

To the Editor:
There is an interesting game called “telephone” or “whispers,” in which a message is passed on, in a whisper, down a line of people, and then the last person speaks the message out loud. The final version of the message is usually radically changed from the original. Reference to this game is sometimes used to call attention to distorted information in research papers.
In the July issue of Respiratory Care, Mark Siobal and colleagues presented an elaborate and well conducted study comparing ventilatory volumetric capnography to other methods.1 While I am reluctant to criticize such a good paper, some minor mathematical errors crept in that reminded me of the whisper game.
In the Discussion section, on page 1149, the important equation relating the partial pressure of CO2 in arterial blood, CO2 production, and minute alveolar ventilation is presented as:
 A simple dimensional analysis shows that this equation is wrong (a whisper error?) The left hand side of the equation has units of pressure, but the right hand side of the equation is dimensionless (ie, units of flow in the numerator cancel units of flow in the denominator). The correct version of this equation is:
A simple dimensional analysis shows that this equation is wrong (a whisper error?) The left hand side of the equation has units of pressure, but the right hand side of the equation is dimensionless (ie, units of flow in the numerator cancel units of flow in the denominator). The correct version of this equation is:
 where the symbol, ∝ means “is proportional to.” In Siobal's paper1 the equation also appears in Figure 7 (same page), and they reference a paper by Tusman et al,2 who give a simplified version of the equation:
where the symbol, ∝ means “is proportional to.” In Siobal's paper1 the equation also appears in Figure 7 (same page), and they reference a paper by Tusman et al,2 who give a simplified version of the equation:
 where K is called “a constant” without further explanation. (Note that the above equation from the paper has a typo: it is missing the dot over the V in the numerator. The dot is a mathematical symbol denoting the derivative, in this case meaning the change in volume with respect to time: ie, flow).
where K is called “a constant” without further explanation. (Note that the above equation from the paper has a typo: it is missing the dot over the V in the numerator. The dot is a mathematical symbol denoting the derivative, in this case meaning the change in volume with respect to time: ie, flow).
The traditional and more useful form of the equation is:
 where PaCO2 = arterial carbon dioxide tension (mm Hg), V̇CO2 = carbon dioxide production (mL/min), and V̇A = alveolar ventilation (L/min).
where PaCO2 = arterial carbon dioxide tension (mm Hg), V̇CO2 = carbon dioxide production (mL/min), and V̇A = alveolar ventilation (L/min).
The factor 0.863 converts concentration to partial pressure and also corrects for the fact that CO2 production is usually expressed at standard temperature and pressure dry (STPD), whereas alveolar ventilation is expressed at body temperature and pressure saturated (BTPS).3 I contend that this form is more useful because it allows actual calculations using real or simulated data.
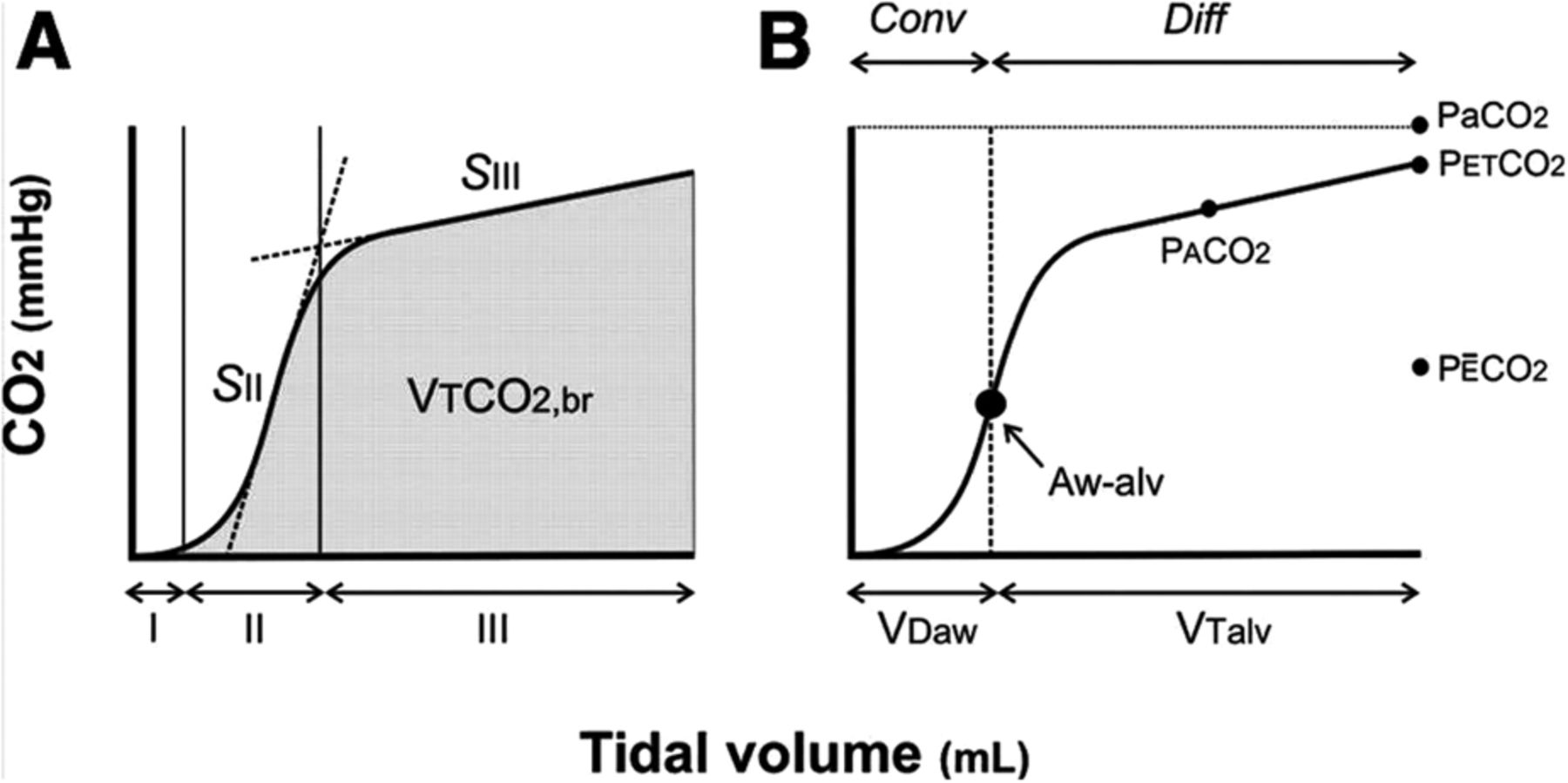
Another whisper error: Siobal et al present the graphic shown in Figure 1 (their Fig. 8). In this figure, the quantity VD-alv is represented as the “shaded areas” between the volume curve and the CO2 axis. Although the vertical axis is labeled simply CO2, there are horizontal lines labeled PaCO2, PACO2, et cetera, implying that the unit of measurement for the vertical axis is mm Hg. The reference is again the paper by Tusman et al.2 Out of curiosity, I looked up that paper and found a very similar graphic (Fig. 2). Note that in Figure 2 the volume axis is labeled in units of mL, and the CO2 axis is labeled in units of mm Hg. This is ok for graph B, because all the points on the graph are either volumes or pressures. But it is not ok for graph A. As with the first equation I mentioned, labeling the CO2 axis in units of pressure is incorrect, based on a simple dimensional analysis. The areas indicated are supposed to be volumes, but the units of those areas would be mL × mm Hg. The problem is that this figure got corrupted when it was “whispered” from its original source.
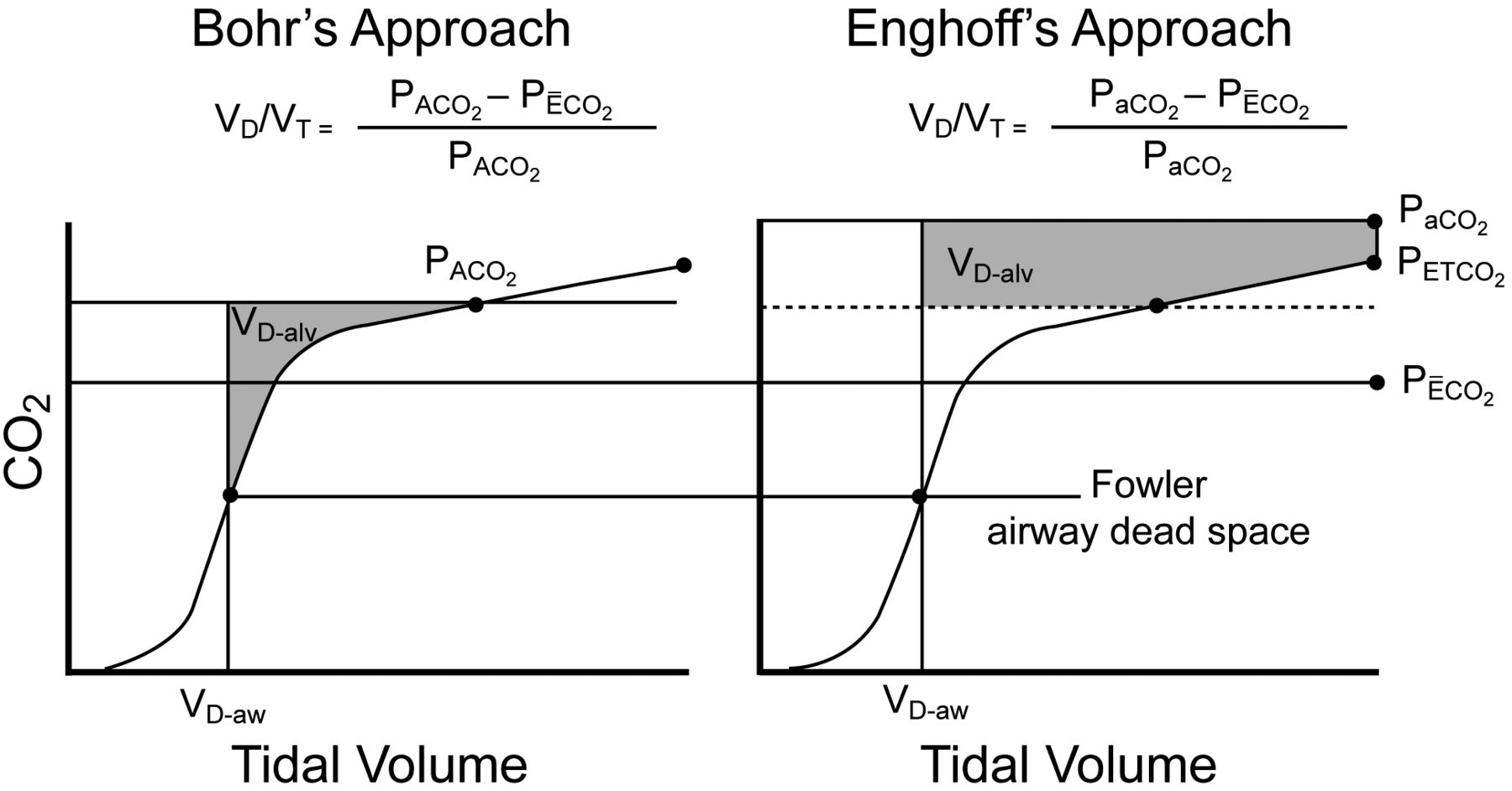
Figure 8 from Siobal et al.1

In that source, Fowler4 showed the vertical axis as CO2 concentration expressed as a fraction. Fletcher et al,5 who were referenced by Tusman et al,2 seem to have written the original article describing volumetric CO2 monitoring. They showed several graphs of volume versus fraction of CO2. Area in units of a fraction times volume yields the units of volume, as required. Tusman et al even state explicitly “The advantage of using fractions of carbon dioxide compared with partial pressure is that each area represents a volume of carbon dioxide, real or theoretical.”2
You may think the above issues are trivial matters, not worth mentioning. If you are a clinician whose main interest is basic concepts, perhaps you would be right. But if you were a researcher trying to analyze raw data, an educator trying to make a simulation with a spreadsheet, or an engineer trying to design software for a monitor, these errors could be quite confusing if you were new to the subject.
Finally, I will mention a small logical inconsistency that appears throughout the literature regarding mean exhaled fraction of CO2. The term “fraction of carbon dioxide in mixed expired gas,” symbolized as F̄ECO2 is attributed by Fletcher et al5 to Bohr.6 In that symbol the bar above the E indicates that it is a mean value. Indeed, the procedure for calculating the fraction of mixed expired gas was, historically, to collect several minutes of exhaled breaths in a large “Douglas bag” and measure the fraction of gas in the bag. Mathematically this gives the mean fraction per breath, and is analogous to measuring a minute's worth of exhalations and dividing the minute volume by the frequency to get the mean tidal volume. If you agree with this line of reasoning, then the symbol should be F̄ECO2 or ̄PECO2 This is admittedly a minor point, but I think it illustrates a general tendency among authors to simply pass on what previous authors have said (or what they think they said) without question.
In summary, an easy way to check mathematical expressions in manuscripts is to perform simple dimensional analyses. If the units are not the same, the equation is wrong.
Footnotes
Mr Chatburn has disclosed relationships with Dräger, Hamilton, CareFusion, Covidien, ResMed, Philips, IngMar, Radiometer America, Teleflex, Strategic Dynamics, Breathe Technologies, and the Alpha-1 Antitrypsin Foundation.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}