Article Text

Statistics from Altmetric.com
- COPD complications
- COPD exacerbations
- COPD treatment
- cough/mechanisms/pharmacology
- emission-computed
- imaging/CT MRI
- imaging, three-dimensional
- respiratory-gated imaging techniques
- tomography
- tracheomalacia
Tracheomalacia is a term used to describe weakness of the trachea. Strictly speaking, tracheomalacia means weakness of cartilaginous structures of the trachea, while excessive dynamic airway collapse (EDAC) describes invagination of the posterior membrane of the trachea leading to a ≥50% reduction in airway lumen.1 Tracheomalacia and EDAC are thought to exist in a significant portion of patients suffering from chronic obstructive pulmonary disease (COPD).2
An 88-year-old man presented with a 2 day history of episodic dyspnoea, wheeze and non-productive cough, on a background of COPD. Despite treatment with oral steroids and short-acting bronchodilators the patient remained symptomatic.
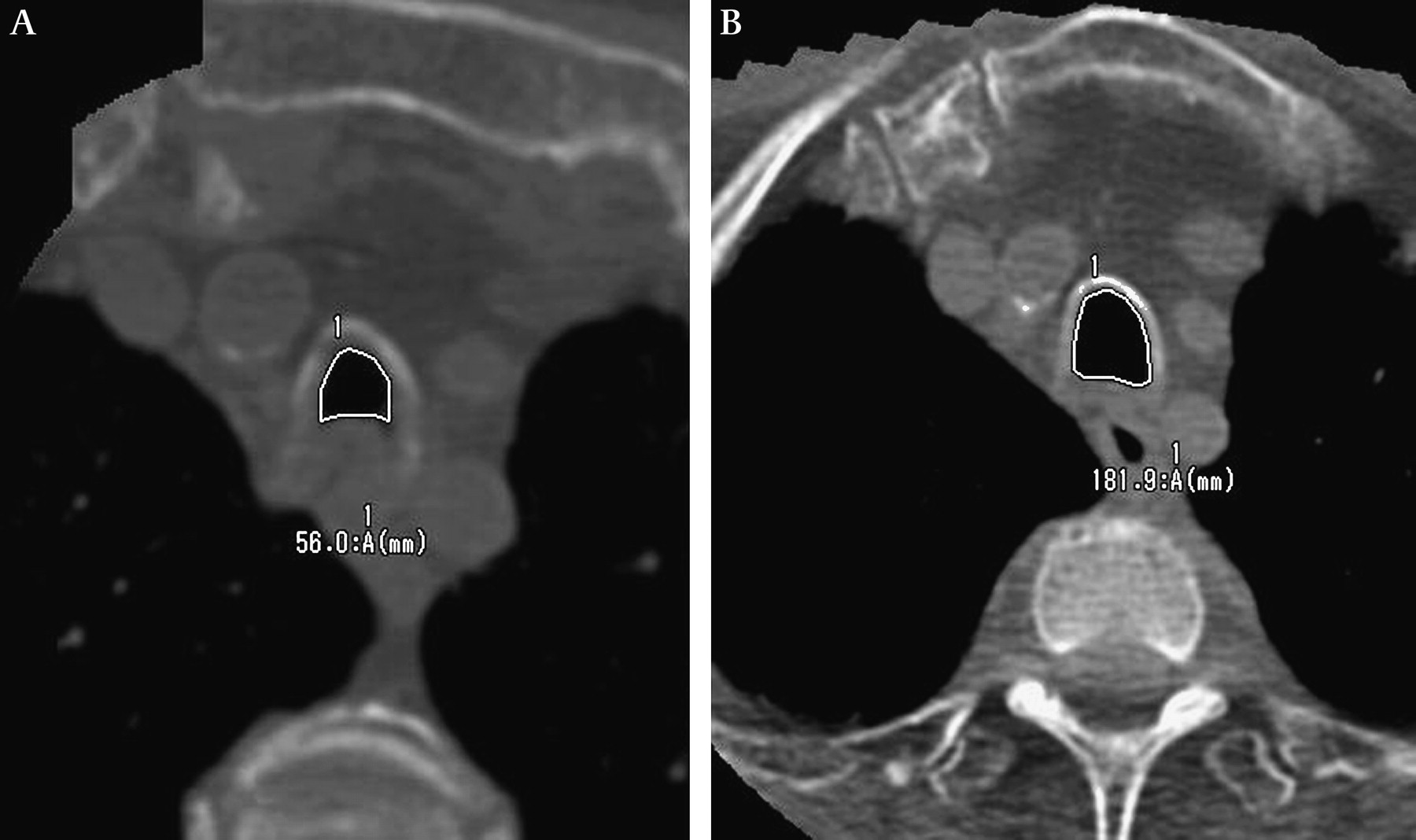
A 320-slice, dynamic CT scan of the patient's upper airway revealed EDAC along the posterior intrathoracic tracheal wall (see figures 1 and 2):
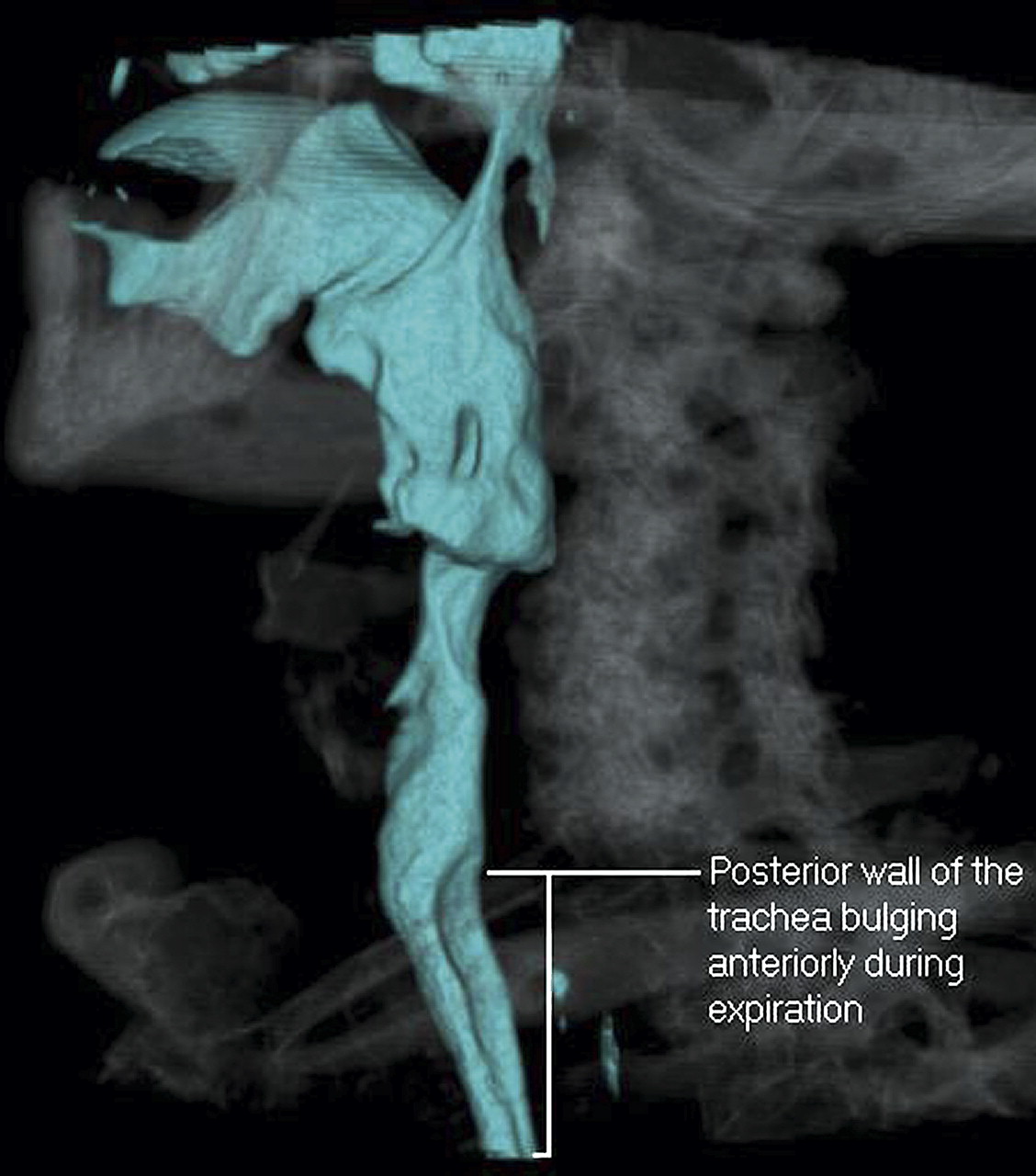
Three-dimensional reconstruction demonstrating collapse of the posterior trachea on expiration.

(A) Full expiration. (B) Full inspiration. Invagination of the posterior tracheal wall into the tracheal lumen during expiration, reducing the lumen by >50% and creating a crescent shape.
Continuous positive airways pressure (CPAP) was applied at 10 cm H2O in order to abolish the patient's symptoms. Repeat 320-slice CT scan of the neck with CPAP in situ demonstrated amelioration of the EDAC (see figure 3 and figure 4).

Three-dimensional reconstruction revealing amelioration of posterior wall bulging while on continuous positive airway pressure (CPAP) at 10 cm H2O during full expiration.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Full expiration without continuous positive airway pressure (CPAP). (B) Full expiration with CPAP.
The reference gold standard for diagnosing tracheomalacia and EDAC is bronchoscopy, which is problematic during acute episodes of dyspnoea. Recent advances in technology have enabled dynamic cine viewing of the upper airway in a less invasive manner. This can be performed rapidly and safely during acute episodes of dyspnoea.3 The images obtained during this study were conducted at a dose of 7.2 mSv which is comparable with the dose received during a standard CT chest. Since this case study we have further refined our technique, enabling similar imaging at a reduced dose of 2–4 mSv.3 Dynamic 320-slice cine CT scan is therefore a safe and helpful tool in diagnosing dynamic airway collapse in elderly subjects. In younger patients (eg, <50 years), 320-slice CT scanning may also be extremely useful, but clinicians should take into account the potential effects of radiation exposure in a given individual.
Learning points
Excessive dynamic airway collapse can co-exist with chronic obstructive pulmonary disease.
Dynamic 320-slice CT scanning represents an alternative to fibre optic bronchoscopy in the diagnosis of excessive dynamic airway collapse.
Continuous positive airway pressure may be applied to individual patients with excessive dynamic airways collapse to ameliorate collapse of the trachea.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.