

Abstract
OBJECTIVE: To compare the influence of 2 ventilation strategies on the occurrence of central apneas.
METHODS: This was a prospective, comparative, crossover study with 14 unsedated subjects undergoing weaning from mechanical ventilation in the medical ICU of Hôpital du Sacré-Cœur, Montréal, Québec, Canada. The subjects were ventilated alternately in neurally adjusted ventilatory assist (NAVA) and pressure support ventilation (PSV) modes. Inspiratory flow/time and pressure/time waveforms and diaphragmatic electrical activity were used to detect central apneas. Ventilatory variability and breathing pattern were evaluated in both modes. Breathing patterns just before central apneas, and associations between apneas and sleep patterns (electroencephalogram) were studied.
RESULTS: Switching from PSV to NAVA did not change mean minute ventilation, tidal volume, or breathing frequency. However, tidal volume variability, defined as the coefficient of variability (standard error/mean), was significantly greater with NAVA than with PSV (17.2 ± 8 vs 10.3 ± 4, P = .045). NAVA induced a greater decrease in central apneas, compared to PSV (to 0 with NAVA vs 10.5 ± 11 with PSV, P = .005). Central apneas during PSV were detected only during non-rapid-eye-movement sleep.
CONCLUSIONS: NAVA was associated with increased ventilatory variability, compared to constant-level PSV. With NAVA the absence of over-assistance during sleep coincided with absence of central apneas, suggesting that load capacity and/or neuromechanical coupling were improved by NAVA and that this improvement decreased or abolished central apneas.
- mechanical ventilation
- central apnea
- ventilation mode
- neurally adjusted ventilatory assist
- pressure support
- sleep patterns
Introduction
Pressure support ventilation (PSV) is widely used, most notably during weaning off mechanical ventilation, but may be associated with central apneas and intermittent breathing.1 During sleep in PSV mode, inspiratory efforts are constant but tidal volume (VT) oscillates, intermittently decreasing the PaCO2 level below the apneic threshold, which is not very different from the PaCO2 value in eupnea.2 The apneic PaCO2 threshold is physiologically lower during stage 1 sleep than during wakefulness.2,3 Studies show that patients who shift repeatedly between sleep stages exhibit increased sensitivity to central apneas.2,3 Central apneas are associated with arousals related to the increase in respiratory effort often seen after apneas.4,5 Severe sleep disruption has been reported in patients with Cheyne-Stokes respiration. The sleep disruption was due to repeated arousals during the hyperpneic phase of Cheyne-Stokes respiration, which accounted for two thirds of all arousals.6,7 In theory, arousals are responsible for a sympathetic response manifesting as tachycardia, hypertension, and increased myocardial oxygen consumption.8 In mechanically ventilated patients, additional factors that may induce arousals include the audio alarm triggered by low minute ventilation (V̇E) and initiation of the apnea backup mode. All these factors must be considered when choosing ventilation settings.
Excessive pressure support during sleep may increase the likelihood of periodic breathing, although CO2 sensitivity is not modified, since V̇E increases in response to PaCO2 elevation.9 However, it does not appear possible to determine the difference between the actual PaCO2 and the PaCO2 apneic threshold (fraction of expired CO2 – PaCO2) in individual patients receiving mechanical ventilation, without performing individual titration through trial and error.
To improve the match between the patient's needs and the assistance delivered by the ventilator, manufacturers have developed several new modes of mechanical ventilation,10 including proportional assist ventilation and neurally adjusted ventilatory assist (NAVA). NAVA is an assist mode that delivers a pressure proportional to the integral of the electrical activity of the diaphragm (EAdi).11 Therefore, the pressure level is determined by the neural output of the patient's central respiratory command, which would be expected to prevent over-assistance.12–15 Moreover, recent studies suggest that NAVA may allow a high level of breathing pattern variability.16–17 Avoiding over-assistance and delivering proportional assistance would be expected to limit apneas, although ventilation varies less during the night than during the day.
The objective of the prospective study reported here was to compare the effects of NAVA and PSV on the occurrence of central apneas during weaning.
QUICK LOOK
Current knowledge
During weaning from mechanical ventilation, excessive pressure during pressure support ventilation is associated with intermittent apnea, because PaCO2 is driven below the apneic threshold. During sleep this intermittent breathing pattern is associated with fragmented sleep.
What this paper contributes to our knowledge
The use of neurally adjusted ventilatory assist (NAVA) ventilation reduces the incidence of central apneas and increases the variability in tidal volume, compared to excessive pressure with pressure support ventilation. For the mean minute ventilation and respiratory rate, there was no difference between the 2 techniques.
Methods
The ethics committee of Hôpital du Sacré-Cœur, Montréal, Québec, Canada, approved the study, and subjects or their surrogates gave their informed consent.
Study Population
This study was performed in the same population as a previous study from our group on NAVA and sleep.18 We conducted a prospective, interventional, crossover study in a 22-bed medical ICU at Hôpital du Sacré-Cœur over a 12-month period. Inclusion criteria were invasive mechanical ventilation, normal consciousness, absence of sedatives and opiates for ≥ 24 h, and PSV with an FIO2 below 0.60 and a PEEP of 5 cm H2O to achieve an SpO2 of at least 90%. Exclusion criteria were presence of a central nervous system disorder, Glasgow Coma Scale score < 11, hemodynamic instability, renal and/or hepatic insufficiency, ongoing sepsis, history of esophageal varices or gastroesophageal bleeding in the past 30 days, and history of gastrointestinal symptoms such as vomiting.
Ventilation Methods
All subjects were ventilated through an endotracheal or tracheostomy tube. Subjects meeting the inclusion criteria were connected to a ventilator capable of delivering both PSV and NAVA (Servo-i, Maquet Critical Care, Sölna, Sweden). As previously described,19 EAdi was recorded using a 16 French gastric catheter equipped with electrodes (EAdi catheter, Maquet Critical Care, Sölna, Sweden), whose correct position was checked using the “EAdi catheter positioning” ventilator function. Humidification was provided by a heat and moisture exchanger in all subjects. End-tidal CO2 (PETCO2) was monitored with the Servo-i volumetric CO2 module.
PSV and NAVA were delivered in random order, determined using a closed-envelope technique. Each mode was delivered for 4 periods of 4 hours: 2 during the day (7:00 to 11:00 am and 12:00 to 4:00 pm) and 2 at night (10:00 pm to 2:00 am and 3:00 to 7:00 am). To prevent possible data contamination from the previous mode of ventilation, data acquisition was delayed for 1 hour after each ventilator setting change (Fig. 1).

Study protocol. Each recording lasted 4 hours, and 4 recordings were obtained with each subject, for a total of 24 consecutive hours. PSV = pressure support ventilation. NAVA = neurally adjusted ventilatory assist.
Inspiratory pressure support was titrated to obtain a VT of 8 mL/kg of predicted body weight during active inspiration, without exceeding 20 cm H2O of pressure support and a breathing frequency of < 35 breaths/min. Flow-trigger sensitivity was set as low as possible (1–2 L/min) without inducing auto-triggering; cycling-off occurred when the inspiratory flow fell below 25% of the peak inspiratory flow. During PSV the ventilator function “NAVA Preview” was used to estimate the NAVA level required to achieve the same peak inspiratory pressure. After switching to NAVA, the settings were gradually adjusted to deliver the same assist level (peak pressure) and external PEEP as used previously with PSV. With NAVA the EAdi inspiratory trigger was at the lowest setting (0.5 μV). EAdi was recorded with both ventilation modes and used to evaluate patient-ventilator synchrony.
The backup apnea ventilation delay was set at 15 seconds, so that apneas lasting 10 seconds or more could be identified and their impact on sleep architecture (arousals) assessed.
Sleep Patterns
The electroencephalogram was recorded using standard electrode positions (left frontal/right auricular reference [F3/A2], right frontal/left auricular reference [F4-A1], left central/right auricular reference [C3/A2], right central/left auricular reference [C4/A1], left occipital/right auricular reference [O1/A2], and right occipital/left auricular reference [O2/A1] in the international 10–20 system for electrode placement).20 The standard reference was the left mastoid lead.20 Two electrooculogram and 3 chin electromyogram leads were used to score rapid-eye-movement (REM) and non-REM sleep. The electroencephalogram, right and left electrooculograms, and submental electromyogram signals were amplified and recorded in the data acquisition system (Alice 5 polysomnography system using Alice Sleepware 2.5 software, Respironics, Murrysville, Pennsylvania).
Sleep recordings were scored manually by a pulmonologist who was blinded to the study data and used Rechtschaffen and Kales criteria for sleep stages,21 and American Sleep Disorder Association criteria for arousals and awakenings.22,23 Central apneas were diagnosed according to international recommendations,23 as absence of breathing and respiratory effort for at least 10 seconds (Fig. 2). Arousals and awakening were classified as apnea-related if they occurred within 3 breaths and/or 15 seconds of the end of an apnea.24,25
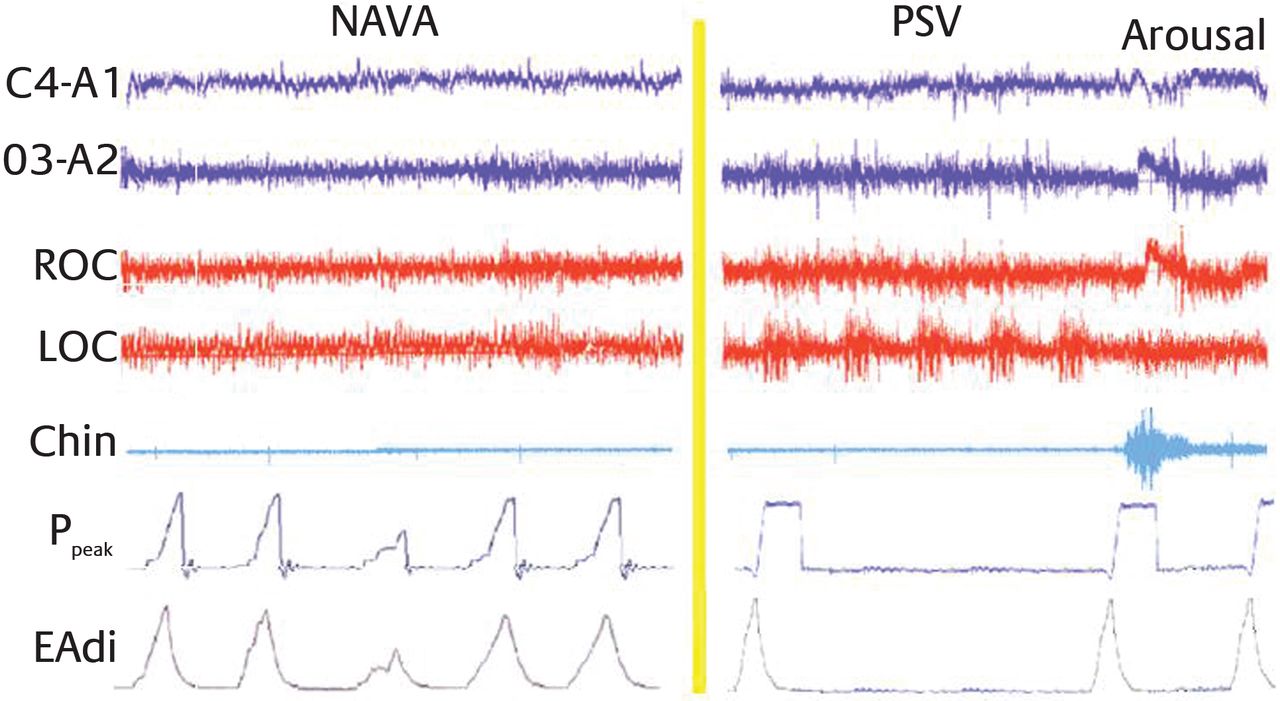
Polysomnography tracings with neurally adjusted ventilatory assist (NAVA) and pressure support ventilation (PSV) in a representative subject. C4-A1 and O3-A2 are the electroencephalogram readings. ROC and LOC are the electrooculogram readings. Chin is the electromyogram reading. Ppeak is the peak airway pressure. EAdi is the electrical activity of the diaphragm reading.
Data Acquisition and Analysis
Flow and pressure signals were acquired at a sampling rate of 100 Hz. Signals from each electrode pair were differentially amplified, digitized, and processed online, using previously described filters and algorithms.26–28 Changes in diaphragm position along the array were accounted for using the cross-correlation technique,29,30 and diaphragm-to-electrode distance filtering was minimized using the double-subtraction technique.31 The root mean square was calculated for the subtracted signal and the signal obtained from the electrode pair on the diaphragm, and these values were summed every 16 ms to quantify EAdi. Signal segments with residual disturbances due to cardiac electric activity or common mode signals were identified using specific detectors and replaced by the previously accepted value. This processed EAdi signal was used to control the ventilator during NAVA and was simultaneously acquired at a sampling rate of 2,000 Hz.
EAdi was obtained from the ventilator through an RS232 interface, at a sampling rate of 100 Hz, and recorded using dedicated software (Nava Tracker 2.0, Maquet Critical Care, Sölna, Sweden). The input was analyzed using software (Analysis 1.0, Maquet Critical Care, Sölna, Sweden, and a customized version of Excel, Microsoft, Redmond, Washington).
The peak of rectified and integrated EAdi swings (peak EAdi) was measured. From the flow signal we obtained the ventilator frequency (f-flow), flow-based inspiratory time, and flow-based expiratory time. To evaluate breathing pattern variability during the different sleep stages with each mode, we calculated the coefficient of variability (defined as the standard error/mean ratio × 100) for VT, breathing frequency, and peak EAdi.32,33
Statistics
The statistical analysis was performed using statistical software (SPSS 17.0, SPSS, Chicago, Illinois). Continuous variables are described as mean ± SD. Data were compared using the general linear model for repeated measures. Given the small sample size, a nonparametric test was used to compare variables; we chose the Wilcoxon test for paired samples. Two-tailed P values smaller than .05 were considered significant. Variability data were compared using analysis of variance for repeated measures.
Results
Study Population
We included 14 subjects, whose main characteristics at admission are reported in Table 1. Mechanical ventilation was required for acute respiratory failure in 10 subjects, postoperative cardiac complications in 3 subjects, and septic shock in 1 subject. Mean PSV level was 15 ± 5 cm H2O, and mean NAVA level was 1.6 ± 1.4 cm H2O/μV. PEEP was kept at 5 cm H2O in all subjects with both ventilation modes.
Subjects
Breathing Pattern
Mean total sleep time was 537 ± 193 min. Mean sleep efficiency (the percentage of sleep during the study) was 56 ± 20%. Table 2 reports the main breathing pattern data. Mean V̇E did not differ significantly between PSV and NAVA: 9.6 ± 1.8 L/min and 9.3 ± 1.8 L/min, respectively (P = .51). Mean breathing frequency was 17 ± 4.6 breaths/min with PSV, and 18 ± 5.7 breaths/min with NAVA (P = .14). The mean V̇E, VT, and breathing frequency did not differ significantly between the 2 ventilation modes. PETCO2 was not significantly different between the 2 modes during any of the sleep stages.
VT, Breathing Frequency, Apneas per Hour, and PETCO2 While Awake and Asleep
VT differed significantly between the 2 ventilation modes during sleep stage 3–4 (mean 391 ± 57 mL with NAVA and 435 ± 64 mL with PSV, P = .005) and during REM sleep (mean 360 ± 54 mL with NAVA and 415 ± 61 mL with PSV, P = .008, see Table 2). During PSV, VT did not vary significantly between wakefulness (429 ± 65 mL) and REM sleep (415 ± 61 mL) (P = .08). However, with NAVA, VT was significantly greater during wakefulness (419 ± 63 mL) than during REM sleep (360 ± 54 mL) (P = .001). VT differed significantly between stage 1 and REM sleep with both modes (NAVA 431 ± 69 mL vs 360 ± 54 mL, respectively, P = .001, PSV 442 ± 61 mL vs 415 ± 61 mL, respectively, P = .001, see Table 2).
Mean breathing frequency during non-REM sleep did not differ significantly between the 2 ventilation modes. During REM sleep, in contrast, mean breathing frequency was significantly higher with NAVA than with PSV (15 ± 3 breaths/min and 13 ± 2 breaths/min, respectively, P = .004). During wakefulness the mean breathing frequency was also significantly higher with NAVA (20 ± 4 breaths/min and 18 ± 3 breaths/min, respectively, P = .005, see Table 2).
Table 3 shows the oscillatory behavior of VT, breathing frequency, V̇E, and PETCO2 during sleep stages 2 and 3–4 with PSV.
Oscillatory Behavior of VT, Breathing Frequency, V̇E, and PETCO2 During Sleep Stages 2 and 3–4 During PSV in the 10 Patients With Central Apneas
Apneas
Sleep apnea occurred in 10 subjects, all of whom had either COPD or chronic heart failure, 2 known risk factors for central apneas. Moreover, these subjects experienced hyperventilation during sleep, which preceded the central apneas. Table 3 reports the mean number of sleep apneas per hour of sleep in the 10 subjects with sleep apnea. The mean sleep apnea index (number of apneas per hour of sleep) was 10.5 ± 11 during PSV and 0 during NAVA (P = .005). During PSV, central apneas occurred only during non-REM sleep. All central apneas were associated with micro-arousals. During the second preceding the detection of central apneas, VT and V̇E increased suddenly, while breathing frequency and PETCO2 decreased (see Table 3).
Variability of Ventilation
Table 4 reports the coefficient of variability values for VT, f-flow, and peak EAdi. VT variability was greater with NAVA during all sleep stages, indicating increased breath-to-breath variability, compared to PSV. In PSV mode, VT variability differed significantly between stage 1 and stage 3–4 sleep, but not between stage 1 and REM sleep (P = .14). VT variability during stage 2 and stage 3–4 sleep in PSV mode differed significantly from that in REM sleep (P = .01 and P = .001, respectively) (Fig. 3). With NAVA, VT variability was stable, with no significant differences across sleep stages (Fig. 4). Tidal volume variability was significantly greater with NAVA than with PSV (17.2 ± 8 vs 10.3 ± 4, P = .045).
VT, f-flow, and EAdi Peak Variability in the 10 Patients With Central Apneas
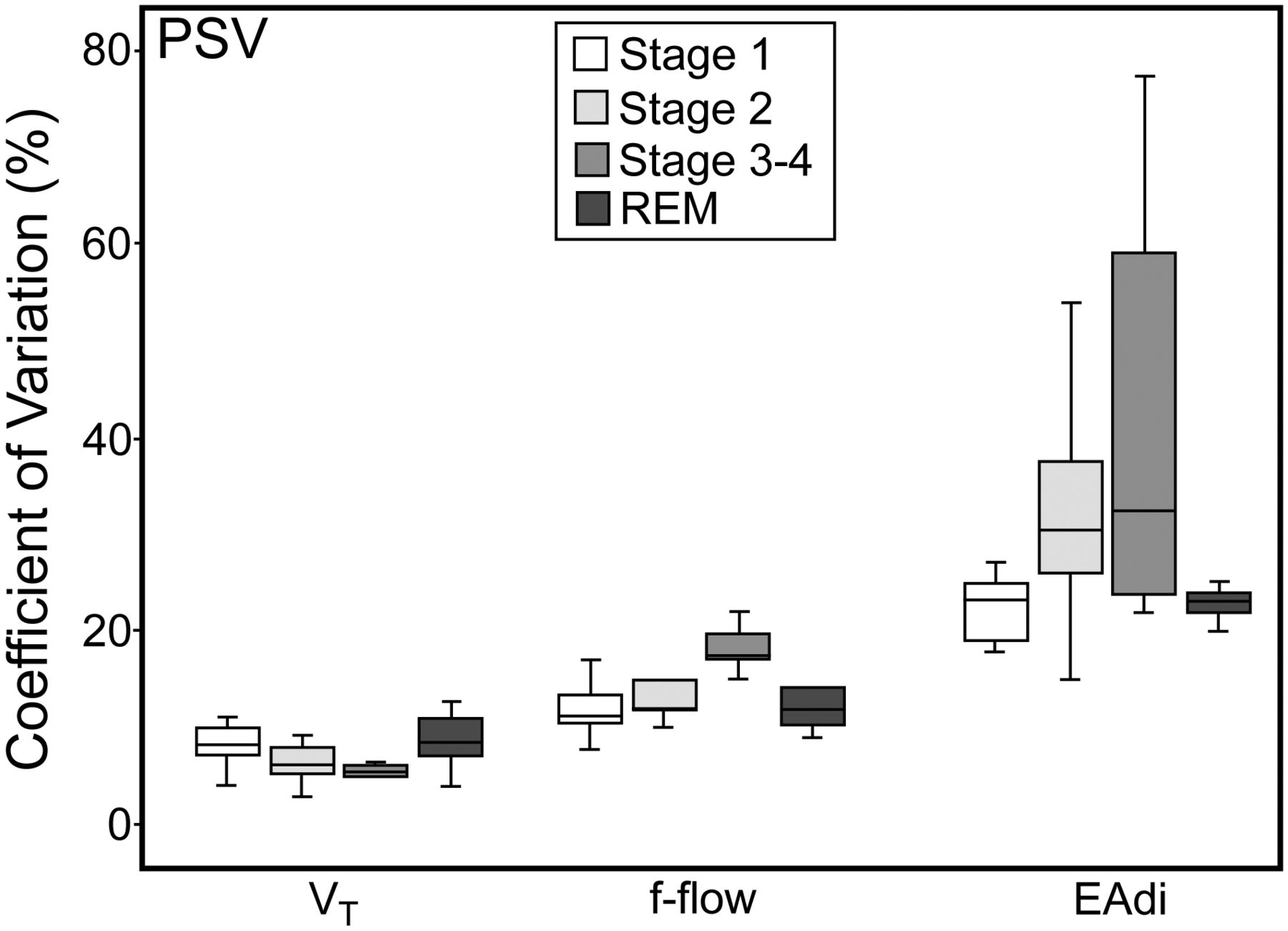
Variability during pressure support ventilation (PSV). VT = tidal volume. f-flow = flow-based breathing frequency. EAdi = electrical activity of the diaphragm.

Variability during neurally adjusted ventilatory assist (NAVA). VT = tidal volume. f-flow = flow-based breathing frequency. EAdi = electrical activity of the diaphragm.
With PSV, f-flow variability differed significantly between sleep stages 1 and 3–4 (P = .01), 2 and 3–4 (P = .005), and 3–4 and REM (P = .001) (see Fig. 3). With NAVA, f-flow variability showed no significant differences across sleep stages (see Fig. 4).
With PSV, peak EAdi variability differed significantly between sleep stages 1 and 2 (P = .005), 1 and 3–4 (P = .003), 2 and REM (P = .038), and 3–4 and REM (P = .002) (see Fig. 3). With NAVA, peak EAdi variability did not vary significantly across sleep stages (see Fig. 4).
Discussion
In this study of unsedated subjects responding to simple orders when awake and receiving assisted mechanical ventilation during the weaning process, the occurrence of central apneas was influenced by the ventilatory mode. Sleep disruption is common in critically ill patients and may influence the clinical course of the acute illness.8,34,35 Even if it is well documented that sleep abnormalities may impair psychological and physiological well-being, with effects such as increased protein catabolism, decreased immune function, and altered respiratory mechanics, which could affect weaning from mechanical ventilation,36 the impact of sleep disturbances on morbidity and mortality remains unknown37; however, it could worsen the quality of life after discharge.38,39
Quantitative and qualitative deficiencies have been characterized, including decreased total sleep time, fragmented sleep, as well as altered circadian patterns. The etiology of sleep disruption in the ICU is multifactorial, including the inherent nature of environment (exposure to noise and light), medications, mechanical ventilation, and particularly, patient-ventilator interaction and acute illness. PSV is associated with central apneas in both healthy individuals1 and mechanically ventilated patients,40 and the ventilator settings influence the degree of sleep disruption,41 suggesting that patient-ventilator asynchrony may contribute to sleep disruption.42 Studies have established that decreasing patient-ventilator asynchrony results in less sleep disruption and in greater sleep efficiency.43,44 Proportional assist ventilation and NAVA were developed to better match the level of assistance delivered by the ventilator to the needs of the individual patient, thereby minimizing patient-ventilator asynchrony.10
NAVA is an assist mode in which the ventilator is triggered, even during expiration with intrinsic PEEP, and cycled off based on the EAdi value, which directly reflects the activity of the patient's neural respiratory command.11 The inspiratory airway pressure applied by the ventilator is determined as follows:
In a recent comparison of the impact of NAVA and PSV on sleep architecture, we demonstrated that NAVA provided better sleep quality in terms of REM sleep, fragmentation index, and ineffective efforts in unsedated adults.18 NAVA also allows considerable variability in the breathing pattern (ie, better replicates the variability of spontaneous breathing). We hypothesized that this greater variability, compared to PSV, decreased central apneas. To our knowledge, this hypothesis has not been evaluated previously. The greater ventilatory variability with NAVA is related to increased flow complexity, with no change in EAdi complexity, compared to PSV.16 The better coupling between mechanical assistance and neural output achieved with NAVA may result in better translation of the complexity of the central ventilatory command into a complex flow pattern. NAVA prevents over-assistance, thereby avoiding episodes of hyperventilation leading to central apneas.
In a polysomnography study of 11 critically ill patients, sleep fragmentation was less marked with continuous mandatory ventilation than with PSV, because PSV was associated with over-assistance-induced central apneas.40 Over-assistance was reflected by higher VT values during PSV than during continuous mandatory ventilation. Adding a mechanical dead space significantly decreased the number of central apneas: a finding that further supported over-assistance as the cause of central apneas.40,50
A study comparing PSV and the SmartCare automated weaning system in conscious unsedated patients showed similar numbers of central apneas.51 SmartCare is an embedded version of the closed-loop NeoGanesh system,52,53 which keeps the patient within the comfort zone (as defined by respiratory parameters) while gradually decreasing the level of pressure support to a minimal value, at which point a trial of spontaneous breathing is performed. SmartCare would be expected to prevent over-assistance by adjusting the level of support. The absence of a difference in central apnea occurrence between PSV and SmartCare may be ascribable to the large proportion in this study51 of patients with chronic heart failure, a risk factor for central apneas. In our subjects also, central apneas occurred chiefly during non-REM sleep, possibly as a result of sequential over-assistance (VT overshoot), which is seen with PSV but not with NAVA. The mechanisms underlying central apneas may be too complex to be prevented by closed-loop mechanical ventilation. Proportional ventilation seems crucial to preventing central apneas. However, the concept underlying SmartCare is interesting, and studies comparing NAVA and SmartCare are needed. In our study the ventilatory behavior preceding central apneas with PSV was similar to that described in a previous study.3 Another finding shared by both studies is the increase in VT and V̇E immediately before central apneas, together with a PETCO2 to the apneic threshold.3
A few methodological points deserve discussion. We obtained 4-hour long recordings on 4 different occasions in each subject. Each subject was studied for 24 consecutive hours. This method was chosen to minimize instabilities or complications, and to avoid delays in extubation. Cessation of sedatives for more than 24 hours does not rule out residual sedation. However, all subjects had Ramsay scores no greater than 2 and Glasgow Coma Scale scores of 11 or more at the time of recording.51 Subjects with risk factors for central apnea (chronic heart failure or COPD) had more numerous central apneas during non-REM sleep, suggesting lower apnea PaCO2 thresholds for central apnea.
Increased diaphragmatic activity during non-REM sleep is associated with an increase in VT.54 In our study, subjects receiving PSV exhibited increased peak EAdi variability during non-REM sleep and a concomitant VT increase, with little VT variability. This pattern increases the risk of central apnea, especially as the apneic threshold is lower in REM sleep than in non-REM sleep.55
A study in healthy volunteers showed suppression of tonic diaphragmatic activity, with preservation of phasic activity during REM sleep.56 Transition inhibition of the intercostal muscles is abolished and phasic activity of the intercostal, abdominal, and sternocleidomastoid muscles is greatly reduced.56,57 The contribution of rib cage motion to VT is moderate during REM sleep, and as a result, VT decreases significantly with NAVA, but not with PSV. Moreover VT variability is higher, which may protect against central apnea.
Limitations of our study should be acknowledged. First, this work was performed in a single center with researcher experience on NAVA, and included only 14 subjects. Therefore, these results may not pertain to other ICUs and to all subjects. Second, sedation was stopped only 24 hours before beginning the study, so we could not exclude that there was an effect of sedation. However, all subjects included experienced NAVA and PSV alternately. Third, a single NAVA level and PSV were used, but we could not be certain that the results were the same with another level. Nevertheless our study demonstrated a physiological effect of NAVA, which must be confirmed by further clinical studies.
Conclusions
To our knowledge, this study provides the first comparative data on the occurrence of central apneas with PSV and NAVA in unsedated, ventilated, critically ill subjects. At a constant ventilation level, NAVA was associated with greater ventilatory variability than PSV. With PSV, over-assistance (VT overshoot) occurred in sleep stages 2 and 3–4. Central apneas occurred only with PSV. The absence of central apneas with NAVA was probably ascribable to improvements in neuromechanical coupling, which avoided the delivery of excessive assistance. The protective effect of NAVA against central apneas occurred even in patients with risk factors (chronic heart failure or COPD). Our data support the use of NAVA in novel ventilation strategies, particularly in patients at risk for central apnea. However, further clinical investigations are needed to evaluate the impact of NAVA on weaning time and patient outcomes.
Acknowledgment
We are grateful to Hélène Prigent MD, Physiology and Functional Testing Department, Raymond Poincaré Teaching Hospital, Garches, France, for her help in editing the manuscript.
Footnotes
- Correspondence: Stephane Delisle RRT MSc PhD FCSRT, Service des Soins Intensifs, Hôpital du Sacré-Cœur de Montréal, 5400 Boulevard Gouin Ouest, Montréal, Québec H4J 1C5 Canada. E-mail: sdelisle{at}hotmail.com.
Dr Delisle has disclosed a relationship with Fisher & Paykel. The other authors have disclosed no conflicts of interest.
See the Related Editorial on Page 884
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}