Article Text

Statistics from Altmetric.com
We read with interest the article ‘The atoll sign’ by Walsh and Roberton1 in the November issue of Thorax. The authors report a case of cryptogenic organising pneumonia with the atoll sign, also called the reversed halo sign. As mentioned by the authors, this CT sign was first described in cryptogenic organising pneumonia and was initially considered to be specific for this disease.2 It was subsequently reported in a variety of pulmonary diseases, including paracoccidioidomycosis (South American blastomycosis), tuberculosis, pulmonary sarcoidosis, lymphomatoid granulomatosis, Wegener's granulomatosis, lipoid pneumonia and pneumococcal pneumonia.3–5
We would like to highlight another important cause of the reversed halo sign: invasive pulmonary fungal infections, particularly pulmonary zygomycosis (PZ) (figure 1). In immunosuppressed patients, the presence of the reversed halo sign on CT should be considered as invasive fungal disease until proven otherwise. It is an early sign that is more frequently seen in patients with PZ than invasive pulmonary aspergillosis (IPA).6

{kind=link}
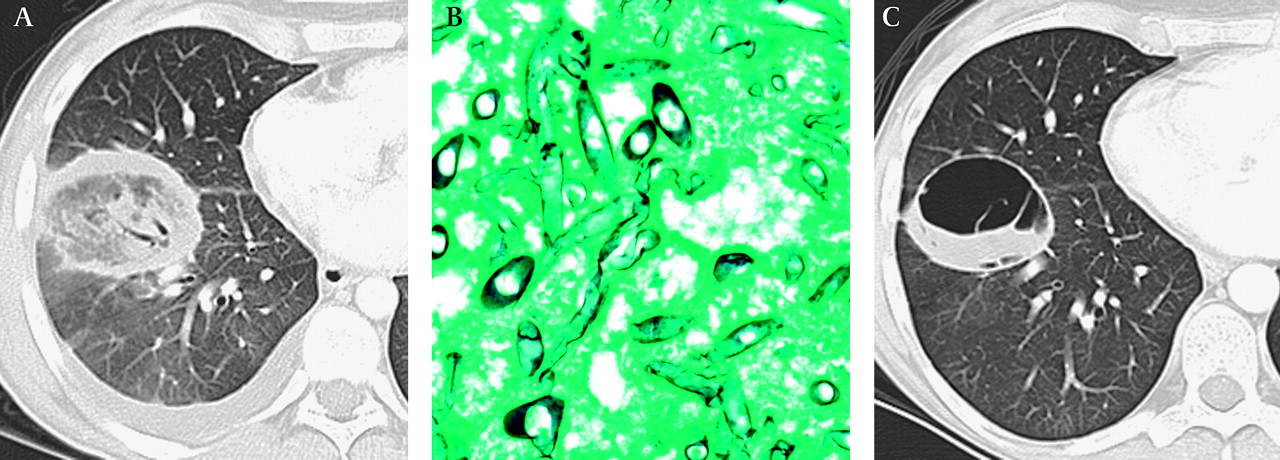
Pulmonary zygomycosis in a 24-year-old woman undergoing chemotherapy for recurrence of acute myelogenous leukaemia, 1 year following allogeneic stem cell transplantation, with a 2-week history of fever and dry cough. (A) Chest CT shows a focal round area of ground-glass attenuation surrounded by a ring of consolidation in the right lower lobe, consistent with the reversed halo sign. (B) Photomicrograph of the specimen from a transthoracic biopsy of the lesion shows pauciseptated hyphae with non-parallel walls and 90° branching, characteristic of Zygomycetes species, which is confirmed by culture. (C) One-month follow-up CT shows cavitation of the lesion, which eventually resolved under antifungal therapy.
Early institution of high-dose antifungal therapy is associated with improved outcomes; therefore, early recognition of invasive fungal disease is important. Moreover, because the therapy for presumed fungal pneumonia in this population is often aimed at IPA due to its higher incidence and the preferred antifungal agent for IPA is voriconazole, which is not effective against PZ, it is important to differentiate between the two entities. The presence of the reversed halo sign can be used to optimise antifungal therapy to cover PZ.
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; not externally peer reviewed.