Article Text

Abstract
This observational study aims to assess the outcome and safety of O2-therapy by high-flow nasal cannula (HFNC) in 28 consecutive patients with severe hypoxemic acute respiratory failure (hARF) consequent to SARS-CoV-2 infection, unresponsive to conventional O2-therapy. Nineteen patients had a positive response. Nine patients required escalation of treatment to non-invasive ventilation (five subsequently intubated). None of the staff had a positive swab testing during the study period and the following 14 days. Severity of hypoxemia and C reactive protein level were correlated with HFNC failure. These data suggest HFNC to be a safe treatment for less severe patients with SARS-CoV-2 hARF and efficacy will need to be assessed as part of a clinical trial.
- critical care
- viral infection
- respiratory infection
- non invasive ventilation
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Patients with Coronavirus 2 (SARS-CoV-2) infection may experience severe hypoxemic acute respiratory failure (hARF) requiring supportive respiratory therapy.1
O2-therapy by high-flow nasal cannula (HFNC), which allows delivering heated, humidified inspired gas at a high flow rate and precise fraction of inspired oxygen (FiO2), has been increasingly used in patients with severe hARF.2 Recent guidelines for the management of SARS-CoV-2 infection suggest HFNC also for treatment of SARS-CoV-2 hARF unresponsive to conventional O2-therapy.3 However, data on the efficacy of HFNC in these patients are scarce and there are major concerns on the possibility of spreading infection among healthcare personnel caring for patients in SARS-CoV-2 dedicated areas.
We report the outcomes of 28 consecutive unselected patients with hARF admitted to the SARS-CoV-2 Respiratory Intensive Care Unit (RICU) of the University Hospital of Padua between 13 and 23 March 2020 who underwent HFNC. The criterion for patients’ admission to our RICU was failure of conventional O2-therapy to maintain SaO2 ≥92%. Study ethical approval was waived by the local Ethics Committee in view of the fact that all the procedures being performed were part of the routine care.
Study inclusion criteria were (1) laboratory-confirmed COVID-19 infection4; (2) PaO2/FIO2 ratio <300 mm Hg, FIO2 being determined as previously described5; (3) failure of conventional O2-therapy delivered through a non-rebreathing mask with a reservoir bag to maintain SaO2 ≥92%. Exclusion criteria were need for immediate endotracheal intubation (ETI) and haemodynamic instability.
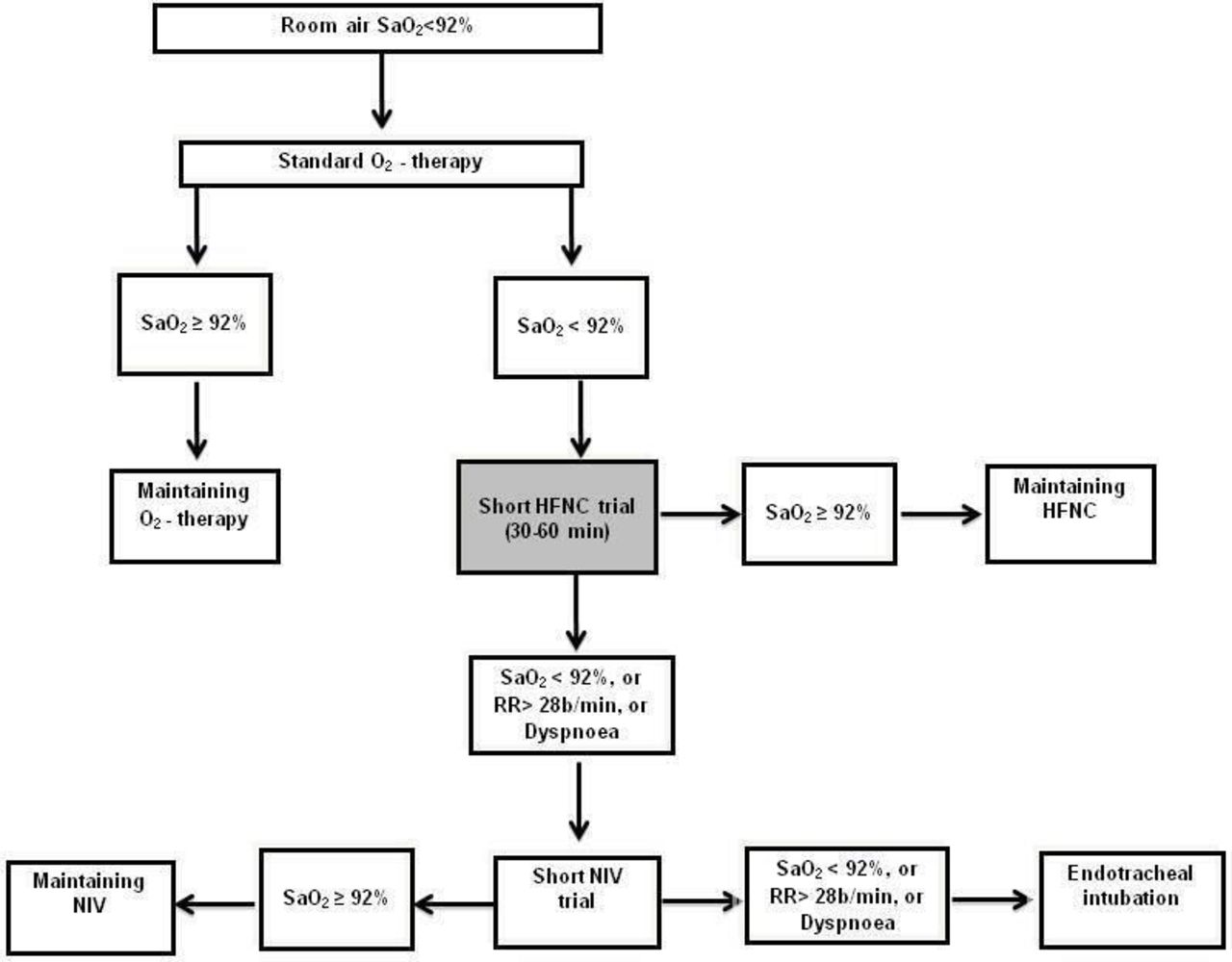
A treatment algorithm from the hospital internal protocol based on a stepwise utilisation of HFNC, non-invasive ventilation (NIV) and ETI was used in the effort to reverse hypoxemia in these patients (figure 1). HFNC oxygen therapy was delivered using an AIRVO2 respiratory humidifier (Fisher & Paykel Healthcare, Auckland, New Zealand), with an integrated flow generator able to adjust FIO2 (between 0.21 and 1.0) and to deliver an air/oxygen mixture at flow rates of up to 60 L/min. The gas mixture (at 37°C) is routed through a circuit via large-bore bi-nasal prongs.
{kind=link}
Treatment algorithm. HFNC, high-flow nasal cannula; NIV, non-invasive ventilation; RR, respiratory rate; SaO2, arterial oxygen saturation.
HFNC was initially used at a 60 L/min gas flow rate and a FIO2 of 1.0; it was then adjusted to provide the minimum FIO2 necessary to maintain a SaO2 ≥92%. To reduce the risk of viral transmission, the patient wore a surgical mask and was instructed to breathe through a closed mouth as long as possible.
The patients were divided into two groups depending on their outcome: the first (success group) included patients who had a successful outcome, as defined by reversal of hypoxemia (SaO2 ≥92%), no need for NIV and/or invasive mechanical ventilation (IMV), discharge from RICU, with the patient alive and conscious for at least 48 hours after discharge. The second group (failure group) included patients who had an unsuccessful outcome, defined as the need for NIV or IMV by ETI and/or death while on HFNC support.
The patients’ baseline demographic and clinical features and clinical and laboratory data at RICU admission (also including SOFA score6) are outlined in table 1. Arterial blood gases were obtained while patients were receiving supplemental oxygen therapy via non-rebreathing mask with a reservoir bag.
Patients’ baseline demographic and clinical characteristics, and clinical and laboratory data at RICU admission
The male:female ratio was 3 to 1 (21 vs 7). The patients were classified, in accordance with the WHO criteria,4 as showing moderate (17 cases) or severe (11 cases) acute respiratory distress at the time they were admitted to the RICU.
Nineteen (67.8%) succeeded HFNC as hypoxemia was reversed and they were discharged from the RICU and were still alive on day 15 after discharge. Nine patients (32.2%) failed HFNC and received NIV. Five of them (17.8%) subsequently required IMV, of whom three died. All nine failing patients had lower PaO2/FIO2 (76 (53–190) vs 126 (52–296) mm Hg; p=0.0194) and higher serum C reactive protein level (130 (110–270) vs 110 (29–180); p=0.01277) with respect to their counterparts. Exact logistic regression following multivariate analysis indicated PaO2/FIO2 to be significantly associated with treatment failure (p=0.0314). Patients with PaO2/FIO2 at RICU admission ≤100 mm Hg showed a greater rate of treatment failure (7/9 (77.8%)), as opposed to those with PaO2/FIO2 >100 mm Hg (6/21 (31.6%); p=0.0246), with an OR of failure of 7.6 (95% CI 1.2 to 48.1).
Seventy-three healthcare workers (HCWs) (20 physicians, including residents, 40 nurses and 13 healthcare assistants) were exposed to confirmed cases of SARS-CoV-2 during the study period. Exposure duration was 48 (44–52) hours per person. All HCWs wore appropriate personal protective equipment, including gowns, hair covers, gloves, eye and face shields, and filtering face-piece respirator class 2 (FFP2) or 3 (FFP3), depending on the kind of manoeuvre performed, FFP3 being reserved for intubation, suctioning and bronchoscopy. All HCWs underwent nasopharyngeal swab on a weekly basis. HCWs who had fever or other COVID-19 signs and symptoms were immediately tested. COVID-19 swab PCR testing were negative in all our staff members during the study period and the following 14 days.
Our data suggest that HFNC played an important role in reversing hypoxemia in approximately two-thirds of the patients with SARS-CoV-2 with severe hARF unable to achieve SaO2 ≥92% under standard oxygen therapy. This improvement in oxygenation might depend on varied mechanisms, such as matching of delivered flow with increased ventilatory demand, achievement of high and stable FIO2 (up to 100%), upper airway washout, generation of positive pressure at end-expiration, and delivery of air heated and humidified.7 Noteworthy, PaO2/FIO2 at RICU admission had prognostic relevance. In fact, in keeping with previous work,1 patients with PaO2/FIO2 values ≤100 mm Hg had an increased risk of treatment failure.
Despite the use of HFNC as a means of respiratory support raises concerns for the increased risk of viral transmission,8 COVID-19 swab PCR testing resulted to be negative in all our staff members throughout the whole study period and in the following 14 days. In support of a limited risk of airborne transmission, recent data demonstrated the dispersion distance of exhaled gases during HFNC treatment to be quite limited.9 Worth remarking, we always applied a surgical mask over the nose and mouth of patients receiving HFNC.
Our study has limitations, such as the low number of patients enrolled and its retrospective nature, which may have caused a significant bias.
Despite these clear limitations, our data show that HFNC can be considered an effective and safe means to improve oxygenation in less severe forms of hARF secondary to COVID-19 not responding to conventional oxygen therapy.
Footnotes
Contributors AV: study design, manuscript preparation. BM: data collection and analysis. CT: data collection and analysis. GA: data collection, conduction of the study. AS: conduction of the study. GG: data collection, conduction of the study. FL: data collection, conduction of the study. GS: study design, data analysis. PN: manuscript preparation, revision of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.