C. Non-specific binding to the antibody was prevented by preincubation with 4% skimmed milk in PBS containing 0.3% Triton-X for 30 minutes. The immunoreactions were visualised by the indirect immunoperoxidase method using Envision polymer reagent which is goat anti-rabbit IgG conjugated with peroxidase labelled dextran (Dako Japan Ltd, Kyoto, Japan) for 1 hour at room temperature. Diaminobenzidine reaction was performed, followed by counterstaining with Hansel’s stain. The numbers of immunopositive cells were counted by two blinded investigators and the mean of the two values was registered. Cell types were distinguished by cell size, cell form, nuclear segmentation, and nuclear-cytoplasmic ratio.
Quantification of serum IL-8
The levels of serum IL-8 were measured using a commercially available ELISA kit (DuoSet ELISA Development Systems, R&D Systems, Minneapolis, MN, USA) according to the instructions provided by the manufacturer. The minimum detectable concentration of IL-8 was 31.2 pg/ml. A standard curve was obtained with serial dilution of the supplied recombinant human IL-8 by linear regression. The concentration of IL-8 in each sample was obtained by interpolation of its absorbance from a standard curve, and the mean value of the duplicate samples was then taken as the representative value.
Quantification of 3-nitrotyrosine
The levels of 3-NT in the cell-free supernatant were measured by HPLC/ECD as described previously.11 Briefly, the cell debris was removed by additional centrifugation of the sputum at 3000g for 15 minutes at 4°C and, to condense the samples, 400 μl of supernatant were centrifuged using an Ultrafree-MC centrifugal filter (Millipore Corp, Bedford, MA, USA) at 9000g for 30 minutes at 4°C. This filter can collect protein of over 10 kDa. After centrifugation, the protein concentration of the sample was determined by the Lowry method.16 After recovering the sputum protein, it was hydrolysed at 50°C for 18 hours with a freshly prepared solution of Streptomyces griseus Pronase (Calbiochem, Darmstadt, Germany) to liberate tyrosine and 3-NT residues. The hydrolysate was centrifuged at 9000g with filtration for 30 minutes with an Ultrafree-MC centrifugal filter and the filtrates were then analysed by HPLC/ECD.
50 μl of the sample were injected into a reverse phase column (C18: 3×150 mm; Eicom, Kyoto, Japan) at a flow rate of 0.5 ml/min. Eluents consisting of 5% methanol and 5 mg/l EDTA-2Na in 100 mM sodium phosphate buffer (pH 5.0) were continuously applied to the analytical electrochemical cells. The upstream electrochemical cell (coulometric cell) was used at −900 mV of applied potential for the reduction of 3-NT. The downstream cell (amperometric cell) was used at an oxidation potential of +300 mV for the detection of the reduced form of 3-NT. 3-NT was detected at a 13.5 minute retention time by the response at the oxidation cell on the basis of a standard curve of electrochemical responses as a function of the authentic 3-NT (Sigma Chemical Co, St Louis, MO, USA) concentration. We checked whether this peak was 3-NT as follows:11 (1) there was no difference in the retention time of the peak between the standard 3-NT and the sputum samples under these HPLC conditions; and (2) when the reduction potential was changed from −900 mV to −600 mV, only the peak at 13.5 minutes disappeared.
The effect of treatment with dithiothreitol on the 3-NT level was determined. Levels of 3-NT with and without treatment with dithiothreitol showed quite good correlation (r = 0.998, p<0.0001), so it was considered that the processing of induced sputum with dithiothreitol had no influence on the measurement of 3-NT.
The amount of tyrosine in the same sample was also determined in a separate process using HPLC analysis. Briefly, 1 μl of each sample was injected into a reverse phase column (Wakopak C30.5: 4.6 mm×300 mm, Wako Pure Chemical, Osaka, Japan) at a flow rate of 0.8 ml/min maintaining the temperature at 37°C. The eluents consisted of 5% methanol in 50 mM sodium acetate buffer (pH 4.7). Tyrosine was detected at a retention time of 8.47 minutes with the electrochemical response set at +600 mV. The amount of tyrosine in a sputum sample was determined based on the peak area compared with the standard curve of tyrosine (Wako Pure Chemical). The level of 3-NT was shown as a ratio to the total tyrosine concentration.
As shown in our previous report, the spike recovery analysis indicated that the percentage of recovery of 3-NT and tyrosine was more than 90%.11 In addition, the coefficient of variation of 3-NT measurement in sputum samples previously performed in triplicate was 5–10%, indicating that the determination of 3-NT by this technique is highly reproducible.11
Statistical analysis
All data were expressed as median (interquartile range). Comparison of outcomes between the theophylline and FP groups was performed using repeated measures ANOVA. Wilcoxon’s signed rank sum test was used to compare the effect of treatment on the total and differential cell counts and pulmonary function. Pearson’s correlation analysis was used to assess the correlations between changes in the RNS marker and those in the differential cell counts. A value of p<0.05 was considered to be significant.
RESULTS
The mean (SD) plasma theophylline level during theophylline administration was 6.32 (0.9) mg/l, which is lower than the clinically recommended concentration as a bronchodilator (10–20 mg/l). Because of this low concentration of theophylline, neither FP nor theophylline had a significant effect on FVC and FEV1 after 4 weeks of administration (FVC: before theophylline 3.34 (2.64–4.03) l; after theophylline 3.49 (2.81–4.16) l; before FP 3.41 (2.86–3.96) l; after FP 3.48 (2.89–4.07) l; FEV1: before theophylline 1.51 (1.11–1.91) l; after theophylline 1.60 (1.09–2.11) l; before FP 1.48 (0.91–2.05) l; after FP 1.59 (1.06–2.11) l).
Theophylline administration significantly reduced the total number of inflammatory cells in the sputum from 2.53 (1.79–3.26)×106/ml to 1.63 (1.01–2.24)×106/ml (p<0.01, table 2, fig 2A). Consistent with this, the number of neutrophils in the sputum also decreased significantly from 1.89 (1.35–2.42)×106/ml to 1.15 (0.80–1.49)×106/ml (p<0.01, table 2, fig 2B), while FP treatment did not affect the numbers of any inflammatory cells in the sputum with the exception of eosinophils (table 2, fig 2A, B). Neither theophylline nor FP had any effect on the number of macrophages in the sputum. The number of eosinophils was quite small, but significant decreases were seen with both theophylline and FP (table 2).
Differential cell counts in induced sputum

Effect of theophylline and fluticasone propionate (FP) on inflammatory cells. Theophylline significantly reduced the total number of inflammatory cells (A) and neutrophils (B), whereas FP had no apparent effect. Bars indicate median values.
To determine the mechanism of the decrease in neutrophils, we next measured the concentration of IL-8 in the sputum supernatant which is one of the well known chemoattractants of neutrophils. As shown in fig 3, theophylline significantly reduced the level of IL-8 in the sputum supernatant (from 1.77 (0.03–3.50) ng/ml before treatment to 1.04 (0.39–1.70) ng/ml after treatment (p<0.01), while FP did not. There was no apparent correlation between the serum levels of IL-8 and the number of neutrophils.

Effect of theophylline and fluticasone propionate (FP) on the concentration of interleukin (IL)-8. The IL-8 concentration in the sputum supernatant was significantly decreased by theophylline while FP had no effect. Bars indicate median values.
We then compared the effects of theophylline and FP on nitrative stress in the airway inflammation of COPD. As shown in table 3 and fig 4A–C, after 4 weeks of treatment with theophylline the total number of 3-NT positive cells in the induced sputum was decreased from 1.24 (0.75–1.72)×106/ml to 0.73 (0.28–1.18)×106/ml. Theophylline also decreased the number of immunopositive neutrophils for 3-NT from 0.97 (0.52–1.42)×106/ml to 0.53 (0.22–0.83)×106/ml (p<0.01, table 3, fig 4D). In contrast, although FP also decreased the total number of 3-NT positive cells (from 1.35 (0.86–1.83)×106/ml to 0.83 (0.25–1.41)×106/ml, p<0.05), the effect was milder than that of theophylline and there was no apparent effect on the number of 3-NT positive neutrophils (0.89 (0.47–1.32)×106/ml before treatment, 0.52 (0.12–0.93)×106/ml after treatment; table 3, fig 4C, D).
Positive cell counts of 3-nitrotyrosine (3-NT) in induced sputum
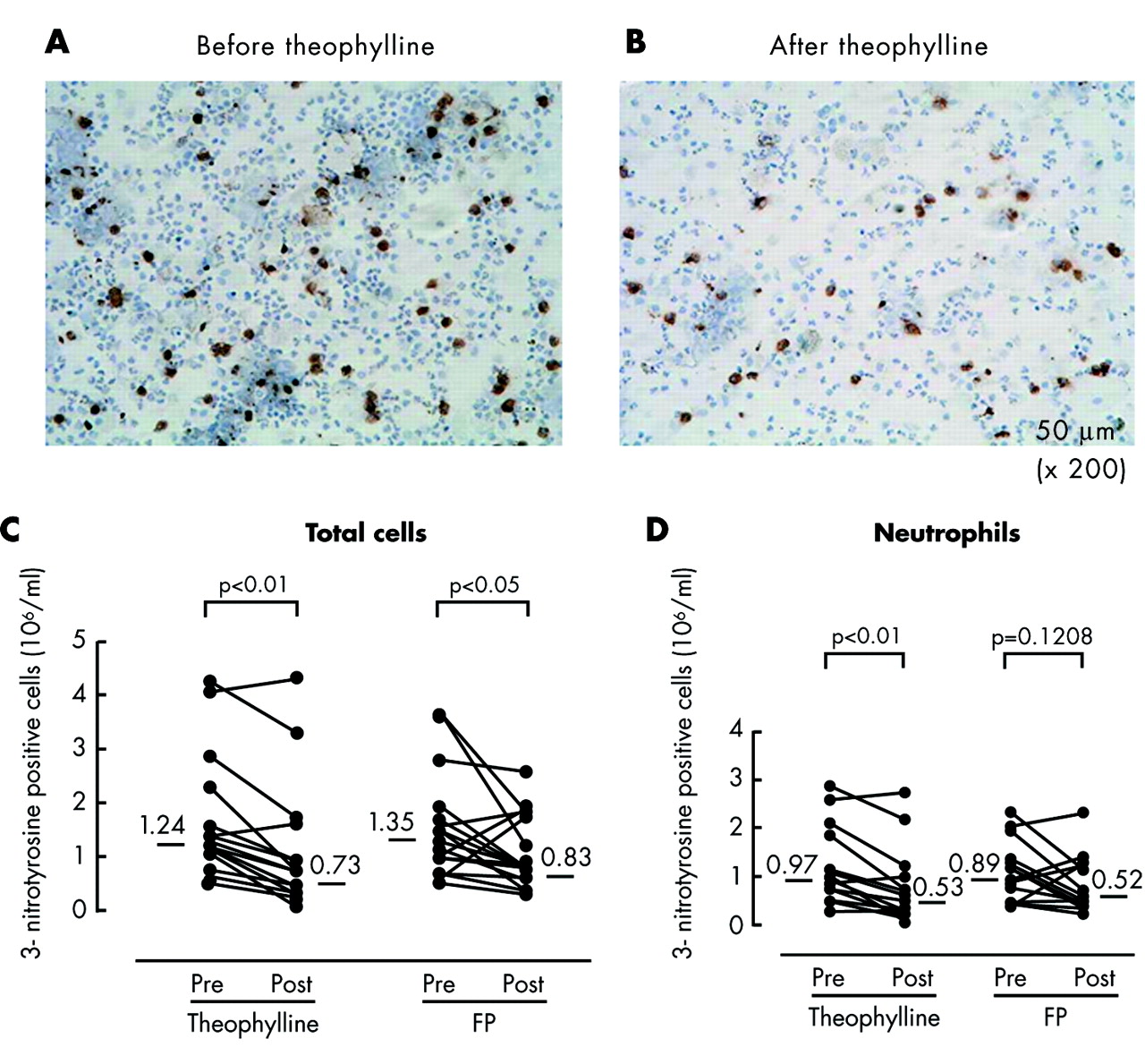
Effect of theophylline and fluticasone propionate (FP) on immunocytochemical staining against 3-nitrotyrosine (3-NT). Immunopositive inflammatory cells for 3-NT in the induced sputum were reduced after treatment with theophylline (B) compared with before treatment (A). Theophylline significantly reduced the total immunoreactivity of 3-NT in inflammatory cells (C) and neutrophils (D). FP also reduced the total immunoreactivity of 3-NT in inflammatory cells, but not in neutrophils. Bars indicate median values.
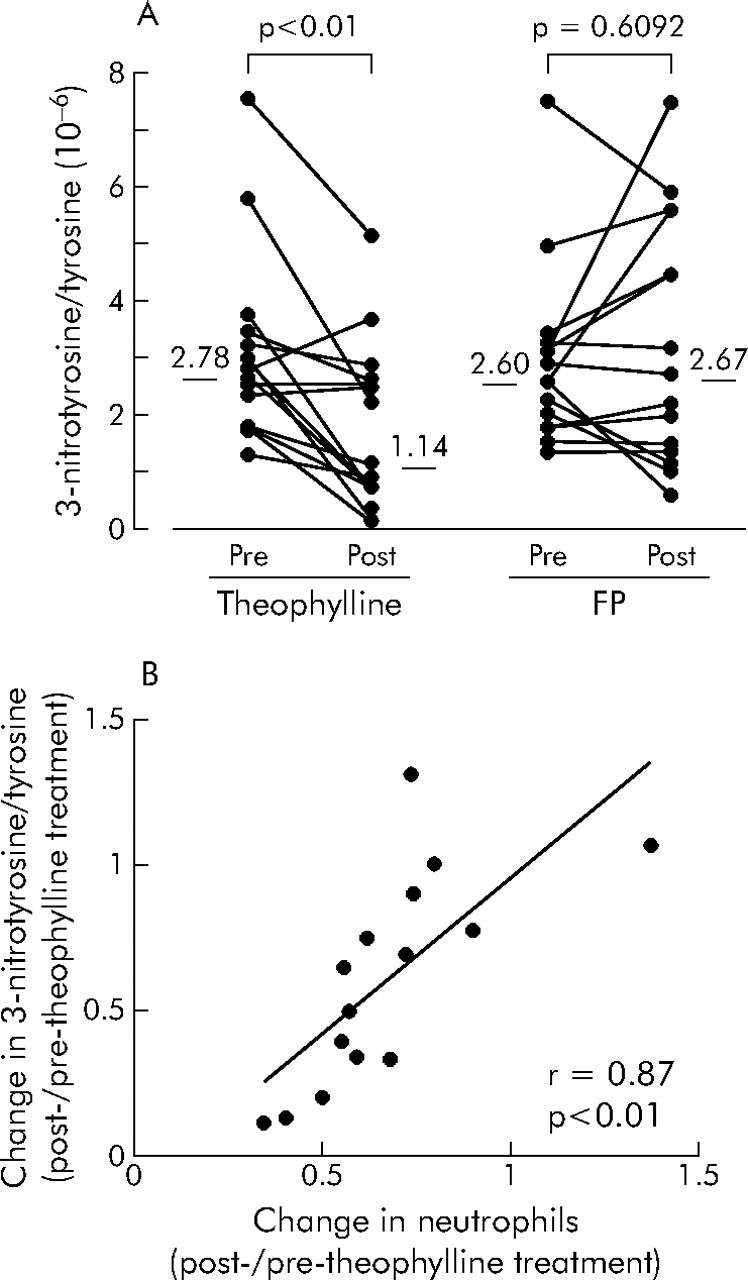
We next measured the levels of 3-NT in sputum. There was a possibility that current smoking may affect the levels of 3-NT, but no significant difference in 3-NT levels was seen between current smokers and ex-smokers, at least in the present study (current smokers 2.14×10−6, ex-smokers 3.43×10−6 3-NT/tyrosine). Consistent with the results of immunocytochmeical staining, the level of 3-NT in the sputum supernatant was significantly decreased after 4 weeks of treatment with theophylline (p<0.01, fig 5A), while no apparent effect was seen after treatment with FP. As shown in fig 5B, there was a significant positive correlation between the decrease in the number of neutrophils in the induced sputum and the reduction in 3-NT levels in the sputum supernatant in those treated with theophylline (r = 0.87, p<0.01). There was no significant correlation between the serum IL-8 levels and the levels of 3-NT in sputum.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of theophylline and fluticasone propionate (FP) on 3-nitrotyrosine (3-NT) levels (A) Theophylline significantly reduced the level of 3-NT in induced sputum as measured by HPLC/ECD, while FP had no effect. (B) There was a significant correlation between the decrease in neutrophils and the decrease in the 3-NT level after theophylline treatment. Bars indicate median values.
DISCUSSION
We have shown for the first time that treatment with low dose theophylline significantly reduces RNS production and neutrophil infiltration to a greater extent than inhaled corticosteroid in COPD airways.
We have previously reported the effect of inhaled corticosteroid on the suppression of nitrative stress in COPD airways. In that study, administration of inhaled corticosteroid for 4 weeks significantly reduced total 3-NT immunoreactivity of inflammatory cells, macrophages and neutrophils in the induced sputum.12 Inhaled corticosteroid also reduced the inducible nitric oxide synthase (iNOS) immunoreactivity in those cells. The formation of nitrotyrosine depends on the oxidation of nitric oxide (NO), which reacts with superoxide anion to produce the more potent RNS, peroxynitrite.17 Peroxynitrite causes tyrosine nitration. Because iNOS is one of the main sources of NO production, it is suggested that the mechanism of nitrative stress inhibition by inhaled corticosteroid, as in our present study, could be due mainly to the reduction of iNOS.
Low dose theophylline reduced nitrative stress in COPD airways to a larger extent than inhaled corticosteroid. Theophylline also inhibited neutrophilic inflammation in COPD airways. In addition, as shown in fig 5, there was a significant positive correlation between the reduction in 3-NT levels and the decrease in the number of neutrophils after theophylline administration. An alternative pathway for the formation of 3-NT is via the neutrophil myeloperoxidase (MPO) effect on NO.17,18 Nitrite produced by the reaction of NO with oxygen is oxidised by MPO which results in the formation of reactive nitrogen intermediates. These products are also involved in tyrosine nitration.17 It is therefore possible that the theophylline induced inhibition of nitrative stress seen in the present study was due to the inhibition of neutrophil infiltration.
We also observed a significant reduction in IL-8 production after theophylline administration, which is a possible mechanism for the inhibition of neutrophilic inflammation by theophylline. This is compatible with the findings of a previous study.13 The precise mechanism of IL-8 reduction by theophylline is unclear. However, it has recently been shown that theophylline can inhibit the release of IL-8 from respiratory epithelial cells in vitro.19 The direct effect of theophylline on respiratory epithelial cells might therefore be one possible mechanism.
A new anti-inflammatory mechanism by theophylline in the treatment of COPD has recently been proposed by Barnes and co-workers.20–22 The activity of histone deacetylases (HDACs), which mediate inflammatory gene repression, is reduced in patients with COPD.23 Although the precise mechanism of this inactivation of HDACs is not yet clear, oxidative/nitrative stress might be involved via the nitration of tyrosine residues in the active centre of HDACs by peroxynitrite or other RNS.24,25 Theophylline has been reported to restore the decreased HDAC activity in patients with COPD.20 In this study we have shown, for the first time, the reduction in tyrosine nitration by theophylline using electrochemical as well as immunohistochemical techniques. Our results support the hypothesis of Barnes and colleagues. It is considered that combined evaluation of the HDAC activity and nitrative stress by HPLC/ECD could clarify the precise mechanism of action of theophylline.
Recent investigations have shown that RNS has an important role in the pathogenesis of COPD, causing cell injury,26 activation of metalloproteinases,27 inactivation of α1-antiproteinase,28 and enhanced IL-8 production.29 Neutrophilic airway inflammation is another important feature of COPD,1–3 and neutrophils are an important source of RNS.10 It is considered that both neutrophilic inflammation and oxidative/nitrative stress could have critical roles in the development of COPD. The findings of our study suggest that theophylline might be a useful therapeutic tool for COPD treatment by inhibiting both neutrophilic airway inflammation and nitrative stress.
In conclusion, treatment with theophylline reduces nitrative stress as well as neutrophilic inflammation in COPD. Because there is a significant positive correlation between the decrease in the number of neutrophils and the reduction in 3-NT levels, the reduction in nitrative stress is considered to be due mainly to the inhibition of neutrophilic inflammation. Since the suppression of nitrative stress seems to be effective in inhibiting the inflammatory process and subsequent obstructive changes in COPD airways, theophylline may slow the progression of airway obstruction in COPD. Further large, long term, placebo controlled studies with a range of concentrations of theophylline and different severities of COPD are needed to confirm this hypothesis.
Acknowledgments
The authors thank Koji Fukui for his technical help with the study and Brent Bell for reading the manuscript.
REFERENCES
Footnotes
-
Published Online First 31 May 2006
-
Competing interests: none declared
Linked Articles
- Correction