

Abstract
BACKGROUND: The statement of the American Thoracic Society and European Respiratory Society on the measurement of static lung volumes (SLV) suggests a preferred and alternate method for measuring and calculating SLV.
OBJECTIVE: To determine if differences in functional residual capacity (FRC), vital capacity (VC), residual volume (RV), and total lung capacity (TLC), obtained using preferred and alternate measurement and calculation methodologies, exist in a clinical setting.
METHODS: Patients attending for SLV at a hospital-based laboratory were recruited. Following spirometry, SLV was measured via body plethysmography, using the preferred and alternate methods in random order. Volumes were calculated using the preferred and alternate calculation methods. Subjects were classified according to standard ventilatory function interpretative strategies. Differences of the means between the measurement methods, and calculation methods were assessed.
RESULTS: One hundred eight data sets were analyzed. Significant, but small differences (< 150 mL) in the means for VC and TLC, and RV and TLC were found in the normal and restricted groups, respectively. No significant differences in SLV parameters were found in subjects with air-flow obstruction. Twelve of the 108 changed ventilatory function classification between methods, with the alternate method delivering a lower inspiratory capacity and TLC without a change in RV in 66% of this subgroup. Identical results were obtained when data were analyzed using both calculation methods.
CONCLUSIONS: Differences in FRC, VC, RV, and TLC obtained using the preferred and alternate measurement methodologies exist in the clinical setting in select classification groups and individuals. Differing calculation methods dependent on measurement method used may be unnecessary.
Introduction
The measurement of static lung volumes using body plethysmography is routinely performed worldwide. In body plethysmography's infancy, thoracic gas volume at functional residual capacity (FRC) was the primary measure recorded. Separate measures of inspiratory capacity (IC), expiratory reserve volume (ERV), and vital capacity (VC) via spirometry were used to calculate total lung capacity (TLC) and residual volume (RV).1
Subsequent advances in technology allowed spirometry maneuvers, linked to FRC measurements, to be performed in body plethysmographs. Consequently, the number of methods for data collection and calculation techniques multiplied. However, corresponding studies examining the effect of the various measurement and calculation methodologies on reported values are sparse and do not wholly reflect current test methodologies or devices.2,3
In an attempt to standardize the measurement of static lung volumes, the American Thoracic Society and European Respiratory Society (ATS/ERS) have documented 2 methods for measuring static lung volumes via plethysmography.4
Measurement Technique 1
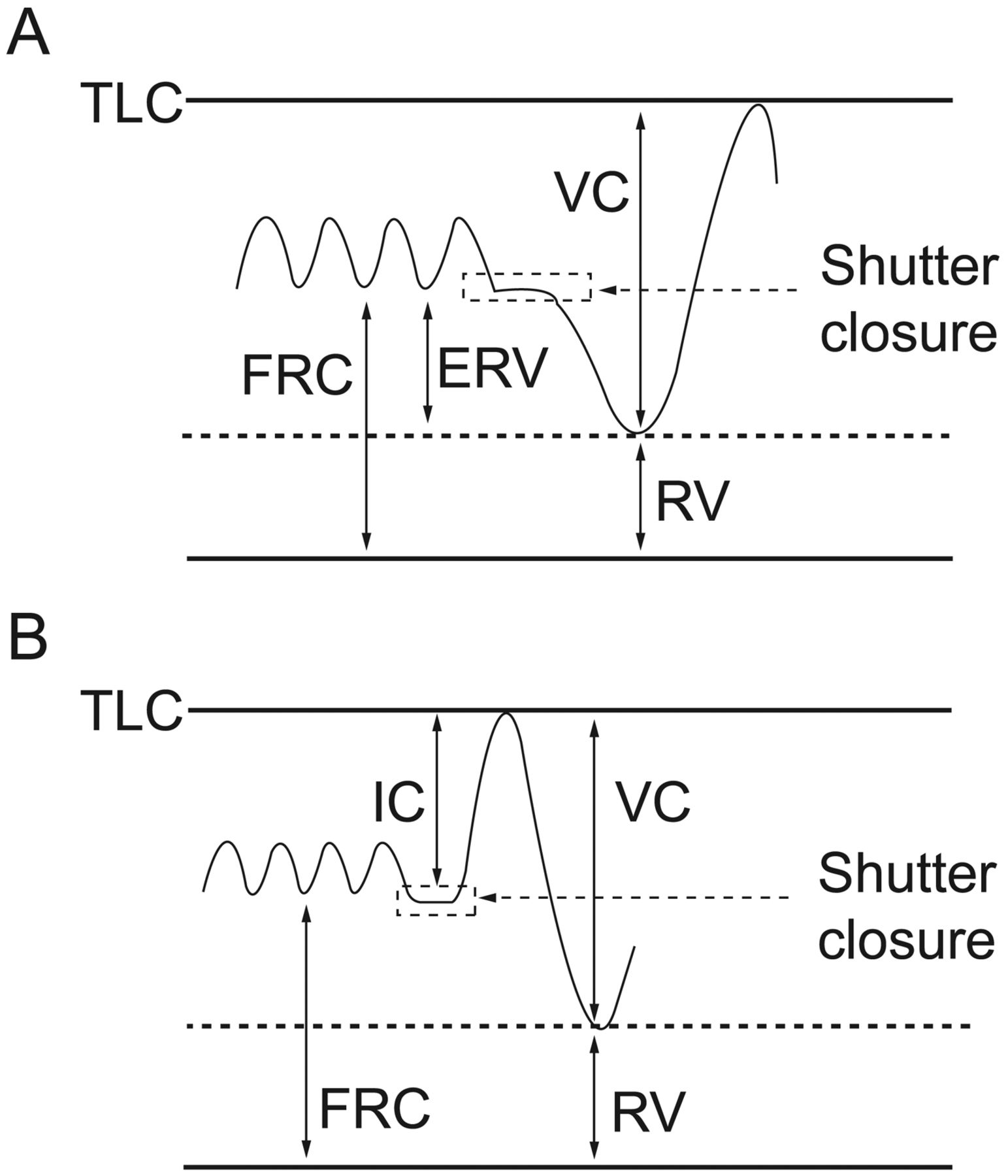
Following shutter closure at FRC, an expiratory maneuver to RV is performed, followed by an inspiratory VC maneuver to TLC (Fig. 1A).

Methods for measurement of total lung capacity (TLC) and residual volume (RV) via body plethysmography. A: Functional residual capacity (FRC) is measured during shutter closure. The subject then exhales to RV before taking a vital capacity (VC) breath to TLC. B: FRC is measured during shutter closure. The subject then takes an inspiratory capacity (IC) breath to TLC before exhaling a VC breath to RV.
Measurement Technique 2
Following shutter closure at FRC, an IC breath is taken to TLC, followed by an expiratory VC breath to RV (Fig. 1B).
Technique 1 was chosen, by consensus, as the preferred method of testing, as it was postulated that the RV was likely to be higher using technique 2, the alternate method, in individuals with obstructive lung disease. The mechanism by which a higher RV results in those with obstruction using the alternate method is not described in the ATS/ERS statement and there appears to be little evidence to support this hypothesis.
The ATS/ERS task force also recommends different methods for calculating the reported FRC, TLC, and RV.4
Calculation Method 1
FRC: The mean FRC of 3 technically acceptable and repeatable maneuvers with acceptable linked ERV and inspiratory VC measurements
RV: The mean FRC minus the mean of the 3 technically acceptable ERV measurements linked to the technically acceptable FRC measurements
TLC: The reported RV value plus the largest technically acceptable inspiratory VC
Calculation Method 2
FRC: The mean of 3 technically acceptable FRC measurements used for the calculation of TLC
TLC: The mean of the 3 largest sums of technically acceptable FRC and linked IC values
RV: The mean TLC minus the largest VC measured
Calculation method 1 is used when measurement technique 1 (the preferred method) is used, and calculation method 2 is used when measurement technique 2 (the alternate method) is used. It is not apparent why different methods of calculation of results are required. Nor is the affect of different calculation methods on reported values known.
The aims of the study were to identify any differences in FRC, VC, RV, and TLC obtained using the preferred and alternate methodologies in contemporary body plethysmographs across ventilatory function classifications in a clinical setting, and to compare the values of TLC and RV calculated using the preferred and alternate calculation techniques.
QUICK LOOK
Current knowledge
The American Thoracic Society and European Respiratory Society have issued a guideline on the measurement of static lung volume, suggesting a preferred and alternate method for measurement.
What this paper contributes to our knowledge
Differences in functional residual capacity, vital capacity, residual volume, and total lung capacity obtained with the preferred and alternate methods did not result in significantly important differences. The use of different calculation methods based on the measurement methods may be unnecessary.
Methods
Following approval from the Alfred Hospital ethics review committee (137/07), consecutive patients, referred to the lung function laboratory for measurement of static lung volumes, were invited to participate. Participants gave informed written consent.
Tests were performed in a Thoracic Society of Australia and New Zealand accredited lung function laboratory within a tertiary medical facility, using calibrated, constant volume, variable pressure body plethysmographs (Elite and Platinum Elite, Medical Graphics, St Paul, Minnesota). Each device was included in the laboratory's quality control program.
The study was a randomized, cross-over design. Spirometry was performed according to ATS/ERS standards.5 Plethysmographic measures of static lung volumes were then obtained using the preferred and alternate methods of the ATS/ERS standards for each subject in random order,4 as follows:
Following a brief explanation of the first test methodology, the subject entered the plethysmograph, the door was sealed and temperature equilibration was attained. The subject was then instructed to attach to the mouthpiece, and, with nose pegs in place and hands supporting cheeks, commence tidal breathing. Following at least 4 tidal breaths and observation of a stable end-expiratory volume, the mouthpiece shutter was closed at or near FRC and subjects performed small, gentle pants against the closed shutter at a frequency of approximately 1 Hz until the shutter reopened. Without coming off the mouthpiece, subjects were then instructed to exhale completely to RV and then inhale completely to TLC if performing the preferred test methodology. If performing the alternate test methodology, without coming off the mouthpiece, subjects were instructed to inhale completely to TLC, followed by a complete exhalation to RV. Subjects could then come off the mouthpiece.
A minimum of 3 maneuvers, and generally a maximum of 5 maneuvers, were performed to obtain 3 acceptable and repeatable FRC measurements. Scientists could attempt more than 5 maneuvers if 3 acceptable efforts had not been achieved within 5 maneuvers and they thought the subject was capable of getting 3 acceptable efforts with a few more attempts.
The second test methodology was then explained and performed as described above, following completion of the first test methodology. The scientist performing the test determined if a short break was required between efforts and/or test methodologies, as happens in usual clinical practice.
Subjects were encouraged to complete the VC maneuver immediately following FRC determination, but a couple of small breaths, without coming off the mouthpiece, were allowed if necessary. Subjects were actively discouraged from coming off the mouthpiece between FRC determination and VC measurement, and in cases where this occurred, the effort was not used.
Data Quality
FRC measurements were acceptable when pants against a closed shutter were represented by “a series of almost superimposed straight lines separated by only a small amount of thermal drift on the pressure-volume plot,” with a panting frequency of approximately 1 Hz.4
Tests were considered acceptable and repeatable when at least 3 acceptable FRC measurements within 5% of each other, each with a linked, technically acceptable VC maneuver, were obtained.4,5 Results were included in the analysis where acceptability and repeatability criteria were met for both the preferred and alternate method. Measurements not meeting the above criteria were excluded from further analysis.
For the VC maneuvers, plateaus were sought at each extreme of the VC maneuver, unless the subject could not or should not continue to blow.
Comparison of Measurement Techniques of the Preferred and Alternate Methods
Following data collection, the FRC, TLC, and RV were calculated.
For the preferred method:
FRC: The mean FRC of 3 technically acceptable and repeatable maneuvers
RV: The mean FRC minus the mean of the 3 linked ERV measurements
TLC: The recorded RV value plus the largest of the linked technically acceptable inspiratory VCs
For the alternate method:
FRC: The mean FRC of 3 technically acceptable and repeatable maneuvers
TLC: The mean of the 3 largest sums of technically acceptable FRC and linked IC values
RV: The mean TLC minus the largest of the linked technically acceptable VCs
Ventilatory function classifications, using standard interpretative strategies,6 were then allocated to each subject, using spirometry and static lung volumes. Static lung volumes from the first randomly selected measurement method were used to classify ventilatory function:
Ventilatory function within normal limits: FEV1/FVC, FVC, TLC, and RV/TLC all within normal limits
Obstruction: FEV1/FVC < lower limit of normal (LLN) and TLC > LLN
Obstruction with gas trapping: FEV1/FVC < LLN, TLC > LLN, and RV/TLC > upper limit of normal
Restriction: FEV1/FVC > LLN and TLC < LLN
Mixed obstructive/restrictive defect: FEV1/FVC < LLN and TLC < LLN
Results were compared to the reference values of Hankinson et al7 and Roca et al8 (spirometry and static lung volumes, respectively). For FEV1/FVC and TLC the LLN was defined as the reference value minus 1.64 SD. For RV/TLC the upper limit of normal was defined as the reference value plus 1.64 SD. Differences in the means between test methods for the parameters FRC, VC, RV, and TLC were sought for each classification group.
Comparison of the Preferred and Alternate Calculation Methods for RV and TLC
For FRC, ERV, and VC values collected via the preferred measurement method, TLC and RV were calculated using the preferred calculation method and the alternate calculation method:
Recorded RV: The mean of the 3 differences of individual, linked FRC and ERV measurements
Recorded TLC: The sum of recorded RV and the largest linked VC
For FRC, IC, and VC values collected using the alternate measurement method, TLC and RV were calculated using the alternate calculation method and the preferred calculation method:
Recorded TLC: The mean of 3 technically acceptable FRCs plus the mean of 3 linked ICs
Recorded RV: The recorded TLC minus the largest linked VC
Differences of the means between calculation methods were sought for RV and TLC for each measurement method.
Statistical Analysis
For 90% power, the number of subjects required to see a significant difference (P < .05) in RV was determined to be 22 per classification group, where a difference between methods of ≥ 200 mL was considered important. Paired Student t tests for parametric, and paired Wilcoxon signed rank tests for non-parametric data, were used to assess differences of the means.
Results
One hundred sixty-six subjects consented to participate over the recruitment period, in which 1,059 static lung volume measurements were made. Nine experienced respiratory scientists (bachelor degree minimum qualification) assisted in the collection of data. This reflected the clinical practice of the laboratory.
Quality of Static Lung Volume Measurements
Figure 2 outlines participant flow through the study. Sixteen subjects did not complete testing. Forty-two subjects did not meet FRC acceptability and repeatability criteria. One hundred eight subjects met FRC acceptability and repeatability criteria. No relationship between severity (based on FEV1 Z score) and ability to meet FRC acceptability and repeatability criteria was found (Wilcoxon 2-sample test P = .20).

CONSORT diagram showing the flow of participants through the study.
Classification of Ventilatory Function
Those who met the FRC acceptability and repeatability criteria for both the preferred and alternate methods (n = 108) were classified as having ventilatory function within normal limits (n = 27), obstruction (n = 38, with a subgroup of 23 also having gas trapping), restriction (n = 31), and mixed obstruction/restriction (n = 12). Table 1 outlines the subject demographics, using the static lung volumes results from the first randomly selected method for each subject. The study population was similar to the overall clinical population with respect to demographics and lung function when grouped into ventilatory defect classifications, except for RV/TLC, in the all obstruction group (mean RV/TLC 47% vs 53%, respectively) and BMI in the obstruction with gas trapping group (mean BMI 27.0 kg/m2 vs 24.6 kg/m2, respectively) (Table 2).
Demographics of Subjects With Complete and Acceptable Data
P Values for the Comparison of the Means of the Study Group and Clinical Population Tested During Study Duration (Wilcoxon 2 Sample Test)
Comparison of FRC, RV, TLC, and VC Between Preferred and Alternate Measurement Methods
A small but statistically significant difference in mean values between the preferred method and the alternate method was seen for VC and TLC in subjects with normal ventilatory function, and for RV and TLC in subjects with restriction (Table 3). No statistically significant differences in mean values between the preferred method and the alternate method were seen for FRC, RV, TLC, or VC in subjects with air-flow obstruction (see Table 3). Due to small numbers, the mixed defect group could not be reliably analyzed.
The Mean Difference Between Methods (Preferred Minus Alternate), With the 95% Confidence Limits for the Mean Difference,* in FRC, VC, RV, and TLC for Each Classification Group With > 22 Subjects
Changes in Classification of Subjects Between Methods
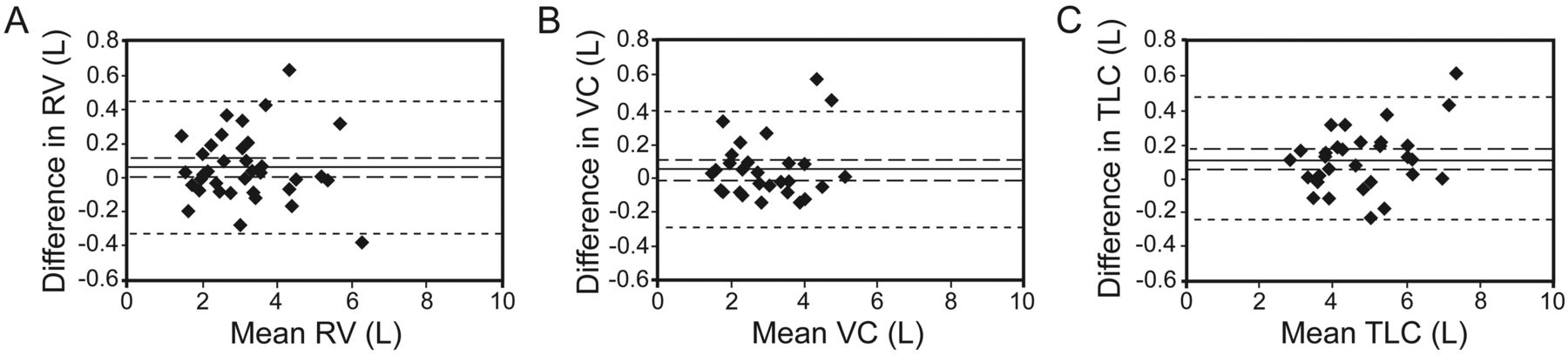
Twelve (11%) of 108 subjects changed ventilatory function classification between test methods (Table 4). Of these, 3 (3% of subjects) had one or more parameters where the difference between methods exceeded the reproducibility (mean difference ± 2 SD) between the methods (see Table 4, Fig. 3). A statistically significant difference in mean values between the preferred method and the alternate method was seen for TLC (P < .001) and IC (P < .001) in this subgroup of 12 subjects, the alternate method producing a smaller TLC and IC than the preferred method. No statistically significant differences in mean values between the preferred method and the alternate method were seen for FRC or RV.
Classification of Ventilatory Function: Subjects Who Changed Classification Between Test Methodologies

Bland-Altman plots of preferred – alternate method versus mean of the preferred and alternate methods for (A) residual volume (RV) for the obstructive group, (B) vital capacity (VC) for the restrictive group, and (C) total lung capacity (TLC) for the restrictive group. Each plot shows points outside the reproducibility limits of the 2 methods, which led to changes in classification between methods. The solid lines represent the mean difference between methods (preferred – alternate). The long-dashed lines represent the 95% confidence limits of the mean differences (first and third quartiles for non-parametric data). The short-dashed lines represent the mean differences ± 2 SD, the reproducibility limits (comparability) of the 2 methods.
Comparison of the Preferred and Alternate Calculation Methods for RV and TLC
For the whole group, no significant differences in mean values between the preferred and alternate calculation methods were seen for RV or TLC (P = .35 and P = .42, respectively, using data from the preferred measurement, and P = .39 and P = .35, respectively, using data from the alternate measurement).
Discussion
This study found small (< 150 mL) but statistically significant differences in the means for plethysmographic measurements of VC and TLC in the normal group, and RV and TLC in the restricted group, using the preferred and alternate methods described in the ATS/ERS Standardization of Static Lung Volumes document.4 However, in subjects with air-flow obstruction, no differences in the means were seen. Eleven percent of subjects tested changed ventilatory classification group between test methods, suggesting clinically relevant differences between the preferred and alternate methods may exist, though only 3 subjects had differences in parameters that exceeded reproducibility between the methods. In addition, this study has shown that the differing calculation methods used by the alternate and preferred methods are unnecessary: identical results were obtained when data collected was analyzed with respect to both calculation methods as set out by the ATS/ERS.4
This study supports the ATS/ERS definition of the preferred method of measuring plethysmographic lung volumes as being an ERV maneuver followed by an inspiratory VC after FRC measurement to calculate RV and TLC.4 However, the reason for this is due to the possibility that IC and TLC may be underestimated using the alternate method in some individuals, rather than the hypothesis of the ATS/ERS task force that RV may be elevated in those with substantial obstruction when using the alternate method.4
The ATS/ERS task force hypothesizes that RV is likely to be elevated in individuals with air-flow obstruction, using the alternate method. The current study was unable to show significant differences in mean RV between test methodologies in obstruction, even in those with gas trapping due to air-flow obstruction. Further, no relationship between the FEV1 z-score (an indicator of severity) in those with obstruction and the absolute difference in RV between the preferred and alternate methods was found (r2 = 0.0004).
In those subjects whose ventilatory function changed classification between methodologies, two thirds moved from a restrictive type pattern using the alternate method to a normal or obstructive pattern using the preferred method. A smaller TLC was achieved using the alternate method, compared to the preferred method, without a concomitant change in RV. It appears that, for some individuals, it may be more difficult to take a complete IC breath to TLC following FRC measurement, as happens using the alternate method, compared to exhaling completely to RV following FRC measurement via the preferred method. This may happen due to poor subject coordination or perhaps because the respiratory muscles are in a less advantageous position at FRC, compared to RV, for completing a maximal inhalation.
It should be noted that classification of ventilatory function is dependent on the choice of reference values and normal limits. Hence, using changes in classification to determine comparability of methods should be undertaken with caution. It is perhaps more useful to look at those individuals who change ventilatory classification between methods and have parameters where the difference between the methods exceeds the reproducibility of the methods. In this study only 3 subjects met these criteria.
Comparisons to Other Data
A study directly comparing the preferred and alternate methods of measuring static lung volumes in a body plethysmograph using linked maneuvers could not be found in the literature. However, a 1989 publication2 exploring differences in mean FRC, RV, and TLC between the preferred and alternate methods using plethysmography, performed the alternate method as linked FRC and spirometry maneuvers, and the preferred method as unlinked FRC and spirometry maneuvers. While the methods of the study were not consistent with the current study, the group did find small, statistically significant differences of the means for RV and TLC between methods. Williams and Bencowitz did not consider the differences to be clinically relevant, as only 2% of the studied population changed classification between methods. This is in contrast to this study's finding of 11% changing classification, but may be explained by differences in the within subject coefficient of variation for RV and TLC between studies (this study 4.5% and 1.9%, respectively, vs the earlier study 11% and 4%, respectively). That is, the tighter coefficient of variation leads to an increase in the accuracy with which ventilatory function can be classified.
Similarly, only one paper exploring different methods of calculating TLC could be found.3 Data were collected using the alternate method, and 4 methods of calculating TLC were compared: method 1: mean FRC + largest IC; method 2: mean FRC + mean IC (using ICs not > 5% different from largest IC); method 3: largest sum of individual, linked FRC and IC volumes; and method 4: the average of sums from method 3 (using sums that did not differ from largest by > 5%). While this group found significant differences between methods (calculated via paired t tests), the mean differences were small (< 3%). Using our data and analysis of variance, no differences in the means were found between the 4 calculation methods described by Bohadana et al (P = .99) for TLC or RV.3 RV was calculated using FRC and ERV values substituted into methods described earlier in this paragraph. Similarly, calculating TLC and RV using the alternate and preferred methods of the ATS/ERS4 resulted in no significant differences of the means. This suggests that the differing methods for calculating TLC and RV, depending on whether the alternate or preferred methods are performed, are unnecessary.
Finally, there are 2 possible limitations of this study. First, the small numbers of subjects recruited, compared to the overall clinical population tested over the study period, may limit the generalizability of the results. The study group and the overall clinical population were found to be similar following classification according to ventilatory pattern with respect to FEV1/FVC, TLC, and RV/TLC, except for RV/TLC in the “all obstruction” group. This is explained by a higher proportion of subjects with gas trapping in the clinical population (71%), compared to the study population (61%). When comparisons were made between the study population and clinical population for those with obstruction without gas trapping, no difference in RV/TLC was found. Hence, this study's findings should be generalizable to a clinical population. Second, the number of scientists participating in data collection and their preference for a particular test method may have introduced bias to the results. The study was not limited to a select number of scientists, so that the study would reflect the clinical practice of the laboratory. All scientists were expected to test to ATS/ERS criteria for each method for each subject, and only data meeting ATS/ERS criteria were analyzed. Where differences of the means were seen between methods, the upper confidence limit of the mean difference was small (≤ 0.19 L), and the clinical relevance of this is likely to be small. Hence, scientist bias affecting the study results is unlikely.
Conclusions
In summary, although significant differences between the means were seen for the normal and restrictive ventilatory function subgroups (VC and TLC, and RV and TLC, respectively), no differences were seen between methods for obstruction as was hypothesized by the ATS/ERS Task Force.4 The significant differences that were seen were small, and their clinical importance overall is unclear. A subgroup of individuals did change classification between test methods, with the alternate method predominantly delivering a lower TLC, in comparison to the preferred method, without a change in RV. This study supports the ATS/ERS static lung volume measurement guidelines that consider the preferred method of testing to be an ERV maneuver followed by an inspiratory VC after FRC measurement to calculate RV and TLC. The 2 ATS/ERS recommended calculation methods for RV and TLC delivered identical results, implying that different calculation methods, based on the measurement method used, are unnecessary.
Footnotes
- Correspondence: Brigitte M Borg CRFS, Department of Allergy, Immunology, and Respiratory Medicine, The Alfred Hospital, 55 Commercial Road, Melbourne, Victoria 3004 Australia. E-mail: b.borg{at}alfred.org.au.
The authors have disclosed no conflicts of interest.
Ms Borg presented a version of this paper at the meeting of the Australia and New Zealand Society of Respiratory Sciences, held April 3–6, 2009, in Darwin, Australia, and at the International Congress of the American Thoracic Society, held May 15–20, 2009, in San Diego, California.
See the Related Editorial on Page 1199
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}