Article Text

Abstract
Background Despite extensive knowledge regarding the effect of pulmonary exacerbations treated with intravenous antibiotics on clinical outcomes in cystic fibrosis (CF), there is little known about the role of milder pulmonary exacerbations treated with oral antibiotics (oPEx).
Methods This was a retrospective cohort study of patients with CF followed at the Hospital for Sick Children and St. Michael's Hospital from 2009 to 2014. We evaluated the effect of oPEx on short-term clinical outcomes as the proportion of oPEx events in which 100% or 90% of baseline FEV1% predicted was recovered at the end of treatment. We then examined the association of the number of oPEx events in the past 12 months on lung function (FEV1% predicted) and nutritional status (body mass index (BMI) z-score) using a mixed-effects model.
Results There were a total of 2608 oPEx events in 570 subjects during the study period. In over half (53.4%) of oPEx events, lung function was already at 90% or higher of baseline FEV1 at the initiation of oral antibiotic therapy and 82% were at 90% or higher of baseline FEV1 at follow-up. In individuals with CF, one or more oPex events in the previous 12 months were associated with decreased FEV1 compared with 12 months periods without oPex events. When the cumulative effect of oPExs on lung function was examined over the entire study period, patients with six or more oPEx events had the steepest rate of FEV1 decline. oPEx events were not associated with changes in BMI.
Conclusions oPEx events are associated with short-term loss of FEV1 and have a negative effect on lung function over time.
- Cystic Fibrosis
- Respiratory Measurement
- Respiratory Infection
Statistics from Altmetric.com
Key messages
What is the key question?
Although the impact of pulmonary exacerbations treated with intravenous antibiotics in patients with cystic fibrosis (CF) has been well described, there is little known about the role of milder pulmonary exacerbations treated with oral antibiotics on short lung function recovery and long-term FEV1 decline in CF.
What is the bottom line?
Pulmonary exacerbations treated with oral antibiotics were associated with short-term loss of FEV1 at the time of an exacerbation and an increasing number of exacerbation events were found to be independently associated with FEV1 decline.
Why read on?
This study describes the impact of pulmonary exacerbations treated with oral antibiotics in a large adult and paediatric CF population over a 6-year period using repeated lung function and nutritional measurements, demonstrating the cumulative negative effect of these events on lung function over time.
Introduction
Patients with cystic fibrosis (CF) experience episodes of acute worsening of respiratory symptoms, referred to as pulmonary exacerbations. In epidemiological research studies, hospitalisation or the use of intravenous antibiotics for respiratory causes is commonly used to define a severe pulmonary exacerbation.1 ,2 Severe exacerbations requiring intravenous antibiotics are associated with decreased lung function over time,3 ,4 and a quarter to a third of patients with CF do not recover their baseline FEV1 after an exacerbation and may be at risk of never regaining this lung function.5 ,6 When assessed longitudinally, approximately half of the decline in FEV1 in patients with CF is associated with these episodes of severe exacerbations.7 Despite extensive knowledge regarding the effect of pulmonary exacerbations treated with intravenous antibiotics on clinical outcomes in CF, there is less known about the role of milder pulmonary exacerbations treated with oral antibiotics in the CF population.
In current clinical practice, physicians often prescribe oral antibiotics to treat less severe pulmonary exacerbations. While pulmonary exacerbations treated with oral antibiotics may be classified as milder and do not lead to hospital admission, given their frequency, they may be associated with long-term clinical outcomes, especially in children. Only one study has examined the use of oral antibiotics to treat pulmonary exacerbations. Wagener et al8 demonstrated that pulmonary exacerbations treated with oral antibiotics have a negative effect on FEV1, but they did not define the impact on recovery of baseline lung function or long-term FEV1 decline. The objective of this study was therefore to analyse the effect of pulmonary exacerbations treated with oral antibiotics on short-term and long-term clinical outcomes in the Toronto CF population.
Methods
Study design and data collection
This was a retrospective cohort study of individuals with CF followed at the Hospital for Sick Children and St. Michael's Hospital (Toronto, Ontario, Canada) from 2009 to 2014. Data for this study were extracted from the Toronto CF Database housed at the Hospital for Sick Children. This encounter-based database prospectively collects information from all paediatric and adult CF subjects from every visit including sputum microbiology, medications and pulmonary function testing.9 Subjects are included in this database if they have a confirmed diagnosis of CF based on (1) the presence of clinical features consistent with CF or (2) a positive family history for CF and either two documented sweat chloride values >60 mEq/L measured by quantitative pilocarpine iontophoresis test, genetic testing showing two CF-causing mutations or a nasal potential difference consistent with CF.10 Specific information on antibiotic treatment and indication for their use was obtained through a systematic review of medical records at the Hospital for Sick Children and St. Michael's Hospital by two of the study investigators (SM and EH). Antibiotics prescribed over the phone to patients who are not seen in clinic were captured in this dataset in the form of written notes included in the medical chart. If there was mention of an antibiotic course prescribed by a primary care physician in the clinic letter, this information was also included in the dataset. This study was approved by the Research Ethics Board at the Hospital for Sick Children (REB# 1000013759) and St. Michael's Hospital (REB# 09-087c).
Study definitions
A pulmonary exacerbation was defined as a clinical event treated with antibiotics for a respiratory cause.11 For each event, patients received either oral antibiotic treatment for a pulmonary exacerbation (oPEx) or intravenous antibiotic treatment for a pulmonary exacerbation (iPEx) based on physician assessment. During a single exacerbation, patients may have been treated with both oral and intravenous antibiotics; these events were classified as iPExs. Patients may have also experienced multiple exacerbations during the study period. The median time between consecutive exacerbations treated with oral antibiotics was 150 days (IQR 63–324 days), <5% of all events had fewer than 10 days between oral antibiotic treatments. Similarly, the median time between consecutive events treated with oral and intravenous antibiotics was 56 days (IQR 21–184 days), <5% of events had fewer than 4 days between treatments. Therefore, events separated by more than 1 day were classified as separate exacerbations. All analyses were also repeated with distinct events separated by 14 days. Events treated with inhaled antibiotics were not classified as pulmonary exacerbations as it is not standard practice to treat exacerbations with inhaled antibiotics alone at the Hospital for Sick Children or St. Michael's Hospital. Episodes treated with antifungal or antimycobacterial drugs were not included in the study.
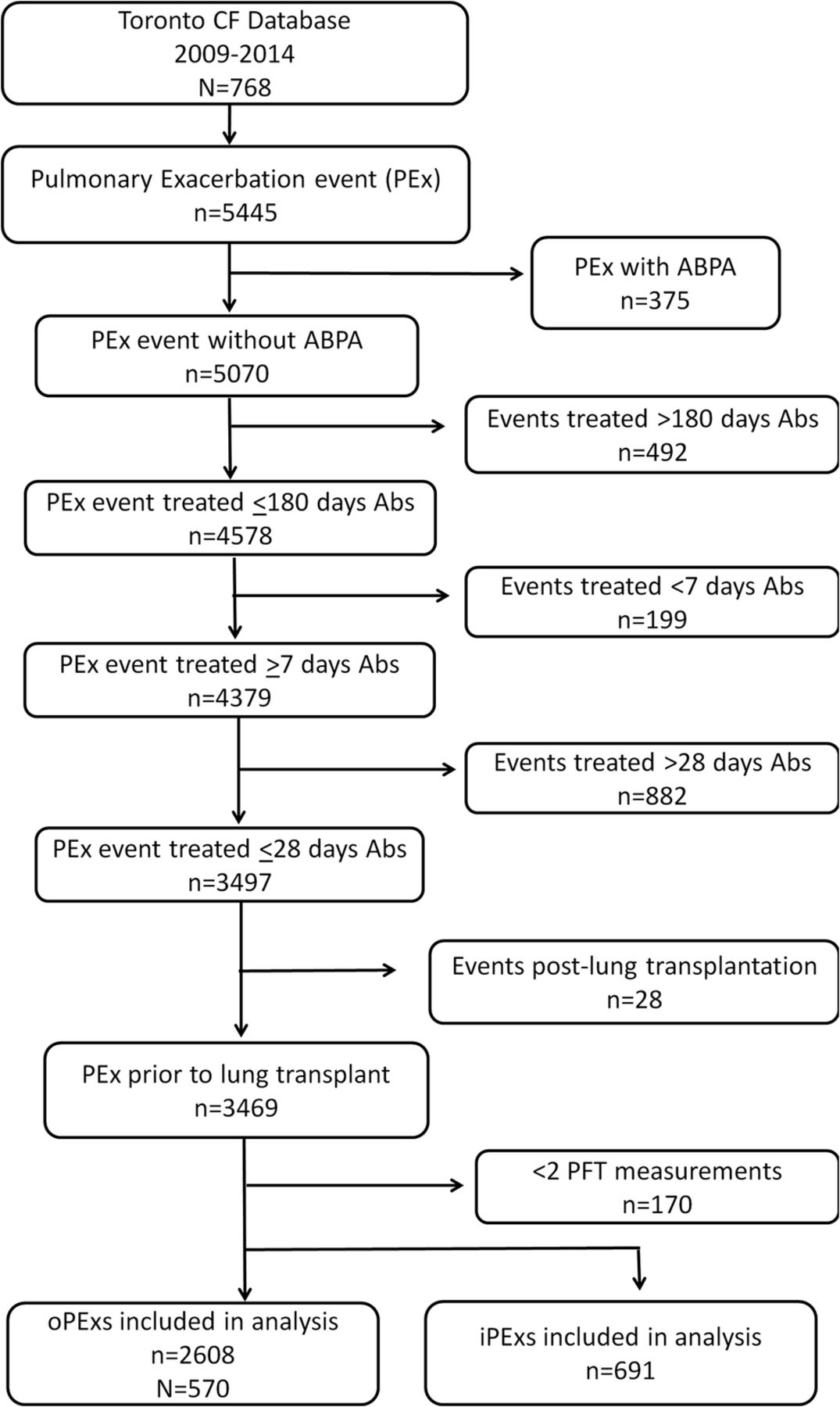
The following exclusion criteria were applied for the pulmonary exacerbation events identified from 2009 to 2014 in the Toronto CF Database (figure 1): (1) active allergic bronchopulmonary aspergillosis (ABPA) as defined by the use of steroids for the treatment of ABPA as recorded in the clinicians' notes,12 (2) events treated with >180 days of antibiotics (representing chronic antibiotic therapy), (3) antibiotic treatment duration <7 days or (4) antibiotic treatment duration >28 days (7–28 days represented 80% of oral antibiotic treatment courses (see online supplementary figure S1)), (5) any events after lung transplantation and (6) <2 pulmonary function tests (PFTs) during the study period.
Supplementary figures

CONSORT diagram showing selection of study population from Toronto CF Database for pulmonary exacerbations treated with antibiotics (oPEx or iPEx) during the study period from 2009 to 2014. ABPA, allergic bronchopulmonary aspergillosis; Abs, antibiotics; CF, cystic fibrosis; iPEx, pulmonary exacerbations treated with intravenous antibiotics; oPEx, pulmonary exacerbations treated with oral antibiotics; PFT, pulmonary function test; n, number of pulmonary exacerbations; N, number of subjects.
The effect of oPEX events was measured on two main outcomes: FEV1 and body mass index (BMI). FEV1 values were adjusted for sex, age, height and ethnicity using Global Lung Function Initiative reference equations and standardised as per cent predicted values.13 BMI Z-scores were calculated according to sex and age using Centers for Disease Control and Prevention (CDC) Growth Charts.14 For patients older than 19 years, BMI Z-scores were calculated by extrapolating from the growth charts at age 19.
Statistical analyses
Initial response to antibiotic treatment
To evaluate the effect of oPEx events on short-term clinical outcomes, we determined the proportion of oPEx events in which 100% or 90% of per cent predicted FEV1 (FEV1%) at baseline was recovered at the end of oral antibiotic treatment.12 CIs were estimated from a mixed-effects model to account for the repeated events in a single patient.
Both outcomes (FEV1% predicted or BMI Z-score) were analysed at baseline, start of oPEx treatment (day 0), end of oPEx treatment and follow-up. Baseline was defined as the best value (FEV1% predicted or BMI Z-score) in the 6 months prior to the exacerbation,5 where the values were restricted to stable visits (ie, did not overlap with treatment with either oral or intravenous antibiotics). Day 0 was defined as the measurement closest to start of treatment, within a window of ±4 days from start of treatment. End of treatment values were defined as the measurement closest to end of treatment, within a window of ±4 days from end of treatment. Follow-up values were defined as the best value in the 3 months following the end of treatment,5 where the value did not overlap with treatment with either oral or intravenous antibiotics.
Long-term impact on lung function and nutritional status
To examine the association of oPEx with (1) lung function (FEV1% predicted) and (2) nutritional (BMI Z-score), we constructed a mixed-effects model, with random intercepts, random slopes (age) and an exchangeable correlation structure to adjust for the correlated nature of repeated outcome measurements within the same subject. The primary explanatory variable was the cumulative number of oPEx events in the previous 12 months (categorised as none, 1 or ≥1) which was treated as a time-varying coefficient. Potential time-independent covariates included sex, pancreatic insufficiency, age at diagnosis (≤2 years, >2 years), functional class of CF transmembrane conductance regulator mutation (class I–III, class IV–V, unknown), baseline PFT and BMI measurements (defined as the first recorded measurement in the study period not overlapping an antibiotic treatment period) and follow-up time in the study. The following covariates were treated as time-varying variables: age at lung function measurement, number of iPExs events in the previous 24 months (rather than 12 months given the low frequency of events, categorised as none; 1 or ≥1), CF-related diabetes (CFRD) and age group (based on the age of the patient at lung function measurement; paediatric ≤18 years of age and adult >18 years of age). In additional microbiology, results were treated as time-varying variables and included chronic infection with Pseudomonas aeruginosa15 and any positive respiratory tract culture in the 12 months prior to the outcome measurement for Stenotrophomonas maltophilia, Burkholderia cepacia complex, Staphylococcus aureus, Haemophilus influenzae, Aspergillus species, methicillin-resistant S. aureus (MRSA) infection or Achromobacter xylosoxidans.
Using a stepwise approach, we first examined the relationship between the outcome and age, and adjusted for each patient's follow-up time. Subsequently potential covariates were entered into the model, adjusted for age and follow-up time, independently to determine which factors were significantly associated with FEV1 or BMI (p value <0.15). Variables were then maintained in the multivariable model if they were independently associated with the outcome or if they changed the coefficient for the effect of oPEx by more than 10%. A backward elimination approach was used to select the variables in the final multivariable model.
Results
Patient characteristics
From 2009 to 2014, 768 patients were followed in the Toronto CF database; of these, 570 subjects matched the inclusion criteria (figure 1). Overall, pulmonary symptoms were treated with oral antibiotics (oPEx) nearly four times more often than were treated with intravenous antibiotics (iPExs) during the study period (2608 vs 691). Seventy-one per cent of the CF population (n=549) had at least one oPEx during the study period. The baseline characteristics of the study population (N=570) are presented in table 1.
Characteristics of the study population
The study population had a median age of 21 years (IQR 11.5–32.9 years) and a median baseline FEV1% predicted of 72% (IQR 51.9–89.2%); the most common bacteria found in respiratory cultures was S. aureus. The median follow-up time for the study population was 5.5 years (IQR 3.8–5.7 years), and there was a median of 4 (IQR 2–7) oPEx events per patient during the study period. One-third of the study population had six or more oPEx episodes during the study period. The annual rate of oPEx was greater in paediatric patients (median 1.1/patient/year (IQR 0.5–1.7) compared with adult patients (median 0.8/patient/year (0.4–1.3).
Treatment response to oral antibiotics
Relative to baseline lung function, FEV1 was −6.9 percentage points (95% CI 6.1 to 7.7, N=368, n=626; p<0.001) lower at the start of the oPEx, −3.6 percentage points (95% CI 2.4 to 4.7, N=194, n=24; p<0.001) lower at the end of treatment and −0.88 percentage points (95% CI 0.4 to 1.4, N=433, n=1025; p=0.001) lower at the follow-up visit. The percentage of oPEx events in which lung function was at ≥90% of baseline FEV1 or at ≥100% of baseline FEV1 at day 0 (start of treatment), end of treatment and follow-up is illustrated in figure 2. The distribution of the relative change from baseline to start of treatment for all oPEx events is shown in online supplementary figure S2. Of note, in over half of oPEx events, lung function was already at 90% or higher of baseline FEV1 at the initiation of oral antibiotic therapy and 82% were at 90% or higher of baseline FEV1 at follow-up. The proportion of oPEx events with lung function at 100% or greater of baseline FEV1 was much lower at every time point (figure 2). The response rates were similar when a 14-day interval was used to define distinct events. We also examined the response to oPEx events within different age groups (see online supplementary figure S3); none of the observed differences between the age groups were statistically significant.

The per cent of oPEx events with ≥90% (dark grey bars) and ≥100% (light grey bars) of baseline FEV1 % predicted at day 0 (n=626), end of antibiotic treatment (n=264) and at follow-up after oral antibiotic treatment for a pulmonary exacerbation (n=1025). oPEx, pulmonary exacerbations treated with oral antibiotics.
Association of oPEx events and lung function and nutritional status
We first investigated the effect of oPExs on lung function by examining the association between the number of oPEx events in the previous 12 months and FEV1. Lung function was significantly decreased if patients had one or more oPEx events in the 12 months prior to the FEV1 measurement compared with 12 month periods without oPEx events (table 2—model 1). This effect was maintained after adjusting for the number of iPEx events in the 24 months prior to the lung function measurement (table 2—model 2). After adjusting for other time-varying factors (CFRD, Aspergillus infection, MRSA infection), lung function was reduced in patients with oPEx events, but the decrease was not statistically significant (table 2—model 3). Neither oPEx nor iPEx events were associated with lower BMI Z-scores in this analysis (see online supplementary table S1A).
The association between oPEx events in the previous 12 months and FEV1% predicted
Supplementary tables
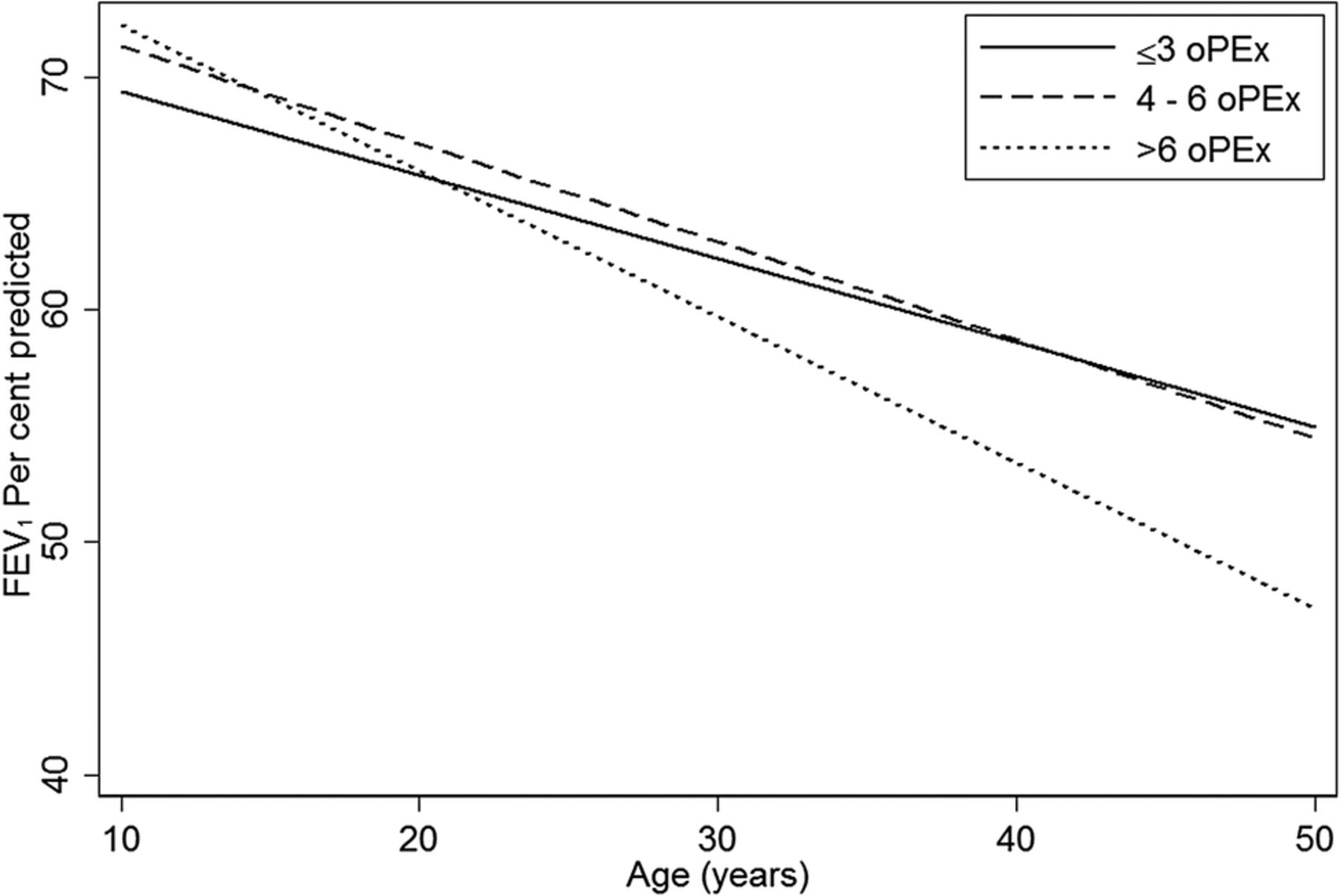
We then examined the cumulative effect of oPExs on lung function decline during the entire study period. The overall rate of FEV1 decline for the study population was −1.1% per year (95% CI −1.2 to 1.05). Patients in the tertile with the greatest number of oPEx events had the steepest rate of lung function decline during the study period (table 3—model 1; figure 3). This was also observed after adjustment for the other factors associated with lung function decline (number of iPEx events, age group, gender, age at diagnosis, pancreatic status, CFRD, baseline FEV1% predicted and infection with H. influenzae, Aspergillus species, A. xylosoxidans) (table 3—model 2). The results were similar in the sensitivity analysis using 14 days to separate events. In addition, the pattern of lung function decline was similar when the analysis was stratified by paediatric and adult patients (see online supplementary figure S4). For BMI, in all three oPEx groups, there was a decline over time with age; however, when adjusted for the above variables, the rate of decline was close to 0 in all three groups (see online supplementary table S1B).
Cumulative effect of total number of oPEx events during the study period and lung function decline

{kind=link}
{kind=link}
{kind=link}
Change in FEV1 % predicted based on cumulative number of oPEx events during the study period: ≤3 (solid line) (50% of oPExs), 4–6 (hatched line) (25% of oPExs) and >6 (dotted line) (25% of oPExs). oPEx, pulmonary exacerbations treated with oral antibiotics.
Discussion
In this study, we systematically measured the effects of pulmonary exacerbations treated with oral antibiotics on short-term and long-term clinical outcomes in a paediatric and adult CF population. We found that a significant proportion of patients treated with oral antibiotics for increasing respiratory symptoms did not recover baseline lung function and that oPEx events were associated with decreased lung function in patients with CF.
There is only one other study that has investigated the effects of oral antibiotic treatment for pulmonary exacerbations on lung function in CF. Wagener et al8 used 3 years of data from the Epidemiologic Study of Cystic Fibrosis to analyse almost 50 000 pulmonary exacerbations. Their primary objective was to characterise treatment patterns of CF pulmonary exacerbations with a secondary focus on clinical outcomes. Wagener et al found that oral antibiotic use was very prevalent, especially in younger patients with less severe disease, and represented the most common method of antibiotic administration (73% of exacerbations), a finding similar to that of the present study. The authors also found that oral antibiotic treatment was associated with a smaller absolute and relative increase in FEV1 compared with intravenous therapy, but they did not take into consideration the initial magnitude of lung function change associated with the exacerbation. Our data demonstrated that in most oPEx events (>50%), lung function did not drop by more than 10% from baseline levels. The lack of an initial drop in lung function may have contributed to the smaller absolute and relative improvements in FEV1 observed with oral compared with intravenous antibiotic treatment. Nonetheless, in nearly 20% of these milder events treated with oral antibiotics, lung function did not improve to baseline values within 3 months of treatment. While the proportion of events was smaller than that reported (25%–30%) for events treated with intravenous antibiotics,5 ,6 it represented a larger absolute number of cases as oPEx events were nearly four times more common than iPEx events.
In their assessment of longer term outcomes, Wagener et al compared the best FEV1 in the 6 months following the event to the best in the 1 year prior to the event and found that FEV1 losses were similar between oPEx and iPEx events. In our encounter-based patient registry, patients had repeated lung function measurements within shorter intervals close to the exacerbation event, as well as repeated exacerbation events over a 5-year period, which allowed us to investigate how oPEx and iPEx events affect lung function over time in patients with CF. When the effect of oPExs on lung function was examined over a short time frame (12 months), patients with one or more episodes had decreased FEV1 compared with periods when they did not have any oPEx events. This effect was independent of more severe iPEx events but was influenced by other factors such as bacterial infection. This is not surprising given the number of factors known to influence CF lung disease. However, when the cumulative effect of oPExs was analysed over a longer time period, the negative impact on repeated oPEx events on FEV1 decline was evident, indicating that they are clinically relevant measures in individuals with CF.
Given the contribution of oPEx events on both short-term and long-term clinical outcomes in patients with CF, the results of our study raise a number of questions. The first is how to capture the treatment of milder exacerbation events that typically occur as an outpatient and are frequently not included in registry data. The second is how to treat patients with frequent, repeated oPEx events who may warrant more intensive treatment to prevent negative consequences.
The results of our study also have relevance with respect to the choice of outcome measures for clinical trials. Traditionally, pulmonary exacerbations in clinical trials have been defined by the use of intravenous antibiotics to treat major respiratory symptoms such as a decrease of ≥10% in FEV1, haemoptysis or radiographic changes.16 Randomised controlled studies of dornase alfa16 and hypertonic saline17 in individuals with CF have demonstrated reduction in the number of exacerbations with treatment using this definition. However, in a study of oral azithromycin in children with CF uninfected with P. aeruginosa, subjects presenting with exacerbations were more likely to have milder symptoms such as cough, rather than significant drops in lung function, which were treated with oral rather than intravenous antibiotics.18 Follow-up analysis of this randomised, double-blind controlled trial did not show a difference in the mean change in FEV1 between patients with no exacerbation compared with those with at least one symptom-based exacerbation in the 6-month follow-up period.19 However, the short follow-up time may have missed the long-term effects observed in the 5-year observation period of the current study. Recent interventional trials of inhaled antibiotics in patients with CF have demonstrated benefit in terms of reduction in milder exacerbations, defined as the use of antipseudomonal antibiotics administered by any route.20–22 With the long follow-up time in our study (over 5 years), we were able to demonstrate that repeated oPEx events have an impact on long-term lung function decline which supports the concept of including these events into pulmonary exacerbation definitions used in clinical trials.
The current study has several limitations. First, due to its retrospective nature, our data lacked specific symptoms associated with pulmonary exacerbations. We defined an oPEx based on a clinician's decision to treat with oral antibiotics which may have introduced an indication bias. Not all exacerbation events will come to medical attention and given that there is no standard protocol for the treatment of exacerbations at our centres, there is likely to be variability in the decision to prescribe antibiotics between different clinicians. Our primary analysis defined distinct events as those where treatment was separated by 1 day. Since treatments within 14 days may be related to the same pulmonary event, we repeated all of the analysis using 14 days between treatments to define distinct events; the results were remarkably similar. Furthermore, while a 10% change in FEV1 is routinely used as a marker of a precipitous drop in lung function indicating worsening clinical status, the normal repeatability of FEV1 is likely to be different for patients with milder disease compared with severe disease. Therefore, it is difficult to conclude whether an observed change in FEV1 is a consequence of intrinsic variability or a true measure of lung function change in this study population, for whom lung function measures were not always available at every time point for every subject. This may have introduced a potential selection bias for those who did get repeat pulmonary function testing as they may have had specific patient characteristics. To estimate the cumulative effect of repeated oPEx events, we did not have a large enough negative control group given the limited number of subjects with zero oPExs during the study period. Furthermore, we could not investigate the sequence in which oPEx and iPEx events occur, whether one is a precursor of the other. Finally, as an observational study, we cannot conclude causality based on the results, only associations.
In conclusion, oral antibiotic therapy for respiratory symptoms is very common in individuals with CF, especially in younger patients, and is frequently triggered by factors other than acute drops in lung function. However, although these events may appear milder, like exacerbations treated with intravenous antibiotics, oPEx events are associated with loss of FEV1 compared with baseline and have a cumulative effect on lung function over time. These events represent clinically relevant study outcome measures for interventional trials in children with CF with milder lung disease.
References
Footnotes
SS and AM contributed equally.
Contributors All authors contributed to the design, data collection and analysis and writing of the manuscript.
Funding This study was funded by an unrestricted grant from Vertex Pharmaceuticals. AM was funded by a Summer Studentship from CF Canada.
Competing interests None declared.
Ethics approval Hospital for Sick Children, St Michael's Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves