

Abstract
BACKGROUND: Respiratory therapist (RT)-driven protocols have been in use for over 30 years. Protocols have been reported to decrease unnecessary or harmful therapy, health-care costs, and hospital stay. This study represents the evaluation of an original respiratory care protocol in the pediatric ICU at Arkansas Children's Hospital for β-agonist and airway clearance interventions where one did not exist.
METHODS: This project was composed of 2 parts: a survey administered to RTs and licensed independent practitioners and a retrospective review of outcome data comparing a therapist-driven β-agonist/airway clearance protocol with physician-directed respiratory care ordering in a patient population admitted for acute respiratory failure.
RESULTS: Acceptance of the protocol was evident in the survey responses because overall perceptions surrounding the implementation of the β-agonist/airway clearance protocol were positive, and responders perceived that the protocol implementation elevated the status and increased the value of respiratory therapists. For the comparison of physician-directed orders with therapist-driven protocols, there were no significant differences between pre- and post-intervention groups for mean age, sex, mean daily acuity, or mean weighted daily acuity (P = .33, .19, >.99, and .79, respectively). There were also no differences in pediatric index of mortality 2, pediatric index of mortality 2 rate of mortality, pediatric risk of mortality 3 probability of death, and pediatric risk of mortality 3 scores (P = .63, .56, .19, and .44, respectively) between the 2 groups. When comparing physician-directed orders to therapist-driven protocols, all outcome measures (length of stay, β-agonist therapies, airway clearance therapies, and ventilator days) showed statistically and clinically important reductions, adjusting for subject characteristics (P < .001) for the therapist-driven protocol group.
CONCLUSIONS: In this institution, implementation of a β-agonist/airway clearance protocol resulted in significant reductions of subject interventions and improved outcomes by decreasing length of stay and ventilator days as well as contributing information where clinical evidence is scant, specifically the pediatric ICU.
Introduction
Respiratory care protocol development and utilization were first described in 1981.1 This innovative approach to respiratory care included patient evaluation, appropriate therapy selection and administration, timely patient reassessment, and alteration of therapy frequency based on the patient's respiratory status. It also provided the impetus for expansion of protocol-directed interventions into many facets of respiratory care. Since that time, numerous authors have added to this body of knowledge and reported extensively on protocol use. Protocols have been reported to decrease unnecessary or harmful therapy, health-care costs, and hospital length of stay while improving resource utilization, effectiveness and appropriateness of care, consistency of care, and patient outcomes, thereby improving the overall quality of patient care.2–8 Protocols involving numerous interventions, including oxygen titration, therapeutic interventions, and ventilator weaning, have been described and reported in the literature.9–13 These studies range from retrospective reviews to randomized controlled trials.
The Respiratory Care Department at Arkansas Children's Hospital has extensively utilized protocols in the medical and surgical units since 1994; however, they were not considered for implementation in the ICUs. The primary barrier was resistance from the medical staff and the prevailing attitude that, as a teaching institution, it was important that fellows and residents were given the opportunity to learn how to administer appropriate respiratory care orders and interventions. Ultimately, with the support of the Respiratory Care Services Medical Director and Critical Care Medicine Director, a plan was formulated to initiate a respiratory care protocol in the pediatric ICU (PICU) at the Arkansas Children's Hospital. This paper reviews the implementation and initial outcomes of a respiratory therapist (RT)-driven β-agonist/airway clearance protocol in the PICU.
QUICK LOOK
Current knowledge
Respiratory therapist-driven protocols have become a standard of care in many health-care institutions throughout the country. Evidence has shown that therapist-driven protocols provide for effective and efficient allocation of respiratory care interventions. Therapist-driven protocols have been shown to improve the overall quality of patient care when properly implemented.
What this paper contributes to our knowledge
This paper summarizes the implementation of a therapist-driven protocol in a pediatric ICU. Survey tools were used to quantify the perceptions of health-care personnel regarding the initiation of the protocol. Outcome data were analyzed and revealed reductions in respiratory care interventions, ventilator days, and length of stay after the implementation of the protocol in this pediatric population.
Methods
This project was reviewed by the University of Arkansas for Medical Sciences institutional review board, which determined it was not human subject research. This study was composed of 2 parts: a survey administered to RTs and licensed independent practitioners and a retrospective review of outcome data comparing a therapist-driven β-agonist/airway clearance protocol with physician-directed respiratory care ordering. The β-agonist/airway clearance protocol was implemented in August 2013.
In the initial phase of this project, 2 survey tools were developed and administered via SurveyMonkey. One was e-mailed to RTs, consisted of 23 statements, and was sent to 46 potential responders. The other was e-mailed to licensed independent practitioners, which included physicians, fellows, and advanced practice nurses; consisted of 17 statements; and was sent to 25 potential responders. Respondents were assured that responses were confidential and implied consent by participation and completion of the survey. The investigators were blinded to individual responses. The initial e-mail notification occurred 6 weeks after β-agonist/airway clearance protocol implementation. Two subsequent e-mail notifications occurred at 2 and 4 weeks after the initial notification. The surveys differed for RTs and licensed independent practitioners but contained 12 identical statements (Table 1). A 4-point Likert scale was used to quantify the responses and included the following options: totally disagree, somewhat disagree, somewhat agree, and totally agree. The 4-point Likert scale was used to eliminate neutral responses and encouraged respondents to either positively or negatively evaluate their perceptions of the survey statements. Results were aggregated into 2 groups, totally agree and somewhat agree versus totally disagree and somewhat disagree, and presented as percentages.
Statements Common to Both Survey Tools Administered to Respiratory Therapists and Licensed Independent Practitioners
In the secondary phase, this study utilized a retrospective pre/post-intervention design. The target population included pediatric subjects admitted to the PICU with acute respiratory failure (ICD-9 codes 518.81, 518.51, 518.84, and 518.53). The β-agonist/airway clearance protocol was composed of a detailed clinical assessment resulting in a score (Table 2). The resulting score was used to initiate therapy frequency (Table 3). A higher score resulted in more frequent interventions. Subjects were reevaluated every 24 h. Based on the reevaluation score obtained, the subject's frequency of therapy increased, decreased, or stayed the same based on objective data obtained during the clinical assessment. This process continued for the duration of the subject's PICU stay or until therapy was discontinued (Fig. 1).
Scoring Tool Used With the β-Agonist/Airway Clearance Protocol
Therapy Frequency Based on β-Agonist/Airway Clearance Protocol Score

Intervention flow diagram for the β-agonist/airway clearance protocol (BA/ACP).
Data were collected for one 6-month time period from October 2012 to March 2013 (Group 1; n = 152) and represented physician-directed respiratory care orders. These data were compared with one 6-month time period from October 2013 to March 2014 (Group 2; n = 171) and represented the therapist-driven β-agonist/airway clearance protocol. Data were included only if the entire PICU stay was inclusive of each specific time period. Data elements included subject age (months), PICU length of stay (d), daily acuity (based on a single assigned value each day), weighted daily acuity (based on the actual number of nursing care hours each day), number of β-agonist interventions (aerosol and metered-dose inhaler), number of airway clearance interventions (chest physiotherapy and intrapulmonary percussive ventilation), d receiving mechanical ventilation, pediatric index of mortality 2, pediatric index of mortality 2 rate of mortality, pediatric risk of mortality 3, and pediatric risk of mortality 3 probability of death scores.
Statistical Analysis
Descriptive statistics of subject characteristics were summarized and compared between the pre-intervention (Group 1) and post-intervention (Group 2) groups. For continuous variables, mean and SD as well as median and range are presented. For categorical variables, count and percentage are presented. Continuous variables were tested for normality using the Shapiro-Wilk test. If non-normality is detected, comparison of continuous variables was performed using Mann-Whitney tests. Comparison of categorical variables was performed using chi-square tests.
In investigating the effect of the β-agonist/airway clearance protocol implementation on various subject outcomes, Poisson regression was used because all 4 outcome variables were right-skewed. Subject characteristics were included in the multivariable Poisson regression model as covariates and were assessed for collinearity. Collinearity was defined as a value >2 after taking the square root of the variance. Coefficient estimates of intervention, 95% CIs, and P values are presented for each of the outcome variables. All analyses were performed in SAS 9.4 (SAS Institute, Cary, North Carolina). P values of <.05 were considered statistically significant.
Results
For the survey, the response rate was 37% (17/46) for RT and 28% (7/25) for licensed independent practitioners, which resulted in an overall response rate of 34% for both groups (Table 4). For the 17 RT respondents, 59% were male, 47% were between the ages of 25 and 40 y, 53% were ≥40 y old, and 71% had <20 y of experience. For the 7 licensed independent practitioner respondents, 29% were male, 86% were between the ages of 25 and 40 years, 14% were ≥40 y old, and all had <20 y of experience.
Demographic Characteristics of Respiratory Therapist and Licensed Independent Practitioner Survey Responders
Survey results are shown in Table 5. Staff who completed the survey responded that they felt that subject reassessment at 24 h was an appropriate time frame (RTs, 88%; licensed independent practitioners, 72%). Both groups reportedly perceived that implementation of the β-agonist/airway clearance protocol had elevated the status of the respiratory care staff (RTs, 71%; licensed independent practitioners, 71%) and that the respiratory care staff had increased their value (RTs, 77%; licensed independent practitioners, 71%). They claimed that the licensed independent practitioners had accepted the β-agonist/airway clearance protocol as a part of the PICU standard of care (RTs, 59%; licensed independent practitioners, 86%). Responses diverged concerning the statement that licensed independent practitioners discontinued the β-agonist/airway clearance protocol, which revealed that 41% of RTs agreed that this was true versus 57% of licensed independent practitioners. Feedback also differed concerning the statement that the assessment score resulted in overtreating the patient (RTs, 29%; licensed independent practitioners, 0%). Most responders stated that they considered the assessment score to be adequately determining treatment of the patient (RTs, 77%; licensed independent practitioners, 71%) and that the β-agonist/airway clearance protocol provided consistency of care based on an objective scoring system (RTs, 76%; licensed independent practitioners, 71%). Both groups answered that the β-agonist/airway clearance protocol allowed for more effective care of patients (RTs, 88%; licensed independent practitioners, 71%) and that it was an efficient system (RTs, 71%; licensed independent practitioners, 71%). According to the survey, they also regarded the implementation of the β-agonist/airway clearance protocol as providing greater consistency of care for patients when a new licensed independent practitioner came on service (RTs, 100%; licensed independent practitioners, 57%).
Survey Responses of Respiratory Therapists and Licensed Independent Practitioners Who Totally or Somewhat Agreed With Each Statement
In the second phase of the project, comparisons for mean age, mean stay, mean daily acuity, mean weighted daily acuity, β-agonist interventions, airway clearance interventions, ventilator days, mean pediatric index of mortality 2 scores, mean pediatric index of mortality 2 rate of mortality scores, mean pediatric risk of mortality 3 scores, and mean pediatric risk of mortality 3 probability of death scores were analyzed (Table 6). For the comparison of Group 1 (pre-intervention, physician-directed orders, n = 152) with Group 2 (post-intervention, therapist-driven protocols, n = 171), there were no significant differences in mean age (78.1 months vs 60.7 months, P = .33) or sex (43.5% males vs 51.4%, P = .19). There were also no significant differences for mean daily acuity (3.3 vs 3.3, P > .99) or mean weighted daily acuity (3.9 vs 3.8, P = .79). There were no differences in means for pediatric index of mortality 2, pediatric index of mortality 2 rate of mortality, pediatric risk of mortality 3 probability of death, and pediatric risk of mortality 3 scores (P = .63, .56, .19, and .44, respectively).
Summary Statistics of All Variables Pre- and Post-Intervention
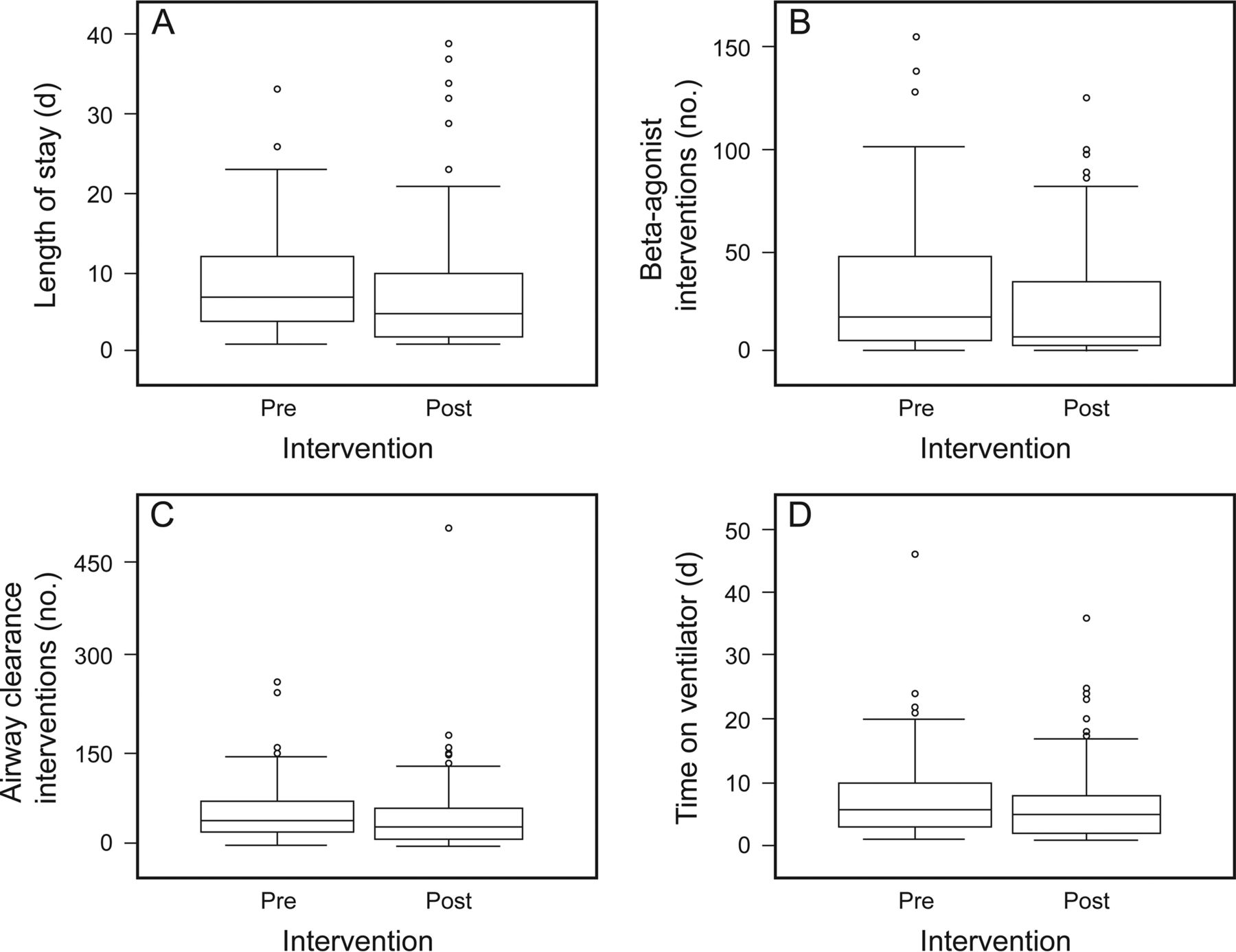
Without controlling for any subject characteristics, raw comparison of outcomes showed that all were improved in Group 2 (post-intervention), with decreased length of stay (d), fewer β-agonist therapies, fewer airway clearance therapies, and fewer days on a ventilator (Fig. 2). The effects of the intervention on various subject outcomes (length of stay, β-agonist therapies, airway clearance therapies, and ventilator days) were adjusted for subject characteristics in the Poisson regression model (Table 7). When comparing subjects with the same age, sex, weighted average daily acuity, pediatric index of mortality 2 rate of mortality, and pediatric risk of mortality 3 probability of death scores, the stay for Group 2 (post-intervention) was observed to be 0.845 d (95% CI 0.780–0.915) compared with every 1 d of stay for Group 1 (pre-intervention). This comparison represented a reduction of length of stay in the post-intervention group by 15.5% (calculated as [1 − 0.845]/1). Similarly, when adjusted for age, sex, weighted average daily acuity, pediatric index of mortality 2 rate of mortality, and pediatric risk of mortality 3 probability of death score, β-agonist interventions were observed to be 0.63 times less frequent (95% CI 0.598–0.664) for Group 2; the airway clearance interventions were noted to be 0.782 times less frequent (95% CI 0.753–0.812) for Group 2; and the number of ventilator days for Group 2 was noted to be 0.748 d (95% CI 0.685–0.819) compared with every 1 ventilator day for Group 1. These comparisons represented a reduction of 37% in the number of β-agonist interventions, 21.8% in the number of airway clearance interventions, and 25.2% in total ventilator days. Overall, comparing Group 1 (pre-implementation) with Group 2 (post-implementation), all outcome measures (length of stay, β-agonist therapies, airway clearance therapies, and ventilator days) showed statistically significant reductions adjusting for subject characteristics (P < .001).

Comparison of subject outcomes between pre- and post-intervention groups. Boxes show 25th and 75th percentiles, and center lines denote the median. Whiskers represent upper and lower adjacent values, defined as the largest observation that is ≤75th percentile + 1.5 interquartile ranges and the smallest observation that is ≥25th percentile − 1.5 interquartile ranges. Points denote outliers.
Effect of the β-Agonist/Airway Clearance Protocol Implementation on Various Subject Outcomes
Discussion
Changes in standard accepted practice are frequently met with resistance. This has been addressed by Tietsort et al2 and Stoller et al.14 As they noted, if initiation of protocols were introduced and marketed correctly, then resistance could be minimized during implementation and subsequent continuation of the program. Following guidelines similar to those that they outlined, the initiation of this project occurred with key stakeholders and included physicians, advanced practice nurses, and a core group of respiratory care personnel who worked primarily in the PICU. These groups met and discussed the possibility of introducing the β-agonist/airway clearance protocol in the PICU. The initial template was developed based on an existing protocol that was used on the medical and surgical units and was revised and enhanced to encompass the critical nature of the patients who would be treated in the PICU. After several meetings, the proposed protocol was communicated to all personnel who frequently worked in the PICU. Suggested changes were incorporated into the protocol and then re-sent for further comment and revision. Acceptance of the protocol was increased by active marketing and face-to-face discussions with all affected personnel. Additionally, the PICU respiratory care core personnel were involved in the development of the plan that was eventually adopted, and this extensive interdepartmental collaboration and cooperation may have led to an improved sense of ownership and acceptance of the protocol despite anticipated resistance to changes of this magnitude.
Acceptance of the protocol was evident in the survey responses, since overall perceptions surrounding the implementation of the β-agonist/airway clearance protocol were positive. Of particular interest in the survey responses was that both groups perceived that the implementation of the β-agonist/airway clearance protocol elevated the status and increased the value of the RTs. This reinforces previous research on these phenomena. As Metcalf et al6 report, greater use of protocols increases RT job satisfaction. Although the survey did not directly ask about job satisfaction, it can be surmised that increasing the status and value of RTs could lead to enhanced job satisfaction. The survey responses helped to validate previous research in that this protocol allowed for adequate treatment of the patient, provided greater consistency of patient care based on an objective scoring system, and was an effective and efficient system for therapeutic interventions. The protocol also allowed for a smoother transition of care when a new licensed independent practitioner came on service, allocating appropriate care to patients based on objective criteria rather than changing the therapy regimen in the absence of a change in patient status due to personal biases of the licensed independent practitioners.
In evaluating any new program, like the initiation of β-agonist/airway clearance protocol protocol, staff feedback is of extreme importance to monitor successful acceptance. This project utilized e-mail notification with an embedded link to an online survey tool, and the combined survey response rate for RTs and licensed independent practitioners of 34% appears to be consistent with the expected response rate for online-based internal surveys. For example, Sheehan15 found, after reviewing 31 studies, that the average response rate for e-mail surveys was 36.8%. Also, according to SurveyGizmo, internal surveys will generally receive a 30–40% response rate.16 Nulty17 compared paper-based survey responses versus online survey responses and found a 33% overall response rate to online surveys. The surveys provided valuable information on the appropriateness of assessment times and frequency of interventions in treating the patient.
The implementation of the β-agonist/airway clearance protocol also positively impacted outcomes in subjects admitted with acute respiratory failure. The rationale for selecting this subgroup of PICU patients was that they were thought to be the most likely to require respiratory care interventions. Additionally, this research adds evidence to the body of knowledge in a population where current information is lacking. Modrykamien and Stoller3 and Stoller18 pointed out that additional study to assess the efficacy of protocols needed to be carried out in settings like the PICU. This analysis helps to address that observation. This study indicates that subject characteristics in both pre-intervention and post-intervention groups were similar. There were overall reductions in the number of β-agonist interventions, number of airway clearance interventions, and ventilator days in the post-intervention group. Additionally, all outcome measures (length of stay, β-agonist therapies, airway clearance therapies, and ventilator days) showed statistically significant reductions, adjusting for subject characteristics in the post-intervention group. These results are considered by the authors as also being clinically important, with a reduction of at least 15% in these parameters. Although not specifically measured in this study, decreased stay in the ICU and a decrease in ventilator days were associated with significant cost savings and resulted in more efficient use of the RT's time when unnecessary treatments were eliminated.
This study has several limitations. First, this study was retrospective in design, and there was no ability to control for potential confounding variables; however, every effort was made to compare similar populations pre- and post-intervention. In addition, at the time of the study, there were no changes in either technology or clinical practice approach to explain these findings. Second, the outcomes noted in this study reflect the realities of Arkansas Children's Hospital and may not be generalizable to other institutions. Finally, although the pre- and post-intervention groups were similar, factors that could not be accounted for may have influenced the reported findings.
Conclusion
This study adds to the growing number of publications addressing RT-driven protocols. It also fills a niche in the knowledge base where clinical data are scant; specifically, the PICU. Implementation of a β-agonist/airway clearance protocol was perceived as a positive development by RTs and licensed independent practitioners based on the survey responses. The implementation of the β-agonist/airway clearance protocol resulted in significant reductions of patient interventions and improved outcomes by decreasing ICU stay and ventilator days.
Acknowledgments
We thank the RTs and licensed independent practitioners from the PICU at Arkansas Children's Hospital for input and support for this project.
Footnotes
- Correspondence: Gary R Lowe MEd RRT-NPS RPFT, Respiratory Care, Slot 303, 1 Children's Way, Little Rock, AR 72202-3591. E-mail: lowegr{at}archildrens.org.
Mr Lowe presented a version of this paper at the 60th International Respiratory Congress of the American Association for Respiratory Care, held December 9-12, 2014, in Las Vegas, Nevada, and the 61st International Respiratory Congress of the American Association for Respiratory Care, held November 7-10, 2015, in Tampa, Florida.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 380
- Copyright © 2017 by Daedalus Enterprises





{kind=link}
{kind=link}