

Abstract
BACKGROUND: There are limited longitudinal studies reporting predictive factors for decline in 6-min walk distance (6MWD) in patients with COPD. While previous studies have confirmed the association between air-flow limitation and decline in 6MWD, other factors have not been clarified. The objective of this study was to investigate whether exercise-induced oxygen desaturation (EID) could be a predictive factor for decline in 6MWD in patients with COPD. The interactive effect of air-flow limitation on the association between EID and decline in 6MWD was also investigated.
METHODS: A longitudinal observational study was conducted with 71 out-patients with COPD who were followed for 1 year. 6MWD, EID, spirometry, and clinical characteristics were assessed. The effect of EID on changes in 6MWD was examined using linear regression analyses. Furthermore, the subjects were categorized into 4 groups according to their EID and air-flow limitation status, and changes in 6MWD were compared among the groups.
RESULTS: 51 subjects completed the follow-up assessments, and 29 (56.9%) experienced EID. Multiple linear regression model revealed that EID was the only predictive factor for changes in 6MWD after adjusting for confounders (β = −38.9, P = .02). As results of multiple comparisons among the 4 groups based on EID and air-flow limitation status, changes in 6MWD in the EID and severe air-flow limitation group were the lowest.
CONCLUSION: Our results revealed that EID was a predictive factor for decline in the functional capacity of subjects with COPD. The assessment of EID and air-flow limitation would thus be useful in estimating the prognosis of decline in the functional capacity of patients with COPD.
- COPD
- peripheral oxygen saturation
- 6-min walk test
- functional capacity
- longitudinal decline
- air-flow limitation
Introduction
Limited functional capacity is the main factor that prevents participation in activities of daily living for patients with COPD.1 The 6-min walk distance (6MWD), the primary outcome of 6-min walk test (6MWT), is the most common tool used to measure the functional capacity of patients with COPD. 6MWD is an important predictive indicator for prognosis independent of some indices of disease severity of COPD, such as air-flow limitation assessed by FEV1 or dyspnea.2–4 6MWD naturally decreases over time for patients with COPD,3–9 and this annual decline in 6MWD also predicts mortality.4,5 Therefore, maintaining functional capacity is an important goal in treating patients with COPD, and clarifying the predictive factors for longitudinal decline in 6MWD is warranted.
There are limited longitudinal studies that have reported predictive factors for decline in 6MWD in patients with COPD. Most studies have reported FEV1 as a primary predictive factor.3,5–8 Casanova et al5 demonstrated that 6MWD decreased only in subjects with severe air-flow limitation (FEV1 < 50% predicted) but not in subjects with mild air-flow limitation (FEV1 ≥ 50% predicted). In addition, previous studies have reported age, sex, weight, hospitalizations, diffusion capacity, and computed tomographic measures of emphysema, hyperinflation, and physical activity as factors associated with decline in 6MWD.3,6–9 However, the results have been inconsistent, and additional studies are needed to investigate factors to accurately predict longitudinal decline in 6MWD in COPD patients.
Patients with COPD frequently experience significant decreases in oxygen saturation during exercise owing to the imbalance between oxygen delivery and exercise-induced demand.10 The 6MWT has also been suggested as the preferred tool to identify exercise-induced oxygen desaturation (EID). Some studies have reported that EID occurred in 20–50% subjects with COPD.10–19 EID negatively affects various organs and is associated with hospitalization and mortality in patients with COPD.13–15,18–20 Nevertheless, the association between EID and decline in 6MWD has not been clarified, especially in longitudinal studies, despite the importance of maintaining functional capacity in COPD patients. We hypothesized that EID would be a factor to cause decline in 6MWD in patients with COPD.
This study aimed to investigate whether EID is associated with longitudinal decline in 6MWD in patients with COPD. Because previous studies have confirmed the association between air-flow limitation and decline in 6MWD,3,5–8 the interactive effect of air-flow limitation on the association between EID and decline in 6MWD was further investigated in our study.
QUICK LOOK
Current Knowledge
Maintaining functional capacity is an important goal in treating patients with COPD; therefore, clarifying predictive factors for longitudinal decline in 6-min walk distance (6MWD) is warranted. Some studies have reported air-flow limitation assessed by FEV1 as a primary predictive factor. There are limited longitudinal studies that have reported other predictive factors for decline in 6MWD.
What this paper contributes to our knowledge
Subjects with COPD who experienced exercise-induced oxygen desaturation (EID) tended to have a decline in 6MWD after 1 y, but this did not change in subjects without EID. In particular, subjects with EID combined with severe air-flow limitation had the largest decline in 6MWD. The assessment of EID and air-flow limitation would be useful in estimating the prognosis of decline in the functional capacity of patients with COPD.
Methods
Subjects
A longitudinal observational study was conducted in out-patients with COPD who were followed for 1 y. Only those patients who completed the baseline assessment between January 2013 and December 2014 were enrolled in the study. The following inclusion criteria were used to clinically define COPD: presence of symptoms, including cough, sputum production, wheezing, and dyspnea; smoking history (20 pack-years); existence of emphysema on chest computed tomography; and a physician diagnosis of COPD.21–23 The exclusion criteria were history of lung surgical procedures, comorbidity of other lung diseases (eg, interstitial lung disease, lung tuberculosis, pneumoconiosis, or lung cancer), exacerbation-related hospitalization 3 months before baseline assessment, and neuromuscular conditions that would interfere with 6MWT. This study was approved by the ethics committee of Kobe University (N287). All subjects provided written or verbal informed consent according to the ethical standards set forth in the declaration of Helsinki.
6MWT
The 6MWT was performed according to American Thoracic Society guidelines at baseline and after a 1-y follow-up.24 The test was performed once each time; a practice test was not conducted. The test was supervised by a trained physical therapist at Kobe City Hospital Organization, Kobe City Medical Center, West Hospital, in a location where a rapid, appropriate response to an emergency was possible. No adverse events occurred during the test. The subjects were allowed to stop and rest during the test but were instructed to resume walking as soon as they felt able to do so. The total distance walked was recorded as 6MWD, and this was used as the primary outcome measure of functional capacity. The modified Borg scale was used to record symptom scores for dyspnea during the test. Peripheral oxygen saturation (SpO2) and heart rate during 6MWT were continuously recorded using a pulse oximeter (WristOx 3150; Nonin Medical, Plymouth, Minnesota) with a finger probe and analysis software (WristOx 2; Star Product, Tokyo, Japan). EID was defined as a nadir SpO2 level of < 90% or ΔSpO2 level of ≥ 4%.12,15
Clinical Characteristics
A chest physician performed a physical examination at baseline assessment. Demographic information was collected, including body weight, height, medical history, inhaled drugs, and use of long-term oxygen therapy. Dyspnea was measured using the modified Medical Research Council (mMRC) dyspnea scale. The COPD Assessment Test was used to assess the disease-specific quality of life. Post-bronchodilator spirometry was conducted using an Autospirometer System 21 (Minato Medical Science, Osaka, Japan). The following values were obtained: FEV1, FVC, and FEV1/FVC ratio. Diffusing lung capacity was also measured as diffusion lung capacity for carbon monoxide (DLCO) by assessing single-breath carbon monoxide uptake. Based on FEV1 values, predicted values of mild and severe air-flow limitation were defined as ≥ 50% (Global Initiative for Chronic Obstructive Lung Disease; GOLD 1 or 2) and < 50% (GOLD 3 or 4), respectively.
Statistical Analysis
All statistical analyses were performed using a commercially available software (JMP9.0 J; SAS Institute Japan, Tokyo, Japan). Data are presented as mean ± SD or proportion (%), as appropriate. Using independent t tests or chi-square tests, subject characteristics and 6MWD at baseline and other measures of 6MWT were compared. To assess the effect of EID or air-flow limitation on changes in 6MWD over time, repeated measures 2-way analyses of variance (ANOVA) were performed. Furthermore, the value of longitudinal changes in 6MWD was calculated for > 1 y, and linear regression analyses were performed to explore the independent predictive factors for changes in 6MWD. Single linear regressions were performed for the unadjusted model using longitudinal changes in 6MWD as a dependent variable and EID and potential confounders, which were considered theoretically related to outcome (age, sex, body mass index, smoking history, mMRC, COPD Assessment Test score, exacerbations during follow-up, FEV1, FVC, and DLCO), as independent variables. Then a multiple linear regression was performed for the adjusted model using longitudinal changes in 6MWD as a dependent variable and EID as an independent variable. Sex and age were mandatorily included in the model. Covariates associated with decline in 6MWD (P < .20) were also included. In addition, the subjects were categorized into 4 groups based on EID and air-flow limitation status (ie, no EID and mild air-flow limitation, no EID and severe air-flow limitation, EID and mild air-flow limitation, and EID and severe air-flow limitation groups). The linear trend of longitudinal changes in 6MWD across the groups was determined using a Jonckheere-Terpstra trend test. The level of significance for all analyses was set at P < .05.
Results
A flow chart of subjects from baseline to follow-up is shown in Figure 1. Of the 71 out-patients with COPD who completed baseline assessments and were included in this study, 51 (71.8%) were able to perform 6MWT at follow-up. The mean follow-up period was 365 ± 30 d. Twenty subjects had missing data on 6MWD after 1 y and were lost to follow-up. No subjects died during the follow-up period. Ten subjects experienced one or more exacerbations.
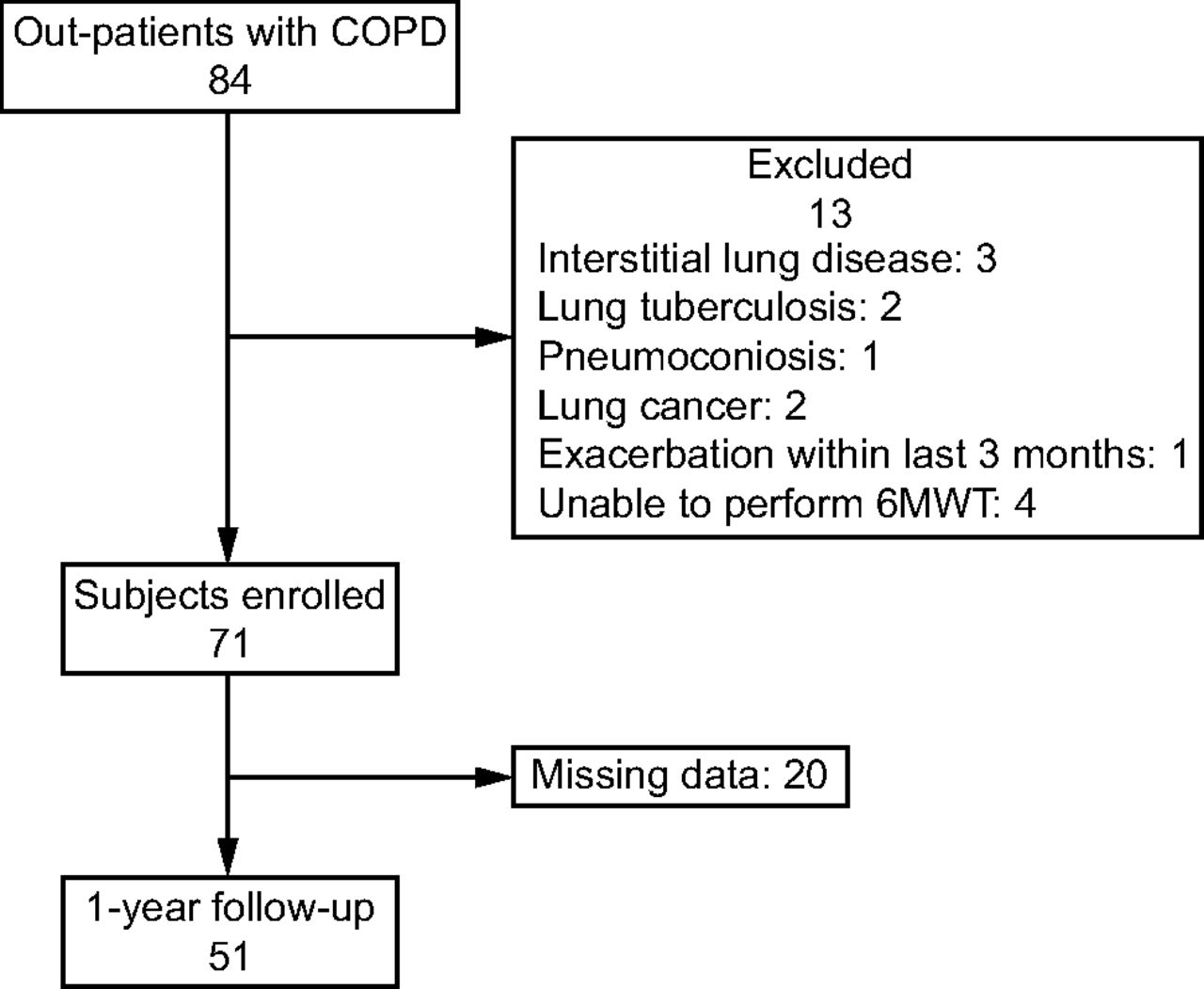
Flow chart. 6MWT = 6-min walk test.
Baseline characteristics of the subjects are summarized in Table 1. Overall, 56.9% of the subjects experienced EID during 6MWT. There were no significant differences in EID status among age, sex, body mass index, and smoking history. Subjects with EID were more likely to report higher frequency of dyspnea on the mMRC scale than those without EID (P = .01). Furthermore, they had poor quality of life according to the COPD Assessment Test score (P = .052). All subjects used some type of inhaled medication (long-acting muscarinic antagonist, Long-acting β2 agonist, or inhaled corticosteroid), and there were no significant differences in type of medication used based on EID occurrence. Subjects with EID had significantly lower pulmonary function, including FEV1 and FVC (P = .005, P = .032, respectively). More subjects with EID had severe air-flow limitation than those without EID (P = .02). When comparing 6MWT measures among the groups, no differences were found between the EID and no EID groups in 6MWD (EID group, 400 ± 130 m vs no EID group, 440 ± 81 m), highest heart rate, and dyspnea at baseline and during the test.
Baseline Characteristics and 6MWT Measures in Patients With COPD Based on EID Status
Effect of EID and Air-Flow Limitation on Longitudinal Decline in 6MWD
The mean ± SD of longitudinal changes in 6MWD over 1 y was −19 ± 55 m. Repeated measures 2-way ANOVA revealed a significant interaction between decline in 6MWD and EID (F = 8.7, P = .005) (Fig. 2A). The EID group exhibited a significant decline in 6MWD (mean change:−38 ± 50 m), whereas the no EID group did not. A significant interaction was also found between decline in 6MWD and air-flow limitation status (F = 4.1, P = .047) (Fig. 2B). The severe air-flow limitation group exhibited a significant decline in 6MWD (mean change: −39 ± 56 m), whereas the mild air-flow limitation group did not.

Changes in 6-min walk distance (6MWD) from baseline to 1-y follow-up based on (A) EID and (B) severity of air-flow limitation. 6MWD = 6-min walk distance; EID = exercise-induced desaturation.
The unadjusted linear regression analysis demonstrated that EID and FVC were significantly associated with longitudinal changes in 6MWD (P = .005, P = .02, respectively). FEV1 tended to be associated with longitudinal changes in 6MWD (P = .10). In the adjusted analysis, EID, FEV1, FVC, sex, and age were included in the multiple linear regression model as dependent variables, and EID was the only predictive factor for decline in 6MWD (β = −38.9, P = .02) (Table 2).
Linear Regression Models to Predict Longitudinal Changes in 6MWD Over 1 Y
Comparison of Longitudinal Changes in 6MWD Within the 4 Groups Based on EID and Air-Flow Limitation Status
Based on EID and air-flow limitation status, 18 subjects (35.3%) were categorized into the no EID and mild air-flow limitation group, 4 subjects (7.8%) into the no EID and severe air-flow limitation group, 14 subjects (27.5%) into the EID and mild air-flow limitation group, and 15 subjects (29.4%) into EID and severe air-flow limitation group. Longitudinal changes in 6MWD showed a significant linear trend across the groups using the Jonckheere-Terpstra trend test (P = .007). Changes in 6MWD in EID and severe air-flow limitation group (mean change:−50 ± 49 m) was the lowest (Fig. 3).

Changes in 6MWD from baseline to 1-y follow-up between the groups based on EID and air-flow limitation status. The linear trend across the groups was determined using the Jonckheere-Terpstra trend test, P = .007. 6MWD = 6-min walk distance; EID = exercise-induced desaturation.
Discussion
This longitudinal study revealed that subjects with COPD who experienced EID during 6MWT had a significant decline in 6MWD after a 1-y follow-up, but 6MWD did not change in subjects without EID. EID was the significant predictive factor for decline in 6MWD after adjusting for potential confounders, including age, sex, FEV1, air-flow limitation, and FVC. In addition, our results indicated that subjects with EID combined with severe air-flow limitation had the largest decline in 6MWD.
The mean decline in 6MWD in subjects with COPD after the 1-y follow-up was 19 m, which increased to 38 m, particularly in subjects with EID. Some studies have demonstrated that 6MWD in subjects with COPD naturally decreases over time, with an annual decline reported as 2–40 m,3–9 which was comparable to that of our study. The larger decline in 6MWD was related to unfavorable outcomes,3,4 and the minimum clinical important difference for 6MWD was proposed as > 30 m.25,26 Polkey et al27 demonstrated that when the decline in 6MWD exceeded the minimum clinical important difference (ie, 30 m), the subject had an increased risk for mortality. Decline in 6MWD in subjects with EID exceeded the minimum clinical important difference, which suggested that EID had a high impact on the functional capacity of subjects with COPD.
To our knowledge, this is the first study to report that EID is a significant predictive factor for decline in 6MWD. Importantly, a longitudinal association was observed even after adjustment for air-flow limitation, a confirmed predictive factor, and for other potential confounders. Several studies have demonstrated that EID is associated with a longitudinal decline in lung function, lean body mass, and quality of life.12,15 Furthermore, subjects with COPD experiencing EID had increased risk of exacerbation and mortality.13–15,18,19 Waatevik et al15 studied 370 subjects with COPD for 3 y and found that those with EID had an approximately 2-fold increased risk of mortality and a 50% increased risk for experiencing future exacerbations. Due to the importance of functional capacity in patients with COPD, our results support and confirm EID as a noteworthy symptom in COPD. A recent large randomized control trial demonstrated that long-term treatment with supplemental oxygen did not provide any benefit with respect to the time to death or first hospitalization or any sustained benefit among subjects with COPD experiencing moderate EID.28 These patients may require intervention to enhance their functional capacity.
There are several explanations for the association between EID and decline in functional capacity. First, dyspnea evoked by EID might cause limited physical activity and deconditioning. Hypoxemia is one of the contributing factors for dyspnea, which is caused by stimulating chemoreceptors in the carotid and aortic bodies.29 In our study, subjects with EID complained of more severe dyspnea than those without EID. Dyspnea, which is a sensation of breathlessness, is a major reason for limited physical activity in patients with COPD and leads to a decline in physical and cardiopulmonary function.1 Second, the negative effects of chronic hypoxemia might cause a decline in functional capacity. Subjects who experienced EID during 6MWT were also shown to experience these symptoms in activities of daily living, both during physical activity and sleep.30,31 Chronic hypoxemia induces pulmonary hypertension, polycythemia, systemic inflammation, and skeletal muscle dysfunction,20 and these adverse sequelae in various organs are correlated with functional capacity. However, these statuses (eg, physical activity, pulmonary arterial pressure, or muscle function) were not assessed, and further studies are warranted to clarify these relationships.
We also found that the decline in 6MWD was greatest in subjects with EID combined with severe air-flow limitation (mean annual decline: 50 m). Another new finding of our study is that the combined assessment of air-flow limitation and EID enabled a more sensitive prediction for declines in the functional capacity of subjects with COPD compared with the assessment of only air-flow limitation. Our results were consistent with those of previous studies in which 6MWD decreased in subjects with severe air-flow limitation but not in patients with mild air-flow limitation.3,5–7 In addition, our results indicated that EID predicted decline independent of the severity of air-flow limitation and that EID had an interactive effect with air-flow limitation on the decline in functional capacity. Causes of EID are multifactorial, such as ventilation–perfusion mismatching, diffusion-type limitation, shunting, and a reduced oxygen content of mixed venous blood, all contributing to EID to some extent.32 EID in COPD is associated with not only severe air-flow limitation but also other symptoms, such as decreasing diffusing capacity, greater emphysema, dynamic hyperinflation, pulmonary artery enlargement, poorer muscle strength, and impaired daily physical activity.11,12,16,17,33 Therefore, the assessment of EID would represent different aspects of disease severity of COPD apart from air-flow limitation. This assessment is noninvasive and easily practiced, and it might be a more informative and appropriate method when combined with the assessment of air-flow limitation during the first screening of disease severity in patients with COPD.
This study has some limitations. First, the number of subjects was inadequate to generalize our results. Second, important factors previously demonstrated to be associated with a decline in 6MWD, such as physical activity, lower limb strength, hyperinflation, and computed tomographic measures of emphysema, were unaccounted for because data regarding these factors were not collected at baseline.6–8 This also limits the generalizability of the results. Future studies with a larger sample size investigating these factors associated with decline in 6MWD, including potential confounding factors, are needed. Third, the 6MWT was performed only once on each occasion in this study, although the American Thoracic Society guidelines recommend 2 tests.24 As the learning effect could occur in measuring 6MWD,34 the annual decline might be underestimated with only 1 measurement. Nevertheless, subjects with COPD experiencing EID demonstrated a larger decline in their 6MWD; therefore, this finding is considered relevant.
Conclusions
Our results revealed that EID was a predictive factor for decline in the functional capacity of subjects with COPD, particularly EID combined with severe air-flow limitation. The assessment of EID and air-flow limitation would thus be useful in estimating the prognosis of decline in the functional capacity of patients with COPD.
Acknowledgments
The authors thank Ryuichi Sawa, Satoshi Minami, Yuya Ueda, Tatsuro Inoue, Katsuyoshi Tanaka, Ryo Nakamura, Shunsuke Murata, Takashi Saito, Taiki Sugimoto, Tsunenori Isa, Aoi Ebina, Yuki Kondo, Yamato Tsuboi, Kazufumi Kitagaki, Kotaro Tosizawa, and Shoma Fukuta of the Department of Community Health Sciences, Kobe University Graduate School of Health Sciences, for their constructive comments on the design of this study and interpretation of the data analysis.
Footnotes
- Correspondence: Shogo Misu, Department of Physical Therapy, Faculty of Nursing and Rehabilitation, Konan Women's University, 6-2-13, Morikita-machi, Higashinada-ku, Kobe 658-0001 Hyogo, Japan. E-mail: s-misu{at}konan-wu.ac.jp.
Mr Misu presented a version of this paper at the 29th Congress of Hyogo Society of Physical Therapy, July 9, 2017, in Kobe, Japan.
The authors disclose no conflicts of interest.
- Copyright © 2019 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}