

Abstract
BACKGROUND: Manually-assisted coughing and mechanical insufflation-exsufflation (MI-E) are commonly used in patients with Duchenne muscular dystrophy (DMD). Few studies have compared cough peak flow (CPF) with manually-assisted coughing to other methods, such as MI-E + manually-assisted coughing. In addition, few studies have reported the reliability of the measured CPF values. This study aimed to compare CPF with different cough-assistance methods and to examine the reliability of CPF data.
METHODS: The study included 12 subjects with DMD (mean age, 34 ± 8 y). CPF, CPF + manually-assisted coughing (assisted CPF), maximum insufflation capacity (MIC) + CPF (MIC-CPF), MIC + manually-assisted coughing (MIC+assisted CPF), MI-E (MI-E–CPF), and MI-E + assisted CPF were measured. A spirometer was used to compare CPF measurements obtained with each of the cough-assist techniques. The reliability of the measured CPF values was analyzed using Bland-Altman analysis.
RESULTS: CPF was 59 ± 34 L/min, assisted CPF was 113 ± 32 L/min, MIC-CPF was 170 ± 30 L/min, MIC+assisted CPF was 224 ± 62 L/min, MI-E–CPF was 199 ± 40 L/min, and MI-E + assisted CPF was 240 ± 38 L/min. A fixed and proportional bias was found in the CPF measurements made with the peak flow meter and the spirometer. The average 95% CI in the difference between peak flow meter, MI-E, and CPF obtained using the spirometer were −7.45 to −1.95 and −1.45 to 4.95, respectively. Test for correlation was r = 0.54 (P < .001) for CPF (peak flow meter) and CPF (spirometer) and r = 0.17 (P = .17) in CPF (MI-E) and CPF (spirometer), respectively.
CONCLUSION: MI-E + assisted CPF was the highest. The CPF measured with the peak flow meter suggested underestimation.
- manually-assisted coughing
- mechanical insufflation-exsufflation
- cough peak flow
- Duchenne muscular dystrophy
Introduction
Cough peak flow (CPF) is considered an index of expectoration of airway secretions in subjects with Duchenne muscular dystrophy (DMD).1,2 Manual or mechanical cough assistance is an approach to increase CPF.2 Manually-assisted coughing (assisted CPF) provides assistance with regard to inspiration and exhalation.3,4,5 There is a procedure to obtain maximum insufflation capacity (MIC), which is the volume of air that can be held in the lungs with the glottis closed, during inspiration assistance.6 CPF with MIC support (MIC-CPF) was measured with voluntary coughing after breath stacking of 3 or 4 insufflations with a manual resuscitation bag-valve-mask. To measure the MIC+assisted CPF, the subjects were deeply insufflated and then asked to forcefully cough, with the abdominal thrust timed to glottic opening. We used thoraco-abdominal compression during coughing as the exhalation assistance method.7
Assisted CPF provides support by pushing the upper abdomen or chest wall in synchrony with the subject's own coughing effort. Mechanical insufflation-exsufflation (MI-E) involves insufflation of the lungs with positive pressure, followed by exsufflation with active negative pressure that creates a peak and sustained flow high enough to provide adequate shear and velocity to loosen and move secretions toward the mouth for suctioning or expectoration.8 Mechanically-assisted coughing (MI-E–CPF) is an airway clearance method in which the thorax or abdomen is compressed in synchronization with MI-E.8–10
In preliminary research on the augmentation of CPF,9,10 MI-E–CPF showed the highest value among the measured modalities: CPF, maximum insufflation capacity + CPF (MIC-CPF), maximum insufflation capacity + manually-assisted coughing (MIC+assisted CPF), and MI-E–CPF. In addition, in systematic reviews, MI-E produced the greatest CPF increase among all of the assessed procedures.11–13 Mechanically-assisted cough is not only effective, but research has shown that CPF actually increased.8–10 However, Kim et al14 reported that CPF increased more with mechanically-assisted coughing compared to MI-E. On the other hand, Lacombe et al15 reported that MIC+assisted CPF yielded significantly higher values than CPF associated with MI-E or mechanically-assisted coughing. A previous study showed that set pressures for MI-E vary (30–40 cm H2O), and this range may be too low for optimal effectiveness.15 Effectiveness is influenced by the set pressure of MI-E, and it is unknown whether MIC+assisted CPF or MI-E–CPF produces the higher CPF.
Bach16 reported that a set pressure of MI-E of 54 cm H2O is most effective. A peak flow meter is widely used for CPF evaluation because it is appropriate for continuous clinical assessment.2 Although a peak flow meter is accurate when the CPF is ≥ 270 L/min, there is a possibility of overestimation when the value is < 270 L/min.17 In addition, it has been reported that CPF measured using a peak flow meter is lower than that measured using a differential pressure-type flow meter (pneumotachograph).17 Thus, instrumental differences in measurement may influence the error in measurement. Preliminary research comparing various cough-assist techniques used CPF values obtained from a pneumotachograph. It is necessary to examine the reliability of CPF measured using a peak flow meter and MI-E to determine the significance of measurement with the same instrument and to perform comparisons. To compare measured values obtained from the same equipment, it is necessary to investigate the reliability of CPF measured using a peak flow meter and MI-E.
The purpose of this study was to compare and assess the reliability of cough-assisted CPF to determine the most effective cough-assistance approach for subjects with DMD.
QUICK LOOK
Current knowledge
Measurement of cough peak flow (CPF) is possible using a peak flow meter and a mechanical insufflation–exsufflation (MI-E) display. The set pressure of MI-E varies according to the patient's condition.
What this paper contributes to our knowledge
There was no statistically significant difference in CPF due to differences in MI-E (± 40 cm H2O), maximum insufflation capacity + manually-assisted coughing, and MI-E + manually-assisted coughing. Using spirometry results as a standard, the CPF displayed on the MI-E device had high reliability. There was a negative fixed bias in the CPF of the peak flow meter.
Methods
This cross-sectional study included 12 subjects with DMD admitted to Akita National Hospital. The mean age was 34 ± 8 y, and the period of hospital stay was 13 ± 8 y. Six subjects received noninvasive ventilation for 1 d. Six subjects who carried out activities of daily living all required assistance (Table 1). The inclusion criteria were age > 12 y, CPF < 160 L/min, and the use of MI-E. The exclusion criteria were history of previous pneumothorax and no requirement of MI-E in patients with CPF > 160 L/min. The criteria for cancellation of treatment were rejection by the patient, fatigue, hyperventilation, worsening of oxygenation, sense of incongruity, intragastric air inhalation, and barotrauma. We explained the purpose and methods of the research to all subjects, the expected effects, the benefits of research cooperation, and the ability to appeal after reporting any adverse effects. We informed them that no identifying information would be used so as to protect their privacy. Subjects who provided informed consent were included. This study was approved by the ethics committee of Akita National Hospital (IRB No. 28/5).
Characteristics of Subjects With DMD
For the measurement of CPF, assisted CPF, MIC-CPF, and MIC+assisted CPF, an automatic spirometer for electronic diagnosis (Auto Spiro AS 507, Minato, Tokyo, Japan) and a peak flow meter (Philips Respironics, Bend, Oregon) were connected (Fig. 1). The same examiner performed 2 random measurements on the same day. The transducer of the automatic spirometer was connected to the mouthpiece of the peak flow meter with tape. CPF was obtained using the peak expiratory flow output from the spirometer and the value from the peak flow meter. For the measurement of MI-E–CPF and MI-E+assisted CPF, an automatic spirometer and MI-E (Cough Assist E 70, Philips Respironics) were connected (Fig. 2).

Connection of the spirometer (Minato) and peak flow meter (Philips Respironics).

Connection of the spirometer (Minato) and mechanical insufflation–exsufflation device (Philips Respironics).
Regarding the connection method, a flexible tube was connected to the MI-E device, the transducer of the automatic spirometer was connected, and a mask was connected. The peak expiratory flow output from the automatic spirometer was recorded as CPF(s), and the CPF on the MI-E display was recorded as CPF(m). Without using an airway pressure meter for MIC measurement in MIC-CPF and MIC+assisted CPF, we pressurized a bag-valve-mask until subjects could not inhale further. The examiner's pressurization method was subjectively judged according to the resistance of the bag-valve-mask, and there were no criteria. In addition, the MI-E setting used was ± 40 cm H2O (1.5 s), with a rest time of 2 s. Whereas a study by Bach and Mehta18 identified 54.1 cm H2O as the most effective pressure, we used a setting pressure that is most frequently used in the clinical setting.8,19,20
Measurements were performed in the supine position because the electric wheelchairs used by subjects do not have a reclining and tilt function, and subjects were unable to maintain a seated position in the hospital bed.
Statistical Analysis
To compare the CPF of each of the cough-assistance approaches, we mainly used CPF measured with a spirometer, indicated as CPF(s). For statistical analysis, one-way analysis of variance and a multiple comparison test (Tukey method) were used. To assess the relationship between CPF(s) and CPF(p) and between CPF(s) and CPF(m), Spearman's rank correlation coefficient was used for relative reliability. Bland-Altman analysis was used for absolute reliability.21 If a systematic error was noted, the 95% limit of agreement ranges were calculated; however, if there was no systematic error, the 95% minimal detectable change was calculated. For all statistical analyses, Statcel 3 (OMS Publishing, Tokyo, Japan) was used.
Results
The CPF(s) values obtained from the automatic spirometer were as follows: CPF, 59 ± 35 L/min; assisted CPF, 113 ± 32 L/min; MIC-CPF, 170 ± 30 L/min; MIC+assisted CPF, 224 ± 62 L/min; MI-E–CPF, 199 ± 40 L/min; and MI-E+assisted CPF, 240 ± 38 L/min. Compared with unassisted CPF, the CPF value was higher with all the cough-assistance methods. In addition, CPF increased when inspiration and exhalation assistance were provided rather than when only exhalation assistance was provided. There was no statistically significant difference among MI-E–CPF, MIC+assisted CPF, and MI-E+assisted CPF, which were considered high according to the guidelines.12,13 However, the highest value was for MI-E+assisted CPF (Table 2).
Comparison of Unassisted/Manual and Mechanically Assisted Cough Peak Flow (Spirometer)
The sample size of CPF(p) and CPF(s) was 96, and the sample size of CPF(m) and CPF(s) was 48. The correlation findings of CPF(p) and CPF(s) were as follows: CPF (rs = 0.93, P < .001, n = 24), assisted CPF (rs = 0.97, P < .001, n = 24), MIC-CPF (rs = 0.81, P < .001, n = 24), and MIC+assisted CPF (rs = 0.96, P < .001, n = 24). The correlation findings of CPF(m) and CPF(s) were as follows: MI-E–CPF (rs = 0.94, P < .001, n = 24) and MI-E+assisted CPF (rs = 0.98, P < .001, n = 24). Regarding the Bland-Altman analysis, agreement between the measurement of CPF obtained with the spirometer and peak flow meter was assessed using data from CPF, assisted CPF, MIC-CPF, and MIC+assisted CPF (n = 96). Subsequently, the agreement between the measurements of CPF obtained with the spirometer versus measurements obtained with MI-E was evaluated, using MI-E–CPF and MI-E+assisted CPF data (n = 48). In the Bland-Altman analysis, a fixed and proportional bias was found in CPF(p) and CPF(s) at sample a size of n = 96. The average 95% CI in the difference between CPF(p), CPF(m), and CPF(s) were −7.45 to −1.95 and −1.45 to 4.95, respectively. Bland-Altman analysis of CPF measurements indicated that the CPF(p) measurements were markedly lower than the CPF(s) measurements [bias (mean 95% limit of agreement), −4.7 L/min (−30.7 to 21.3 L/min)] (Fig. 3). Test for no correlation was r = 0.54 (P < .001) [bias (mean 95% limit of agreement) −4.7 L/min (−128.7 to 76.6%)]. There was no proportional or fixed bias in CPF(m) and CPF(s) at a sample size of n = 48 (Fig. 4). The 95% minimal detectable change for CPF(m) and CPF(s) was 21.8 L/min. Test for no correlation was r = 0.17 (P = .17).
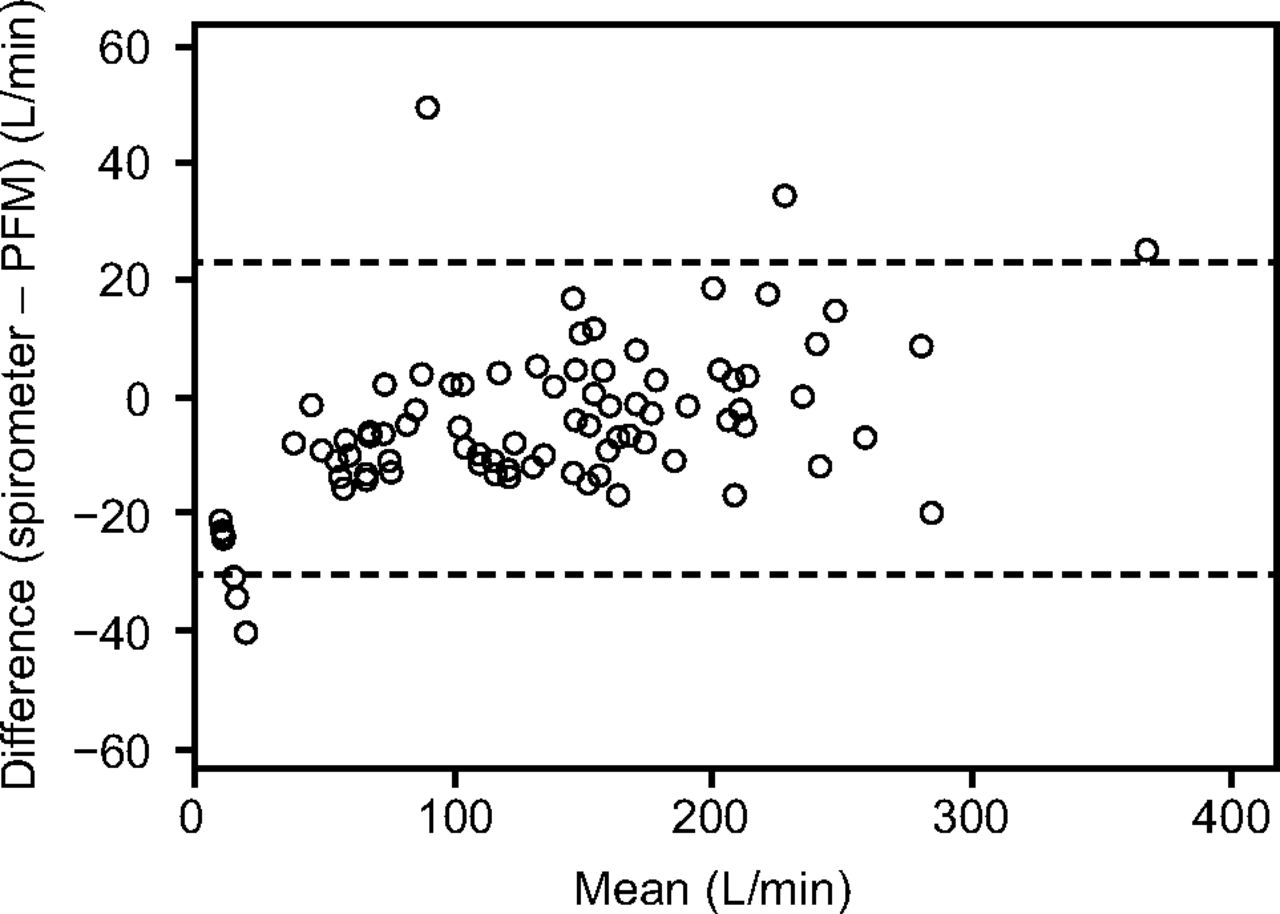
Bland-Altman plot representing the agreement between cough peak flow measurements obtained with a spirometer and with a peak flow meter. The difference between the 2 measurements is plotted against the mean of the 2 measurements. The solid and dashed lines indicate the difference between measurements (bias) and the upper and lower 95% limits of agreement (bias ± 1.96 SD).

Bland-Altman plot representing the agreement between cough peak flow (CPF) measurements obtained with a spirometer and with a mechanical insufflation–exsufflation (MI-E) device. The difference between the 2 measurements is plotted against the mean of the 2 measurements. There was no proportional or fixed bias of CPF determined with MI-E and CPF determined with automatic spirometry.
Discussion
In this study, the CPF of unassisted and manual/mechanically-assisted coughing was compared using the same equipment. There was no statistically significant difference in MIC+assisted CPF and MI-E+assisted CPF when compared with CPF(s) MI-E obtained using the automatic spirometer, which was connected to the peak flow meter and MI-E. Using the automatic spirometer, we examined the reliability of the peak flow meter and MI-E. In Bland-Altman analysis, negative fixed bias and proportional bias were recognized for peak flow meter and CPF from spirometer. The 95% minimal detectable change for CPF(m) and CPF(s) was 21.8 L/min, and the limit of agreement of CPF(p) and CPF(s) was −30.7 to 21.3 L/min.
Our hypothesis was that MI-E–CPF has the highest value. However, we found no significant difference among MIC+assisted CPF, MI-E+assisted CPF, and MI-E–CPF. The pressure of MI-E in this study was ±40 cm H2O. On the other hand, there was no upper limit on the pressure of the bag-valve-mask. The bag-valve-mask pressure might have been higher than the MI-E pressure, and inspiration might have been higher than the MI-E value. In addition, the pressure in the MIC procedure might have been higher than that in the MI-E procedure. Therefore, we believe that the amount of inspiration was high.
In a previous study, it was shown that CPF increased as MIC increased.22 In other words, the bag-valve-mask pressure was higher than the MI-E pressure, which is considered to be different from MI-E–CPF due to the increase in the volume of air intake. In MIC+assisted CPF, high peak flow is achieved by creating high intrathoracic pressure, whereas MI-E shifts instantly from positive to negative pressure to simulate the pressure differential achieved with the normal cough mechanism. Patients must make adjustments during the shift from inspiration to expiration during MI-E, therefore pharyngeal function should be maintained. In a study of laryngeal responses in MI-E among healthy volunteers, it was noted that some people reported laryngeal obstruction at negative pressure.23 This may be because the timing of MI-E and coughing do not match. Regarding the comparison of the CPF values of a pneumotachograph and peak flow meter, the peak flow meter has been shown to have a higher or lower value, and a consensus has not yet been reached.18,24
The operating principle of the peak flow meter is the measurement of CPF at the position indicated when the piston held by the spring moves according to the expiratory flow rate. In the automatic spirometer, the measurement is derived using the volume calculated from the flow measured using a hot wire-type flow meter. It is thought that the measurement value is influenced by differences in the sensitivities of the measurement approaches. In previous studies, a pneumotachograph was considered more sensitive, and a previous study reported that it is accurate for subjects with cough deterioration.24 The findings of this study support the latter results, with the CPF measured with the automatic spirometer being the most accurate.
The present study has some limitations. First, the set pressure of MI-E was 40 cm H2O, which was used in preliminary research and is a common setting. However, the optimal pressure of MI-E should be determined according to the condition of the patient. Additional research on the optimal inspiratory pressure settings for MI-E would be useful. Second, we aimed to compare MI-E and MIC at the same pressure, but there might have been an increase in dead space and air leakage with the connections between the peak flow meter and spirometer, which could lead to some degree of error in our measurements. This error in the peak flow meter measurement was influenced by the method of air entrainment used by the bag-valve-mask. There could also be variations in our results secondary to differences in the performance of the bag-valve-mask procedure.
Conclusion
In this study, among subjects with DMD, there were no statistically significant differences among MI-E–CPF, MIC+assisted CPF, and MI-E+assisted CPF. Using spirometry as the standard, the CPF displayed on the MI-E device has a high reliability. However, there was a negative fixed bias in the CPF of the peak flow meter. Therefore, the peak flow meter may underestimate the true value of CPF.
Footnotes
- Correspondence: Kazuto Kikuchi RPT, Department of Rehabilitation, Akita National Hospital, 84-40 Idonosawa, Iwaki Uchimichikawa, Yurihonjo City, Akita, Japan. E-mail: riha1{at}akitahp.jp.
The authors have disclosed no conflicts of interest.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}