

Abstract
BACKGROUND: Single-step tests have been proposed as simple and inexpensive challenges to diagnose exercise-induced bronchoconstriction (EIB) in the pediatric population. Work performed and the resulting ventilation, however, might be substantially lower in stepping than running. This might decrease the diagnostic yield of step-based challenges.
METHODS: In a cross-sectional study, 53 children with asthma with exercise-related symptoms (34 boys, age 6–18 y) underwent an incremental stepping test, a 6-min constant stepping test, and a treadmill running test on different days.
RESULTS: Constant and incremental stepping tests presented with lower metabolic demands (V̇O2 1.42 ± 0.48 and 1.34 ± 0.55 L/min, respectively), ventilatory demands (V̇O2 45 ± 14 and 43 ± 16 L/min, respectively), and cardiovascular demands (160 ± 20 and 161 ± 19 beats/min, respectively) than the treadmill running test (1.65 ± 0.60 L/min, 54 ± 17 L/min, and 172 ± 7 beats/min, respectively) (P < .05). Between-test agreement in diagnosing EIB was poor (kappa 0.217–0.361). Although EIB prevalence was higher after the treadmill running test (60%) compared to constant (53%) and incremental (47%) stepping tests, 7 subjects developed EIB only in stepping. Clinical and resting functional characteristics did not differ in discordant subjects (ie, EIB negative in a given test but positive in another) versus concordant subjects (ie, EIB negative or positive in both tests). EIB was not related to individual test ability in eliciting high to very-high ventilation (≥ 40% or ≥ 60% maximum voluntary ventilation, respectively). Moreover, a negative stepping test but a positive treadmill test (and vice versa) was not associated with greater ventilatory demands.
CONCLUSIONS: Lower prevalence of EIB in stepping compared to treadmill running is not related to less ventilation demand in the former modality. Although stepping might be useful as a screening EIB test due its portability and low cost, a negative test should be confirmed with a running-based test in symptomatic children.
Introduction
Exercise is a common and potent trigger of asthmatic symptoms in children.1 Exercise-induced bronchoconstriction (EIB) is a marker of inadequate disease control, and it is associated with poor quality of life and increased utilization of health care resources.2 EIB worldwide prevalence in children and adolescents with asthma is 46%3 Unfortunately, reported symptoms are imprecise to diagnose EIB, particularly in children.4,5 Thus, several exercise challenge tests have been proposed to dehydrate and cool down the airways, thereby eliciting EIB in susceptible individuals.1,2,6 Regardless of the type of exercise, it must be intense enough to achieve 80–90% predicted maximum heart rate, or ventilation corresponding to 17.5–21 times FEV1.4
Weight-bearing exercise is associated with greater ventilatory demand than weight-supported exercise.7 Assuming a critical role for high ventilation in increasing post-exercise bronchial hyper-responsiveness,1,2,6–11 these findings might explain the higher prevalence of EIB after a treadmill test compared to a cycling test.7,12 Laboratory-based tests, however, are not widely available and often require bulky and expensive ergometers. Treadmill tests, in particular, raise additional concerns about children's safety and their ability to exercise steadily at high speeds.13 Single-step tests are externally valid and a portable alternative to ergometer-based tests,14–16 but the metabolic demands associated with stepping might be considerably lower than those associated with running.17 Moreover, the vertical work associated with stepping places a greater burden on lower limb muscles.18,19 Thus, a stepping test in children may be limited by leg fatigue before they have reached the high levels of ventilation thought necessary to provoke EIB.20,21 It is therefore conceivable that by failing to elicit sufficiently high ventilation, stepping tests might be less sensitive than treadmill tests in detecting EIB. This hypothesis, however, has not been tested in children with asthma.
We prospectively compared the prevalence and severity of EIB in response to stepping and treadmill running as modulated by potential inter-modality differences in ventilation in children with asthma with exercise-related symptoms. To investigate whether sudden versus progressive increases in ventilation would also influence a stepping test's ability to detect EIB,22 subjects underwent constant work load and incremental stepping tests. We hypothesized that stepping would induce less EIB due to lower ventilatory requirements compared to running. Moreover, we anticipated that a delay in reaching high levels of ventilation would further reduce the diagnostic yield of the incremental compared to the constant stepping test.
QUICK LOOK
Current knowledge
Laboratory-based tests are commonly used to evaluate exercise-induced bronchoconstriction (EIB), but are not widely available, and require bulky and expensive ergometers. Single-step tests are an externally validated and portable alternative to ergometer-based tests.
What this paper contributes to our knowledge
Constant and incremental stepping tests were roughly equivalent in determining EIB, but both protocols exhibited lower metabolic, ventilatory, and cardiovascular demands than treadmill running. Despite higher EIB prevalence after running, some subjects with a negative treadmill test had a positive stepping test. In such cases, a single-step test might be useful to screen for EIB.
Methods
This was a prospective, cross-sectional study. Subjects' parents or legal guardians signed informed consent, and children gave their assent to participate in the study, which was approved by the institutional Research Ethics Board (Ethics Committee of the University Nove de Julho, São Paulo, Brazil).
Study Design, Participants, and Measurements
Fifity-three children and adolescents (34 boys, age 12 ± 3 y) with a diagnosis of asthma and a history of exercise-induced respiratory symptoms followed in the asthma out-patient clinic at the Pediatrics Department of São Paulo School of Medicine, Federal University of São Paulo, Brazil, comprised the study group. Patients were excluded for recent disease exacerbation (within the preceding 6 weeks) as stated in the medical record. Smoking, severe asthma (Global Initiative for Asthma23 step 5), presence of other chronic lung diseases, and relevant systemic comorbidities (eg, heart disease, diabetes, and musculoskeletal diseases) were also exclusion factors. Subjects' parents (or legal guardians) were instructed to discontinue short- and long-acting β2 agonists and oral leukotriene receptor antagonist administration within the timeframe defined by current guidelines.1,2,6,20,21 Inhaled steroids were discontinued 24 h before testing. Subjects were instructed to avoid exercise, heavy meals, and coffee, tea, or soft drinks within this timeframe.1,2,6,20,21
Spirometry
Standard spirometric tests (CPX Ultima, Medical Graphics, St. Paul, Minnesota) were performed in the seated position according to the American Thoracic Society/European Respiratory Society criteria.24 The Global Lung Function Initiative scale was used to classify spirometric values; z scores > −1.64 were considered normal, z scores from −1.64 to −2.5 were considered mild obstruction, z scores from −2.5 to −3.5 were considered moderate obstruction, and z scores < −3.5 were considered severe obstruction.25 Volumes and flows were measured before the challenges and at 5, 10, 15, 20, and 30 min after the challenges. A FEV1 decrease (nadir) ≥ 10% from pre-exercise values defined a positive EIB test.1,2,6 EIB was classified as mild (10–15% FEV1 decrease), moderate (16–25% decrease), or severe EIB (> 25% decrease).2 The area under the FEV1 curve (AUC), which provided an additional index of EIB severity, was calculated as the integral of the FEV1 response (% from pre-exercise) from 5 min to 30 min post-challenge (SigmaPlot, version 12.0, Systat Software, San Jose, California).
Exercise Challenges Testing
Exercise challenge tests were carried out at least 72 h apart in a randomized sequence. Tests were performed at room temperature between 19°C and 24°C and relative humidity of 60 ± 3%. Standard variables including metabolic demand (oxygen consumption (V̇O2, L/min), carbon dioxide output (V̇CO2, L/min), ventilatory (minute ventilation (V̇E, L/min), cardiovascular demand (heart rate, beats/min), gas exchange (SpO2, %) were recorded throughout the tests. Subjects were asked to rate dyspnea and leg fatigue at exercise cessation by using the 0–10 Borg scale. An index of ventilatory demand relative to maximum capacity was established by the V̇E at the peak of exercise divided by maximum voluntary ventilation (MVV) multiplied by 100. MVV was calculated as pre-exercise FEV1 × 40. V̇E/MVV values ≥ 40% and ≥ 60% indicated high and very-high ventilatory demands, respectively.1,2,6 The V̇E/MVV AUC was calculated to provide a more precise index of ventilatory stress. It was separately calculated as the integral over exercise time under total ventilation, high ventilation, and very-high ventilation (SigmaPlot, version 12.0).
Treadmill Test
The treadmill test (Millenium Classic, Inbrasport, Porto Alegre, Brazil) was performed as proposed by Carlsen et al26 at a 5.5% grade with speed adjusted within the initial 3 min to reach 80–90% maximum predicted heart rate, which was then maintained for 4–6 min.
Stepping Tests
The single-step tests were performed using a step 15 cm high for subjects up to 1.40 m and a step 20 cm high for taller subjects (> 1.40 m high).15,27 The arms were kept unsupported. The standardized instructions recommended by the American Thoracic Society for the 6-min walking test were provided prior to the constant stepping test.28 Briefly, subjects were instructed to step up and down at their own cadence during this timeframe. Subjects were allowed to stop at their will and resume exercise regardless of the elapsed time. The same encouragement phrases were provided every minute in an even tone.28 During the incremental stepping test, stepping cadence was made faster in response to an external sound stimuli as established by Sykes29 and modified by Dal Corso et al,30 starting at 10 steps/min, with the stepping rate increased 2 steps/min every 30 s up to symptom limitation or inability to maintain the required stepping rate for 15 s.30 Objective and subjective criteria for test interruption were the same as those recommended by the American Heart Association for the pediatric population.31
Statistical Analysis
The sample size was calculated to detect a treadmill-step difference in FEV1 % fall > 3.3% with a SD of 5.9%16 assuming a α error of 5% and a β error of 20%. These criteria yielded a sample size of 48 subjects. To account for potential dropouts, we assessed 53 children. According to data distribution, measures of central tendency and dispersion were mean ± SD or median (interquartile range). Between-group comparisons over time were performed with repeated measurements of analysis of variance (ANOVA). Chi-square tests examined potential differences in proportions. The level of between-test agreement in eliciting EIB was tested by Cohen's kappa (≤ 0 indicating no agreement, 0.01–0.20 as none to slight, 0.21–0.40 as poor, 0.41–0.60 as moderate, 0.61–0.80 as substantial, and 0.81–1.00 as almost perfect agreement). The Bland-Altman test examined between-test differences in EIB severity as a function of their means. The Pearson correlation coefficient was used to test the presence of linear association between continuous variables. A 2-sided P value < .05 was considered statistically significant.
Results
Sixty-three patients were screened for study participation. Ten patients were excluded (2 due to recent exacerbation, 6 due to lack of disease control as indicated by the accompanying physician, and 2 due to lack of understanding of study procedures). Thus, 53 subjects were enrolled (Table 1).
Subject Characteristics
Baseline spirometry indicated the presence of air flow obstruction in 15 subjects (8 mild, 6 moderate, 1 severe) with the remaining tests within the limits of normal. Pre-challenge spirometric values did not differ among tests. Prechallenge spirometric values did not differ among tests (Table 2).
Pre Challenge Spirometric Values
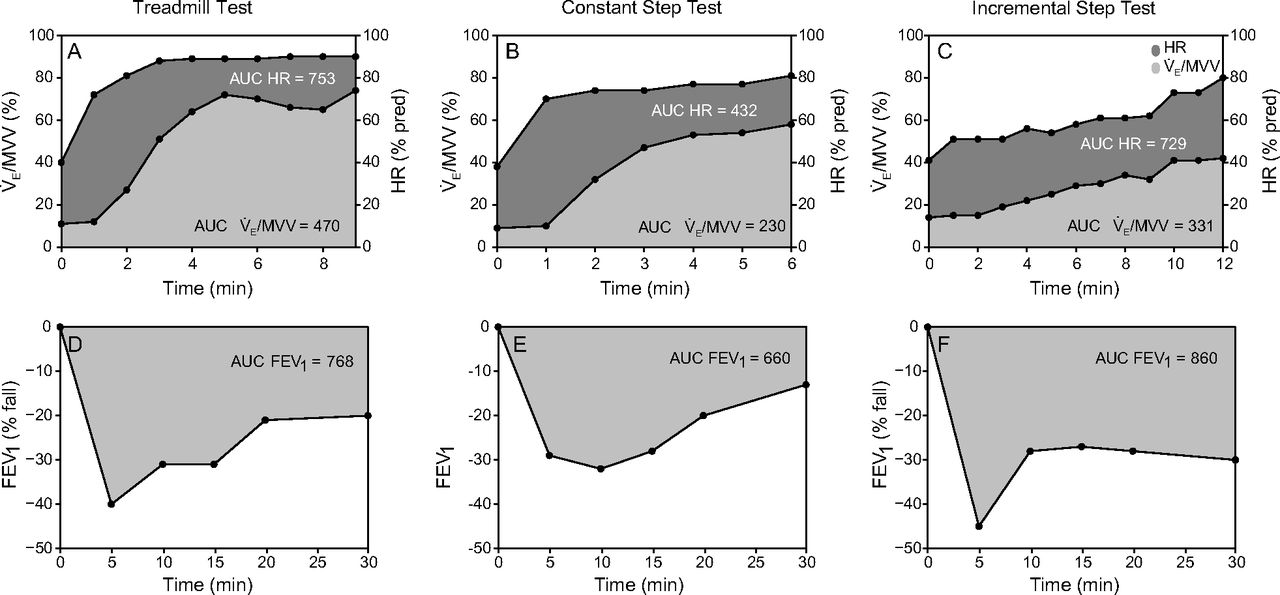
All subjects successfully completed all proposed tests without complications. To reach the target heart rate (80–90% predicted),26 subjects ran during the treadmill tests (7 ± 1 km/h). As expected by the test's design, the constant stepping test was shorter than the treadmill test, whereas the incremental stepping test was longer than the treadmill test (Table 3). The total number of steps performed in the constant stepping test was lower than that in the incremental stepping test (180 ± 24 steps and 292 ± 86 steps, respectively). Stepping was associated with lower metabolic, ventilatory, and cardiovascular demand than treadmill running (Fig. 1 for a representative subject). In fact, a greater fraction of subjects reached high (40–60% V̇E/MVV) and very high (60% V̇E/MVV) ventilatory demand during the latter test. The oxygen saturation peak was lower in the treadmill test than in the stepping tests. In contrast, end-exercise symptoms did not differ (Table 3).
Responses to Running (Treadmill Test) and Stepping (Constant and Incremental Tests) in Asthmatic Children

Representative ventilatory and cardiovascular responses during different exercise challenges in a subject with positive exercise-induced bronchoconstriction (A–C). Panels D–F depict the resulting post-exercise decreases in FEV1. V̇E = minute ventilation, MVV = maximum voluntary ventilation, AUC = area under the curve, HR = heart rate.
Forty-five subjects (85%) presented with EIB in at least one challenge. Although EIB prevalence was higher after the treadmill test (60%) compared to the constant and incremental stepping tests (53% and 47%, respectively), between-test agreement in diagnosing EIB was poor (Cohen's kappa values were 0.217–0.361) (Table 4). As shown Supplemental Figure 1, and E-Table 1, there were no significant between-test differences in EIB severity. There were no significant clinical and resting functional differences in subjects with EIB negative in a given test but positive in another versus concordant subjects (ie, EIB negative or positive in both tests) (see the supplementary materials at http://www.rcjournal.com).
Between-Test Agreement for the Diagnosis of EIB in Asthmatic Children
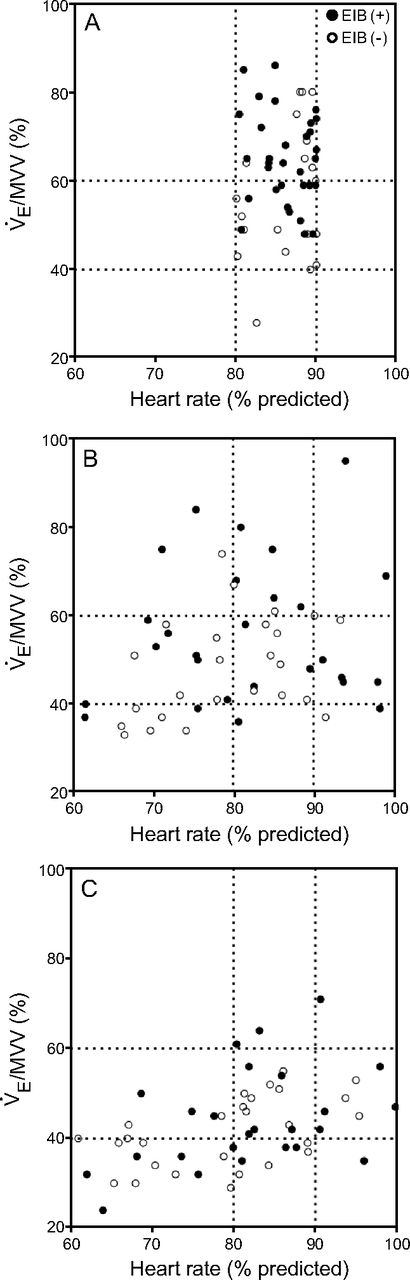
Figure 2 shows that the presence of EIB was largely independent of the ventilatory demand reached in each of the challenges. For instance, a similar fraction of subjects presented with EIB regardless of high or very-high ventilatory demands attained (24% and 37%, respectively) during the treadmill test (Fig. 2A). Similarly, subjects presented with EIB despite test failure in eliciting very-high ventilatory demands (constant stepping test) or even high ventilatory demands (incremental stepping test) (see Figs. 2B and 2C, respectively). Using heart rate as a surrogate of exercise intensity produced similar results.
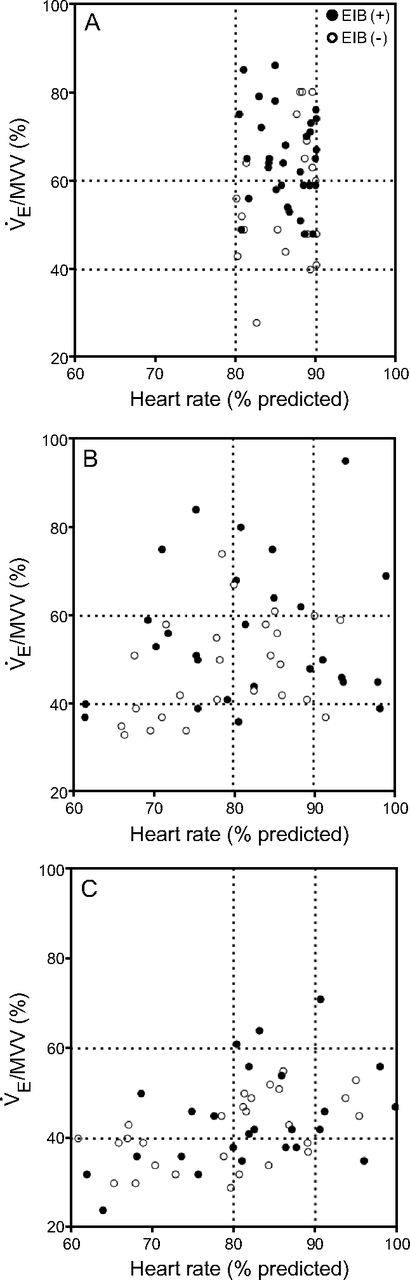
Ventilatory and cardiovascular demand in response to different exercise challenges in subjects who presented with (+) or without (−) EIB. (A) Treadmill test. (B) Constant step test. (C) Incremental step test. V̇E = minute ventilation, MVV = maximum voluntary ventilation, EIB = exercise-induced bronchoconstriction.
Discussion
Our aim was to compare the prevalence and severity of EIB in response to stepping tests and treadmill running tests as modulated by potential inter-modality differences in ventilation in asthmatic children. We hypothesized that stepping would induce less EIB due to lower ventilatory requirements compared to running.
This study contrasted the ventilatory demand elicited by single-step (constant stepping and incremental stepping) and treadmill running challenges as related to their diagnostic yields for EIB in children with asthma and exercise-related symptoms. We found poor between-test agreement in diagnosing EIB. Thus, despite higher EIB prevalence after running, some subjects with a negative treadmill test had a positive stepping test. In line with our main hypothesis, stepping was associated with lower ventilatory demands than running. Contrary to our hypothesis, however, EIB prevalence and severity were largely independent of between-test differences in ventilatory demand. Moreover, the rate of increase in ventilation (ie, faster in constant stepping compared to incremental stepping) did not influence test outcome. Our findings therefore indicate that the ability to elicit high (≥ 40% MVV) or very-high (≥60% MVV) ventilation is not a key requirement for an effective EIB challenge in children with asthma with a high pre-test likelihood of abnormality. Although a stepping test (either constant or incremental) can be used to screen for EIB, a negative challenge should be confirmed with a high-intensity treadmill test. Single-step tests have long been advocated as a portable, inexpensive, and reproducible field exercise testing modality for patients with chronic lung diseases.30,32,33
In this study, we showed that stepping is associated with less ventilatory stress than treadmill running in children with asthma. A substantial fraction of subjects did not reach the ideal ventilatory stress recommended by current guidelines in response to stepping (Fig. 2).1,2,6 These findings could explain the lower prevalence of EIB that we observed (Table 4). Contrary to our expectations, we were unable to find supporting evidence that lower ventilatory stress during stepping hampered test sensitivity in detecting EIB. Thus, our results indicate that reaching high to very-high ventilatory demands is not required to elicit EIB in highly susceptible patients, that is, in children with asthma with a history of exercise-related symptoms. Due to the large day-to-day variability in EIB, repeating the challenge might be more relevant to improve diagnostic yield than increasing testing intensity.34
Nevertheless, failure to reach such high targets might be critical for children with lower pre-test probability of EIB, such as non-asthmatic children without exercise-related symptoms. Due to the lack of differences in environmental conditions and ventilatory demands in patients who developed EIB only after treadmill, alternative explanations should be sought to explain the higher sensitivity of running to elicit EIB. Interestingly, seminal studies presented evidence that the asthmogenic properties of running were not a mere consequence of a higher ventilation load.11,12,35 In this context, oral breathing is greater in running compared to walking,36 so it is possible that the former is associated with less air humidification.37 Release of mediators by the distal (small) airways is mechanistically linked to EIB.20
Differences in breathing pattern and ventilation distribution might expose a larger fraction of the small airways to drier inspired air during running. Moreover, higher cardiac output and greater bronchial blood flow during running might increase local availability of bronchoconstrictive mediators.38 Regardless of the precise mechanisms, our data indicate that the superiority of running compared to stepping in eliciting EIB is not simply consequence of high ventilatory demands inherent to upright, weight-bearing exercise. From a practical perspective, our results demonstrate that treadmill and stepping tests are not interchangeable as exercise challenges for EIB. Specifically, a negative stepping test should be confirmed with a high-intensity treadmill test, particularly in a patient with a high pre-test likelihood of abnormality. Surprisingly, however, a fraction of our subjects presented with EIB only in response to stepping (Table 4).
We cannot rule out that a negative treadmill test with a positive stepping test merely reflects day-to-day variability in EIB susceptibility.2 In other words, it remains unclear whether these subjects would eventually develop EIB had we repeated the treadmill test.38 Additional studies investigating this specific issue are warranted. It should be recognized specifically that the incremental stepping test adds complexity to a field challenge. Considering that the diagnostic yields of constant and incremental stepping tests were roughly equivalent (Table 4), the former seems to be a clinically more attractive option. Whether shorter tests (eg, 3 min)15 would also prove useful remains to be investigated in this specific sub-population of children with exercise-related symptoms.
This study has some limitations. We did not test our subjects on the treadmill at the same (lower) ventilatory demands reached in the stepping tests. Thus, we cannot elaborate on whether low to moderate ventilatory demands would also be effective in eliciting EIB in this specific test modality. Exercise load in the treadmill test was guided by a physiological outcome (heart rate) that reflects exercise intensity. In contrast, the stepping tests were either self-paced or externally paced. Thus, it could be argued that our study design biased the treadmill test to elicit EIB more frequently.
As discussed, however, our data do not indicate that reaching a high cardiorespiratory stress was critical for EIB in our sample. Under the logical assumption that there is a minimal ventilatory load associated with EIB, prospective studies are necessary to investigate whether such requirements are modulated by exercise modality.
Conclusion
The lower prevalence of EIB in stepping tests compared to treadmill running tests was not related to less ventilatory demand in the former testing modality. Regarding the chosen challenge, testing ability to elicit high or very-high ventilation was not a key feature of an effective EIB test in children with asthma with a history of exercise-related symptoms. Although a single-step test might be useful to screen for EIB, a negative challenge should be confirmed with a running-based test in this patient sub-population.
Acknowledgments
We thank Anderson Jose, Laryssa Souza Leitão, Felipe Elias Moreira, and Mariana Mazucca Reimberg (Postgraduate Program in Rehabilitation Sciences, Universidade Nove de Julho, São Paulo, Brazil) for helping with subject recruitment and evaluations.
Footnotes
- Correspondence: Simone Dal Corso PT PhD, Universidade Nove de Julho, Rua Vergueiro no. 235/249, 2o subsolo, Liberdade, São Paulo, Brazil 01504-050. E-mail: si.dal.corso{at}gmail.com.
Ms Selman presented a version of this manuscript at the 17th Congresso Paulista de Pneumologia e Tisiologia, held November 15-18, 2017, in São Paulo, Brazil.
Ms Selman has disclosed a relationship with the São Paulo Research Foundation. The other authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2019 by Daedalus Enterprises





{kind=link}
{kind=link}