Article Text

Statistics from Altmetric.com
Nasal polyposis is a multifactorial disease with a complex and still not completely understood pathogenesis. In more than one third of cases it is associated with intolerance to acetylsalicylic acid (aspirin, ASA) or to other non-steroidal anti-inflammatory drugs (NSAIDs).1 In as many as 20% of cases nasal polyposis is also associated with the presence of bronchial asthma and/or rhinitis, configuring the so-called ASA triad or aspirin disease.2
Nasal polyps may benefit from medical treatment (corticosteroids) and surgery,3 but they frequently relapse soon after surgery4-9 with significant morbidity and high social and medical costs. Unfortunately, the effect of treatment with steroids is also often temporary.3 ,10-16
In the last two decades it has been observed that, in aspirin sensitive patients, oral aspirin desensitisation (followed by long term aspirin treatment) often results in an improvement in the clinical course of nasal polyposis.17-21 We have shown that aspirin sensitive patients with nasal polyposis have a higher rate of positive nasal provocation tests (rhinomanometric measure of nasal airflow reduction after exposure to the drug) with lysine-acetylsalicylate (LAS) than aspirin sensitive patients without nasal polyps.22-24 Moreover, LAS has been found to have an in vitro non-specific antiproliferative, dose dependent effect on the growth of fibroblasts of both nasal polyps and normal skin.23 We have shown that long term topical (endonasal) treatment with LAS prevents the recurrence of nasal polyps after polypectomy with satisfactory results.24
In this paper we present and discuss the definitive results obtained in two controlled long term prospective follow up studies dealing with the evaluation of relapse rates in nasal polyposis.
The first is a six year follow up study of patients with nasal polyps who underwent long term intranasal LAS treatment after surgical polypectomy in comparison with matched controls (patients who underwent simple polypectomy with no further treatment). The cumulative percentage of patients in whom polyps did not recur during the follow up period was evaluated by the life table method and compared with that of controls using a χ2 log rank test.25 This first controlled follow up will be referred to as “SP-LAS” (surgical polypectomy + LAS treatment). In the second controlled study a group of patients suffering from nasal polyposis (in whom surgery was indicated) received a “medical” polypectomy (corticosteroids) followed by long term topical LAS treatment instead of surgery. A successive three year prospective follow up was completed. This second follow up study will be referred to as “MP-LAS” (medical polypectomy + LAS treatment).
Methods
SELECTION OF PATIENTS
In both studies consecutive patients suffering from nasal polyposis were followed as outpatients at the Department of Allergology of Policlinic A Gemelli, Rome, Italy. In all cases a diagnosis of nasal polyposis was established by means of clinical criteria (ENT examination including rhinoscopy, standard skull radiographs, and computed tomographic (CT) scan of the nasal and paranasal cavities). The severity of symptoms (impaired quality of life despite appropriate medical treatment, chronic nasal congestion, recurrent infections, bone erosion, mucoceles, worsening asthma, or other complications) indicated surgery in all patients.
According to the principles of the Helsinki declaration, informed consent to the entire protocol was obtained from each patient.
All subjects underwent a complete allergological evaluation including skin prick tests with the commonest inhaled allergens (Graminae, Parietaria, olive, cat, dust mite,Aspergillus,Penicillium,Alternaria; ALK-Abello, Madrid, Spain). Serum total (PRIST, Pharmacia) and specific (RAST, Pharmacia) IgE determinations were also performed.
A nasal provocation test (NPT) with LAS was performed in all subjects. NPT measures, by means of anterior rhinomanometry,26-28the percentage decrease in nasal airflow following the inhalation of increasing doses of the specific allergen. The NPT response was considered positive if inhalation of the specific allergen resulted in a reduction in airflow of more than 40% of the basal value. In patients with a positive skin prick or RAST test an NPT was also performed, inhaling the specific allergen to confirm the occurrence of any hypersensitivity. After measuring basal (untreated) nasal airflow, non-specific hyperreactivity of the nasal mucosa was excluded by measuring nasal airflow before and 10 and 20 minutes after inhaling saline (2 ml, 0.9%). Thereafter, an initial dose of 20 μg LAS in 2 ml saline was administered. Nasal airflow was evaluated 10 and 20 minutes after the allergen challenge. Where the NPT response was negative, 200 μg LAS and, if further negative, 2 and 4 mg LAS were administered, with an interval of 20 minutes, recording nasal airflow 10 and 20 minutes after inhalation. Nasal airflow was also determined 60 and 360 minutes after the positive response to identify any delayed response.
In both studies a complete ENT examination and a CT scan of the skull were performed every 6–12 months in all patients admitted to the follow up.
SP-LAS STUDY
Seventy six consecutive patients with nasal polyps (41 men, 35 women) aged 14–71 years were enrolled over an eight year period (1988–95). According to ENT indications, all patients underwent surgical ablation (Pietrantoni-De Lima technique). About one month after surgery inhalation treatment with LAS (six times/week) was started. The initial dose corresponded to 20 μg aspirin, progressively increasing to a maintenance dose corresponding to 4 mg aspirin six times/week.
MP-LAS STUDY
Forty nine patients (21 men, 28 women) aged 19–71 with nasal polyps in whom surgery was indicated were admitted to the follow up study during the period 1995–8. In all subjects a simple “medical polypectomy” was performed, administering 40 mg triamcinolone retard intramuscularly every 10 days (three administrations, total dose 120 mg). Such a treatment achieves a decrease (at least temporary) in polyp volume and facilitates penetration of LAS into the rhinosinusal cavities. Thereafter, increasing doses of LAS were administered by inhalation according to the protocol described for the SP-LAS study.
CONTROL SUBJECTS
Both the follow up studies shared the same control population consisting of 191 age matched subjects suffering from nasal polyposis (101 men, 90 women, age 16–70) who had previously undergone surgical polypectomy with no further medical treatment. This group of patients may represent a somewhat “improper” control population for the MP-LAS study which involves patients who did not undergo any surgical polypectomy. However, the MP-LAS prospective study cannot have a “natural” control group since obvious ethical considerations prevent follow up without any further treatment (besides initial corticosteroids) in a population of patients suffering from severe nasal polyps in whom surgery is indicated.
STATISTICAL ANALYSIS
In both the follow up studies the rates of recurrence of nasal polyps were evaluated by the life table method.25 This statistical tool is able to include in the analysis data on subjects abandoning the study at any time, evaluating at any considered time interval the actual number of patients still at risk. The difference in rates of recurrence of the investigated patients and the control subjects were evaluated by the log rank test25 which gives a “relative” rate of recurrence for each investigated population. Such a figure represents the ratio between the average recurrence rate of the patients and the overall (investigated subjects and controls) averaged rate of recurrence of polyps (that is arbitrarily set at 1.00). This permits an easy and global quantitative comparison between different populations and the computing of appropriate χ2statistics.
Results
SP-LAS STUDY
Thirty eight (50%) of the 76 enrolled patients had aspirin sensitivity (mainly with asthmatic symptoms) and in 28 subjects (36.8%) the complete aspirin triad syndrome was diagnosed. A moderate to severe degree of anosmia was present in 62 patients (81.6%), in 72.6% of cases associated with aspirin intolerance.
Thirty patients (39.5%) had positive skin prick tests (19 toDermatophagoides, eight to Graminae, and three to Parietaria); these subjects had a history of rhinitis (19 patients) or asthma (11 subjects). However, a true allergic reaction (positive RAST and/or specific NPT) was detected in only 25 subjects (32.9%).
LAS treatment was well tolerated by all patients and no adverse reactions were observed. LAS-NPT was positive in 24 cases (31.6%).
The results of the SP-LAS prospective study are summarised in fig 1which shows the cumulative percentages (life table method) of patients in whom there was no recurrence of nasal polyps after polypectomy over the six year follow up period. A highly significant statistical difference was seen between the relapse rates of LAS treated subjects and controls (χ2 13.4; df = 1; p<0.001, log rank test). The relative relapse rate of the controls (1.40) was nearly twice that of the treated patients (0.78). The percentage of controls in whom nasal polyps had not recurred was 48.7% at one year, declining to 15.2% after three years and to 6.5% six years after surgery. Conversely, 93.1% of patients treated with LAS were relapse-free at one year, 55.1% at three years, and nearly 35% six years after surgery.

SP-LAS follow up results: cumulative percentage relapse of nasal polyposis after surgery (life table method).
No statistical difference in the cumulative rates of recurrence were found between aspirin tolerant and aspirin sensitive treated patients and controls.
MP-LAS STUDY
Twenty five of the 49 investigated patients (51.0%) were aspirin sensitive (mainly with asthmatic symptoms; only three patients had urticaria-angioedema). In 14 cases (28.6%) the complete clinical picture of the aspirin triad was evident. Most patients (87.8%) had anosmia (in 72.1% of cases associated with sensitivity to aspirin).
Twenty patients (40.8%) had positive skin tests (13 toDermatophagoides, five to Graminae and two to Parietaria); 11 had rhinitis and nine had symptoms of asthma. However, a true allergic reaction (positive RAST and/or specific NPT) was detected in only 10 subjects (20.4%).
Treatment with LAS and NPT were well tolerated by all patients and no adverse reactions were observed. LAS-NPT was positive in 16 cases (32.6%).
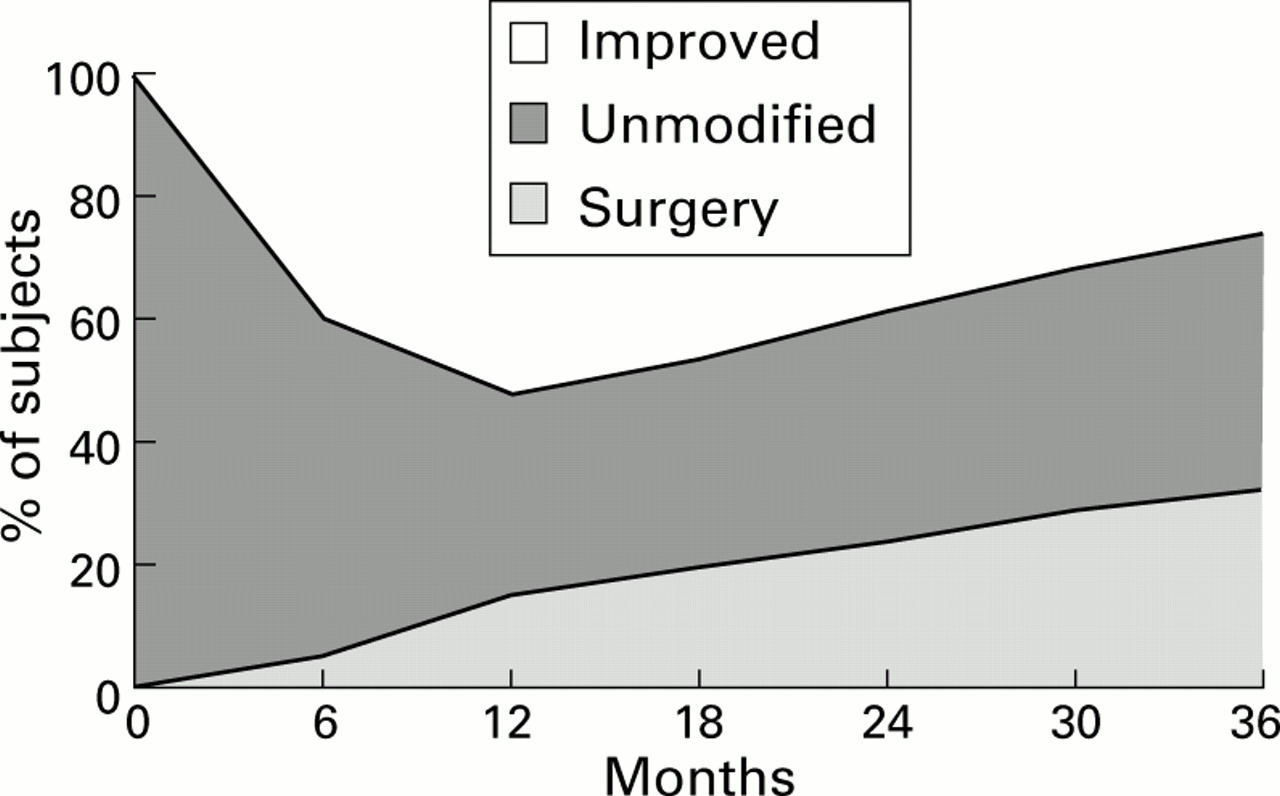
Figure 2 summarises the results obtained in the three year MP-LAS follow up. The percentage of patients whose symptoms and clinical picture improved after LAS treatment (with no surgical polypectomy) was 42.4% after six months, 54.3% at one year, and was nearly 30% after three years. These figures are not statistically different (log rank test) from the relapse-free rates obtained in controls (who did undergo surgical polypectomy), which did not reach 50% one year after surgery and were 15% three years after polypectomy (fig 1). As already stated, such a comparison may be somehow improper and it should be regarded just as indicative.
{kind=link}
{kind=link}
MP-LAS follow up results: cumulative percentage of subjects with polyposis after “medical” polypectomy (corticosteroids) followed by topical LAS treatment (life table method).
About one third of the patients treated with LAS showed no change in nasal polyps after three years of treatment (fig 2). The cumulative percentage of patients in whom the disease worsened and who therefore had to be treated surgically was just 3.8% in the first six months, rising to 13.1% after one year and to 32% at the end of the three year follow up. These last figures appear to be surprisingly low in a population of patients suffering from severe nasal polyps requiring surgery.
As in the SP-LAS study, no statistical difference was observed in the rates of recurrence of nasal polyps between aspirin tolerant and aspirin sensitive subjects.
Discussion
Our results indicate that long term topical treatment with LAS may be clinically effective in nasal polyposis. The potential effectiveness of topical LAS in the prevention of recurrence of nasal polyps after surgery has already been reported24 ,29 and our preliminary results have substantially been confirmed by other authors.30 The present study provides further evidence of the effectiveness of LAS treatment following surgery in patients with nasal polyposis, and demonstrates also the favourable effects of LAS in patients who did not have surgery even though surgery was indicated.
The favourable effect of LAS in nasal polyposis is probably due to its non-specific anti-inflammatory properties rather than to desensitisation since LAS is highly effective in both aspirin tolerant and aspirin sensitive patients. These findings are confirmed by a previous report23 of the inhibitory effect of LAS on the growth of cultures of nasal polyps on normal skin fibroblasts from aspirin tolerant and aspirin sensitive patients. It was dose dependent, non-specific, and “cytostatic” since cell viability was always as high as 85%.
Long term topical treatment with LAS is almost free of side effects and it may therefore be used in subjects known to be at risk, such as those suffering from the aspirin triad.
In conclusion, in patients with nasal polyposis a medical approach should always be performed before surgery which has, in most cases only, transient results.