

Abstract
BACKGROUND: Increasing numbers of individuals are being initiated on home mechanical ventilation, including noninvasive (bi-level) and invasive mechanical ventilation delivered via tracheostomy due to chronic respiratory failure to enable symptom management and promote quality of life. Given the high care needs of these individuals, a better understanding of the indications for home mechanical ventilation, and health-care utilization is needed.
METHODS: We performed a retrospective cohort study using provincial health administrative data from Ontario, Canada (population ∼13,000,000). Home mechanical ventilation users were characterized using health administrative data to determine the indications for home mechanical ventilation, the need for acute care at the time of ventilation approval, and their health service use and mortality rates following approval.
RESULTS: The annual incidence of home mechanical ventilation approval rose from 1.8/100,000 in 2000 to 5.0/100,000 in 2012, or an annual increase of approximately 0.3/100,000 persons/y. The leading indications were neuromuscular disease, thoracic restriction, and COPD. The indication for the remainder could not be determined due to limitations of the administrative databases. Of the 4,670 individuals, 23.0% commenced home mechanical ventilation following an acute care hospitalization. Among individuals who survived at least 1 y, fewer required hospitalization in the year that followed home mechanical ventilation approval (29.9% vs 39.8%) as compared with the year prior.
CONCLUSIONS: Utilization of home mechanical ventilation is increasing in Ontario, Canada, and further study is needed to clarify the factors contributing to this and to further optimize utilization of health-care resources.
Introduction
Recent guidelines recommend the use of either invasive or noninvasive ventilation (NIV) as home mechanical ventilation for treatment of chronic respiratory failure.1–4 Home mechanical ventilation has been shown to be effective in prolonging life and improving health-related quality of life.5 Given the expanding use of home mechanical ventilation, a better understanding of the profile of individuals using it and the impact on the health-care system is needed.
A growing body of scientific evidence supports the provision of home mechanical ventilation for life extension in neuromuscular conditions causing respiratory failure, such as amyotrophic lateral sclerosis (ALS),6 muscular dystrophy,7 and other less common neuromuscular diseases.1 For such patients, ventilation has also been shown to improve health-related quality of life6,8 and reduce symptoms related to chronic respiratory failure, such as dyspnea, daytime sleepiness, and fatigue. Home mechanical ventilation for neuromuscular and chest wall disease has been shown to reduce the frequency of emergency department visits and hospital admission.5 Studies also support ventilation for obesity-hypoventilation syndrome to lower the risk of death,9 improve daytime sleepiness10 and quality of life, as well as to lower health-care utilization.11 Home mechanical ventilation for lung disease, such as COPD, remains controversial,12,13 although it may be used to reduce hospitalizations14 or as a bridge to transplantation. Additionally, home mechanical ventilation may be used to facilitate discharge from hospital and to prevent individuals from needing ongoing institutional care, so that they may preserve their independence.1,3
Various regional and national approaches to the delivery of community support services for home mechanical ventilation have been developed both within Canada and internationally with substantial variation in the types of patients receiving it as well as the level and type of service provision.4,15–18 Although the benefits of home mechanical ventilation to the individual, their family members, and the health-care system are relatively undisputed, the optimal way to support individuals to live at home and to reduce avoidable acute care utilization remains unknown. One comparison of 2 systems showed divergence in the characteristics of home mechanical ventilation users and of the service provision; however, quality of life was not different.18 Describing the characteristics of home mechanical ventilation recipients and improving the understanding of service provision to them is the first step in establishing their needs and improving health-care delivery and outcomes.
Previous studies have used surveys15,16,19,20 to describe the prevalence and characteristics of home mechanical ventilation users and their utilization of the health-care system. These surveys, however, may underestimate the frequency of home mechanical ventilation initiation by relying on volunteer reporting and do not provide information about changes over time given their cross-sectional nature. Therefore, our primary objective was to examine the incidence of home mechanical ventilation at a population-based level in Ontario, Canada, over a 12-y time frame. Secondary objectives included describing the indications for home mechanical ventilation, trends in 1- and 3-y mortality, and their health-care utilization before and after initiation of home mechanical ventilation.
QUICK LOOK
Current knowledge
Previous studies of home mechanical ventilation have described the prevalence of and indications for home mechanical ventilation. These measures vary widely among industrialized nations and even between regions in the same country. These reports are based on surveys of referral centers and may not represent the population.
What this paper contributes to our knowledge
We used provincial health administrative databases to identify first time users of home mechanical ventilation and determine the incidence per year. We describe the leading indications for mechanical ventilation. We also determined health-care utilization changes and describe the mortality rates of individuals using home mechanical ventilation.
Methods
Study Description
We conducted a retrospective population-based cohort study to characterize home mechanical ventilation users in Ontario, the largest province of Canada, with a population of approximately 13 million individuals.
We conducted our study according to a prespecified protocol approved by the research ethics board at Sunnybrook Health Sciences Centre (Toronto, Ontario), and reporting of the study followed guidelines for observational studies using routinely collected health data.21
Data Sources
Ontario has a universal, publicly funded, single-payer health-care system with health-care data housed in large population-based health administrative databases. Relevant data sets were linked using unique encoded identifiers and analyzed at the Institute for Clinical Evaluative Sciences. Individuals with an approved request for equipment for home mechanical ventilation, which includes ventilators capable of either invasive or noninvasive ventilation, were identified from the Assistive Devices Program database, a database that contains approvals for various assistive devices, including ventilators. All individuals in Ontario residing outside a hospital or chronic care facility with a clinically recognized need for home mechanical ventilation are eligible to receive equipment and related consumables when requested by an eligible health-care provider and subsequently approved by the Ministry of Health and Long Term Care. Additional information on these individuals was obtained from the following databases: the Ontario Health Insurance Plan, which contains all billing for physician services, including those for procedures; the Discharge Abstract Database, which contains all data on demographic and clinical information and responsible diagnoses for all hospitalizations; the National Ambulatory Care Reporting System, which contains all emergency department visits, ambulatory 1-d surgeries, and select ambulatory clinics (eg, dialysis); the Registered Persons Database, which contains demographic data, including death outside of a hospital setting; the Continuing Care Reporting System, which contains data on facility-based continuing (residential) care services; the National Rehabilitation Reporting System, which contains data on in-patient rehabilitation programs; and the Home Care Database, which contains data about provincially funded home care use. Diagnoses in the databases are documented using the International Classification of Disease 9th Revision (before 2002) or 10th Revision (after 2002) or database-specific codes. Intercensal populations were estimated using data from the Ontario Ministry of Health and Long-Term Care: IntelliHEALTH ONTARIO.
Participants
Inclusion Criteria
We obtained all records of ventilator equipment and supplies from the Assistive Devices Program database. Individuals were included in the cohort if a request for a ventilator (capable of either invasive or noninvasive ventilation) was submitted and approved between April 1, 2000, and March 31, 2013, and they were ≥18 y of age on the approval date. We defined the index date as the home mechanical ventilation approval date from the Assistive Devices Program database. Individuals started on home mechanical ventilation with equipment loaned from another provider or purchased privately or started on acute care ventilation during a hospitalization could not be identified. We used procedural codes for tracheotomy in the 5 y before the Assistive Devices Program approval date as a surrogate for individuals receiving invasive ventilation, as we could not distinguish applications for NIV from those for invasive ventilators. We did not consider devices typically used to treat sleep apnea, namely CPAP or bi-level positive airway pressure devices incapable of providing a backup rate as mechanical ventilation.
Exclusion Criteria
Individuals were excluded if the Assistive Devices Program database indicated that they were long-term care residents. Additional exclusion criteria comprised records with invalid/inaccurate information, such as an invalid health card number, age missing or >105 y, sex missing, death date recorded before signed consent for a ventilator, and not being an Ontario resident when their ventilator was approved. In cases where multiple request records were noted, we restricted inclusion to the first record for that individual (assumed to be the first/incident application).
Cohort Characteristics
For all included individuals, we determined age, sex, and rural residence at the time of home mechanical ventilation approval. Neighborhood income quintiles were determined based on home address and an algorithm from Statistics Canada.22 We determined the Charlson-Deyo comorbidity score to establish the overall burden of other medical conditions.23 The Charlson-Deyo score is a composite of 19 common comorbidities,24 which is used to predict mortality24 and health-care utilization.25 Home mechanical ventilation users who did not have any hospitalizations were assigned a score of zero. We identified COPD, asthma, and congestive heart failure as comorbidities using validated algorithms,26–28 given that they may have contributed to the need for home mechanical ventilation, but did not consider them the primary indication if other conditions were present, since Canadian guidelines do not support use of home mechanical ventilation for these conditions,1 and we could not determine the severity of disease.
Incidence of Home Mechanical Ventilation
The incidence of home mechanical ventilation was defined as the number of new home mechanical ventilation approvals per 100,000 adults in Ontario per fiscal year.
Primary Indication for Home Mechanical Ventilation
As the Assistive Devices Program database does not include the indication for home mechanical ventilation, we used health administrative databases to identify potential primary indications for ventilation. A priori, we identified the following list of potential indications: thoracic cage restriction disease (kyphoscoliosis, fibrothorax, thoracoplasty, obesity, thoracic resection) and neuromuscular disease (ALS, muscular dystrophy, diaphragmatic paralysis, myasthenia gravis, Guillain–Barré syndrome, spinal cord injury, stroke/transient ischemic attack, multiple sclerosis, Parkinson's disease, neuropathy, post-polio syndrome, spina bifida, spinal muscular atrophy). We sought diagnostic codes from hospitalizations in the year preceding home mechanical ventilation approval. We also searched for diagnoses from physician billing, rehabilitation, and chronic care admissions during this time.
Urgency of Home Mechanical Ventilation Initiation
We identified patients who were hospitalized in the month before home mechanical ventilation approval and determined whether they received critical care services and/or mechanical ventilation.29
Health-Care Utilization
We compared health-care utilization in the year before initiation of home mechanical ventilation with the year following approval excluding the 30 d before and 30 d following approval, given the increased utilization related to initiation of home mechanical ventilation, which might bias the results of a pre/post comparison. We restricted this analysis to users who survived at least 1 y to ensure that information was available for the complete period. We considered that inclusion of users who died before the full year would bias results, given censoring of the health-care utilization due to death. Specifically, we looked at hospitalizations, emergency department visits, and out-patient respirology/pulmonary medicine and out-patient neurology specialist physician visits identified using specialty-specific billing codes.
Mortality After Home Mechanical Ventilation
We determined the 1- and 3-y mortality rate per 100 individuals following the initiation of home mechanical ventilation. We stratified by age groups 18–39, 40–64, and 65 y and older, given the anticipated higher mortality in older individuals.
Analysis
We reported continuous variables as means and SD or medians and interquartile ranges where appropriate. Categorical variables were reported as frequencies and proportions and were compared using chi-square tests. For health-care utilization, we compared frequency of health service use before and after home mechanical ventilation initiation using the Fisher exact test. Results were reported with 95% CI and P values where appropriate. We used linear regression to determine the mean rate of increase in incidence of home mechanical ventilation per year and used the Cochran–Armitage test to examine change over time. All statistical tests were completed using Stata release 13 (StataCorp, College Station, Texas) and SAS for UNIX version 9.3 (SAS Institute, Cary, North Carolina).
Results
Cohort Characteristics
We identified 4,670 individuals approved for home mechanical ventilation from April 1, 2000, to March 31, 2013 (fiscal years 2000–2012). Characteristics of these subjects are shown in Table 1. The incidence of approvals increased from 1.8 per 100,000 adults in 2000 to 5.0 per 100,000 adults in 2012 (Fig. 1). This is equivalent to a mean increase of 0.3/100,000 (95% CI 0.2/100,000 to 0.4/100,000). At least one neuromuscular disease or thoracic cage disorder was identified for 44.9% of individuals. The most frequent neurological conditions were ALS (7.5%) and muscular dystrophy (6.8%). Of thoracic cage restriction conditions, obesity was the most common, affecting 15.9% individuals. COPD, congestive heart failure, and asthma were found in 31.3, 22.6, and 13.0% of the cohort as a whole, but COPD without other potential indications was found in 18.8% of the cohort. Almost 8% of individuals had undergone tracheostomy before home mechanical ventilation approval, indicating the need for invasive ventilation. Over the course of the study period, the proportion of new users who had undergone tracheotomy ranged from 12.2% in 2000 to 6.3% in 2011 with a significant decline annually in the proportion of invasively ventilated individuals (P = .01).
Characteristics Home Mechanical Ventilation Users in Ontario, Canada, 2000–2012

Incidence of newly approved assistive device program ventilator applications per 100,000 adults ≥18 y old. P < .001 for trend. Incidence was calculated as the number of new approvals/fiscal year/100,000 adults ≥18 y old based on population.
Urgency of Home Mechanical Ventilation Initiation
Twenty-three percent of individuals were hospitalized in the 30 d before home mechanical ventilation approval. Of these, 100% required ICU admission and 72.5% received mechanical ventilation in hospital. The median (interquartile range) hospital stay was 15 (7–36) d. The remaining 77.0% had no acute care hospital stay within 30 d of approval and therefore commenced home mechanical ventilation in an out-patient setting.
Health-Care Utilization
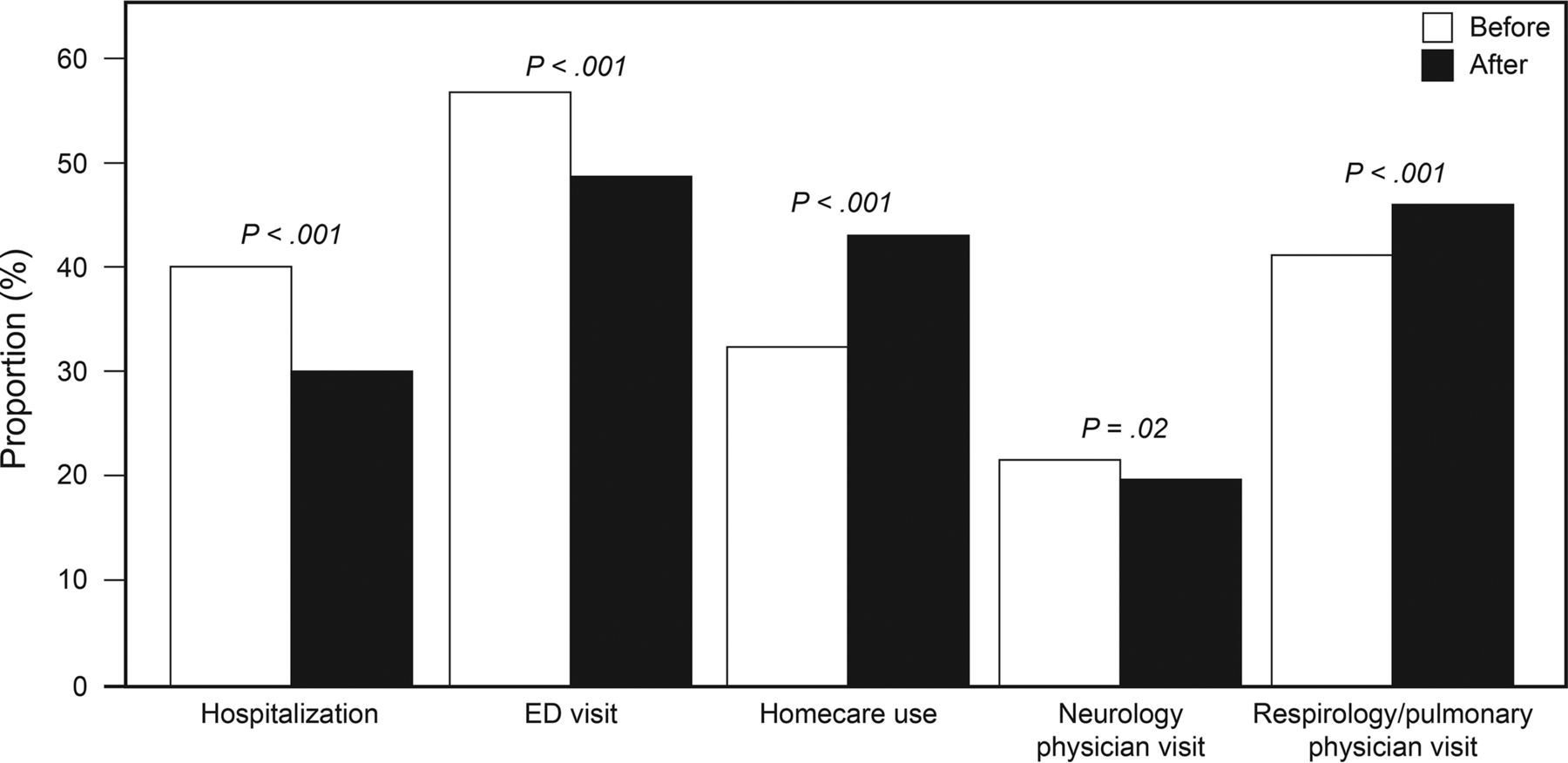
Of the 4,670 individuals approved for home mechanical ventilation, 75.3% survived to 1 y and were included in our analysis of health-care utilization. Overall, fewer individuals were hospitalized in the year following home mechanical ventilation approval compared with the year prior (29.9% vs 39.8%, P < .001), excluding the 30 d immediately before and after home mechanical ventilation approval. The proportion requiring at least one emergency department visit decreased from 1,998/3,517 (56.8%) in the year before home mechanical ventilation approval to 1,725/3,517 (49.0%) following approval (P < .001). In contrast, the number of individuals using home care services increased from 32.9% in the year before home mechanical ventilation approval to 43.9% in the 12 months after (P < .001). Respirology/pulmonology out-patient visits increased from 41.9% in the year before home mechanical ventilation approval to 47.0% in the year after (P < .001), whereas neurology out-patient visits dropped from 21.8% in the year before to 19.8% in the year after (P = .02) (Fig. 2).

Health services utilization in the year before and year after home mechanical ventilation approval. Health service utilization excludes 30 d before and after home mechanical ventilation approval. Use was calculated as a proportion of surviving cohort members who had that type of health-care contact. ED = emergency department.
Mortality After Home Mechanical Ventilation
Crude 1- and 3-y mortality rates remained largely stable from 2000 to 2012 and increased by age strata. The only significant change observed during the study period was in 1-y mortality in 40–64-y-old subjects (Table 2).
1- and 3-Year Mortality Trends After HMV Approval
Discussion
We conducted a 12-y retrospective cohort study of home mechanical ventilation users using administrative data and found that the incidence of home mechanical ventilation approval almost tripled. Only a minority required invasive ventilation, and few were hospitalized in the 30 d before the approval of home mechanical ventilation, suggesting that most were identified and initiated in out-patient settings. We found for individuals that survived for 12 months after home mechanical ventilation approval that the overall proportion of hospitalizations and emergency department visits declined significantly, comparing the 12 months before and 12 months after approval, whereas home care use and respiratory specialist out-patient visits increased. Mortality among these subjects was largely unchanged.
The reason for the increased incidence of home mechanical ventilation over time (from 1.8/100,000 in 2000 to 5.0/100,000 in 2012) is probably multifactorial; however, due to the limited information available from health administrative databases, we can only speculate on the reasons. One reason may be the steadily rising prevalence of obesity in Canada.30 Another might be the development of specialized centers and physician leaders who can influence the overall attitudes toward provision of home mechanical ventilation and increase incidence rates.31 A now dated European survey reported a European prevalence of 6.6/100,000, although this varied from 0.1 in Poland to 9.6/100,000 in Denmark, and reported that the indication for mechanical ventilation varied widely between countries.15 This survey also showed no consistency in the proportion of individuals receiving invasive ventilation, although it was highest for those with a neuromuscular indication. A more recent Canadian survey reported a prevalence of 12.9/100,000 and reported that more than half of individuals had neuromuscular disease, with lung disease representing <5.0%.16 Neither reported the incidence of home mechanical ventilation use to provide data comparable with our findings. Conversely, we were unable to report on prevalence, as administrative databases did not enable us to determine those individuals who had discontinued home mechanical ventilation.
Many incident cases were not hospitalized in the 30 d before home mechanical ventilation approval and were therefore initiated on therapy in another setting. Home-based and polysomnographic home mechanical ventilation starts have been shown to be acceptable in previous studies,32,33 and this indicates that this approach has been adopted.
The reduction in hospitalizations (from 39.8 to 29.9%) following home mechanical ventilation approval has been shown in cohort studies of individuals with neuromuscular disease5 or obesity.11,34 Our findings confirm this finding at a population-based level. This is relevant, given the resources that need to be invested to provide home mechanical ventilation in constrained health-care systems. The frequency of pulmonary medicine out-patient consultations for home mechanical ventilation users increased but remained low overall (41.8–47.0%), which is concerning, since few other physicians have expertise in management of chronic respiratory failure requiring home mechanical ventilation. It is surprising that neurology consultations were found for only about 1 in 5 users, which is about half the proportion who had a neurological diagnosis. It may be that some respirologist/pulmonologists and neurologists are billing using internal medicine codes or that home mechanical ventilation is being managed by non-respiratory sleep physicians, intensive care physicians, or internists.
In our study, 1 and 3-y mortality varied by age strata, but there was little significant change over the 12-y period studied. Our mortality rates are consistent with the range of what has been reported previously. In individuals with ALS, 1- and 3-y mortality has been reported as 17.0–27.0 and 47.0–79.0%, respectively, in individuals using home mechanical ventilation.35 Patients with less progressive conditions, such as obesity-hypoventilation syndrome,36 have been reported to have 10–20% mortality observed at 4 y in home mechanical ventilation-treated individuals. The lack of change in mortality suggests that the indications and care for home mechanical ventilation users are similar across the time periods and that therapy options remain limited to prolong life for affected individuals.
There are several limitations to our study. First, in our cohort, we could not confirm the primary indication for home mechanical ventilation approvals, as the primary indication was not identifiable from administrative data. Therefore, using codes assigned for diagnoses arising from episodes of health-care utilization, we took a conservative approach and prioritized neuromuscular or thoracic cage-restricting conditions over COPD or lung disease. We made this choice because home mechanical ventilation use in COPD is discouraged in Canada.1 Notwithstanding Canadian guidelines, we found that 18.8% of our cohort had COPD without other indications for home mechanical ventilation initiation. Second, home mechanical ventilation adherence data were not available. Consequently, we were not able to determine the prevalence of home mechanical ventilation use within our cohort, although it is likely that most 1-y survivors were still using home mechanical ventilation. Third, we had to use the home mechanical ventilation approval date as a surrogate for a start date. Initiation of home mechanical ventilation may have predated the approval for hospitalized individuals if they were using an alternative non-government funded and short-term ventilator supplier to facilitate transition home. For those started as out-patients, therapy would follow soon after approval, since the home mechanical ventilation unit needs to be shipped and set up. Fourth, we did not assess trends in indications for home mechanical ventilation over time. These data may provide further explanation of the drivers of increasing incidence of home mechanical ventilation and should be explored in future studies. Fifth, we could not quantify the proportion of health-care utilization directly attributable to home mechanical ventilation opposed to that required for management of underlying disease and are therefore unable to comment on attributable costs of home ventilation.
Conclusions
The incidence of home mechanical ventilation use in Ontario has risen significantly; however, home mechanical ventilation users have lower rates of acute care health-care utilization. This suggests that home mechanical ventilation is having a positive impact on the health-care system. Areas for future study include elaborating on the reasons for the growth in home mechanical ventilation approvals by properly tracking new home mechanical ventilation starts, particularly the indication for therapy, as well as measuring patient follow-up and important outcomes prospectively. This may involve establishment of a registry of home mechanical ventilation users as well as leveraging existing technologies that allow monitoring of therapy adherence and efficacy.
Acknowledgments
Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information. However, the analyses, conclusions, opinions, and statements expressed herein are those of the authors and not necessarily those of the Canadian Institute for Health Information.
Footnotes
- Correspondence: Marcus Povitz MD MSc FRCPC, London Health Sciences Centre, 800 Commissioners Road East, Room E6-202, London, Ontario N6A 5W9, Canada. E-mail: marcus.povitz{at}lhsc.on.ca.
This study was supported by the Institute for Clinical Evaluative Sciences (ICES) Western site. ICES is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). Core funding for ICES Western is provided by the Academic Medical Organization of Southwestern Ontario (AMOSO), the Schulich School of Medicine and Dentistry (SSMD), Western University, and the Lawson Health Research Institute (LHRI). The opinions expressed in this document are solely those of the authors and do not represent an endorsement by or the views of the United States Air Force, the Department of Defense, or the United States Government. The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 491
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}