

Abstract
Over the past decade, concepts of control of breathing have increasingly moved from being theoretical concepts to “real world” applied science. The purpose of this review is to examine the basics of control of breathing, discuss the bidirectional relationship between control of breathing and mechanical ventilation, and critically assess the application of this knowledge at the patient's bedside. The principles of control of breathing remain under-represented in the training curriculum of respiratory therapists and pulmonologists, whereas the day-to-day bedside application of the principles of control of breathing continues to suffer from a lack of outcomes-based research in the intensive care unit. In contrast, the bedside application of the principles of control of breathing to ambulatory subjects with sleep-disordered breathing has out-stripped that in critically ill patients. The evolution of newer technologies, faster real-time computing abilities, and miniaturization of ventilator technology can bring the concepts of control of breathing to the bedside and benefit the critically ill patient. However, market forces, lack of scientific data, lack of research funding, and regulatory obstacles need to be surmounted.
- artificial respiration
- mechanical ventilation
- ventilator
- obstructive sleep apnea
- sleep apnea
- servo ventilation
- critical illness
Introduction
Mechanical ventilation in the intensive care unit (ICU) has seen tremendous strides, from mere manual bagging through a tracheostomy tube to sophisticated ventilation with built-in alarms and striking visual displays.1 But, shocking as it may seem, mechanical ventilation in the ICU has yet to fully embrace the core principles of control of breathing. In contrast, the bedside application of the principles of control of breathing to ambulatory subjects with sleep-disordered breathing has out-stripped that in critically ill patients. Therefore, in the ICU arena, for the concepts of control of breathing to fully move from being just theoretical concepts to “real world” applied science at the patient's bedside, much more needs to be done. The overarching goal of this review is to take a small step in that direction. The specific objectives are to examine the basics of control of breathing, discuss the bidirectional relationship between control of breathing and mechanical ventilation, and critically assess the application of this knowledge at the patient's bedside.
Basics of Control of Breathing
The principles of control of breathing remain under-represented in the training curriculum of respiratory therapists, medical students, and even pulmonologists in training. While this may seem inexplicable, this is quite expected in that there is an explosion of knowledge and information in medicine, and there are many items competing for space and time in such curricula. Moreover, imparting theoretical concepts without adequate applied physiology may be an additional hurdle. This would be similar to teaching theoretical physics at a course entitled “Introduction to Engineering.” This part of this review is an attempt to provide the very basics of control of breathing with applied physiological exemplars. An additional goal of these exemplars is to underscore the stark differences of some of the basic assumptions of control of breathing in ambulatory subjects versus critically ill patients receiving mechanical ventilation.
Respiratory system control comprises the sensors, effectors, and the central controller (Fig. 1) that work together to ensure adequate gas exchange—intake of O2 and elimination of CO2, which, in turn, ensures normal pH for appropriate functioning of enzymes and other proteins that maintain cellular function. The central controller resides in the respiratory centers of the brain stem (medulla and pons). The respiratory centers comprise the inspiratory-firing and expiratory-firing neurons that reside in the ventral respiratory group of the ventrolateral brainstem. The ventral respiratory group is a collection of 3 nuclear groups: the Bötzinger complex, nucleus ambiguous, and nucleus retro-ambigualis. The neurons in the ventral respiratory group may be considered the upper motor neurons of the respiratory system and effect respiratory muscle activity by innervating and stimulating the motor neurons in the anterior horns of the spinal cord at various levels: cervical or thoracic for effecting activation of the upper airway, diaphragm, and intercostal muscles. The dorsal respiratory group, which lies in the dorsomedial aspect of the medulla oblongata receives afferent input from the peripheral chemoreceptors and pulmonary sensory inputs through the vagus and glossopharyngeal nerves.

Control of breathing in humans. The central controller resides in the brain stem. The various components and stages of the effector arm (shown on the right) and the sensor arm (shown on the left) constitute a continuous feedback loop, with the end-product being gas exchange. Factors that influence each of these steps in this loops are shown within boxes. V̇E = minute volume. V̇/Q̇ = ventilation/perfusion ratio.
In healthy subjects the respiratory controller ensures adequate blood gas exchange, which remains remarkably stable despite wide variations of ventilation. In contrast, the conventional paradigms of respiratory control may not apply to critically ill patients. In spontaneously breathing individuals the respiratory controller achieves normalization of gas exchange, remains responsive to physiological demands (eg, exercise and speech), and strives to ameliorate dyspnea. In patients receiving mechanical ventilation, however, gas exchange may take lower precedence to prevention of lung injury.
Exemplar 1: Respiratory Controller Versus Preventing Lung Injury
A 24-year-old woman with status asthmaticus is admitted with acute hypercapnic respiratory failure (PaCO2 59 mm Hg, PaO2 88 mm Hg, and pH 7.31 on room air). Following intubation, to prevent barotrauma, her arterial pH is allowed to fall to 7.14, with PaCO2 at 98 mm Hg, while low tidal volumes of 6 mL/kg ideal body weight are administered in a volume-controlled continuous mandatory ventilation (VC-CMV) mode. Large doses of sedatives and analgesics are administered to counter the normal respiratory controller's response of tachypnea (and air hunger), to prevent breath stacking and worsening intrinsic PEEP. Despite heavy sedation, however, the young patient continues to exhibit an intact respiratory controller response of high inspiratory drive, and manifests double-triggering of the ventilator, with plateau pressure exceeding 35 cm H2O. To prevent barotrauma, she is paralyzed with cisatracurium bolus and infusion, and heavy sedation is continued. pH is maintained at 7.25 with intravenous bicarbonate infusion, while the PaCO2 is allowed to climb to 108 mm Hg with a PaO2 of 102 mm Hg, on an FIO2 of 0.40.
While the exemplar may be considered an extreme scenario, the reader should be cognizant that conventional paradigms (normalization of pH, arterial gases, and dyspnea) that govern control of breathing during unassisted breathing are significantly altered by the resetting of ventilation endpoints, administration of intravenous bicarbonate, sedation, analgesics, and even paralytic agents. However, the core principles of control of breathing will come back into play after a period of stabilization, when liberation from mechanical ventilation and initiation of spontaneous breathing is contemplated.
The sensors of the respiratory control system consist of the central and peripheral chemoreceptors and neuro-mechanical afferent inputs. The central chemoreceptors are located near the ventral-lateral surface of the medulla, in contact with the cerebrospinal fluid (CSF). The central chemoreceptors are stimulated by the H+ concentration in the CSF. The CSF concentration of H+ is regulated by PaCO2, local blood flow in the area of the brain, and local metabolism. The blood/brain barrier prevents the H+ from the blood from gaining direct access to the medullary chemorecptors, whereas the blood/brain barrier is permeable to CO2, which diffuses across the blood/brain barrier and combines with H2O to liberate H+ ions, thereby stimulating the central chemoreceptors. Such an indirect means of influence of arterial pH on CSF pH (H+ concentration) has clinical importance.
Exemplar 2: Spurious Ventilator Dependence Due to Exuberant Ventilation
A 64-year-old man with COPD on home oxygen is admitted with acute hypercapnic and hypoxic respiratory failure (PaCO2 79 mm Hg, PaO2 58 mm Hg, and pH 7.21 on room air). His resting arterial blood gases on room air a year before were PaCO2 54 mm Hg, PaO2 58 mm Hg, and pH 7.36. He is obtunded and therefore intubated and placed on VC-CMV. Three days later, while still on VC-CMV, his arterial blood gases are PaCO2 33 mm Hg, and PaO2 112 mm Hg, and pH 7.52, on FIO2 0.30, and he is mildly sedated. The therapist reports that attempts at spontaneous breathing trials (on pressure support of 5 cm H2O and PEEP of 5 cm H2O) have met with long apneas, followed by initiation of apnea ventilation. The therapist deems the patient not ready to wean.
In this exemplar, the chronic elevation of PaCO2 would have prompted compensatory generation of CSF bicarbonate and resetting of CSF pH to normal, despite the elevated PCO2 in the CSF and arterial blood. Subsequently, the aggressive ventilation and iatrogenic respiratory alkalosis would have substantially reduced H+ in the CSF (that already had an excess of bicarbonate anions), resulting in abnormally low ventilatory drive. Such reduced ventilatory drive, combined with sedation-induced lack of wakefulness drive to breathe, would result in central apneas. The occurrence of such central apneas can be misconstrued as ventilator dependence.
The peripheral chemoreceptors are located in the carotid bodies (at the bifurcation of the common carotid artery) and the aortic bodies are in the aortic arch. The carotid bodies are responsive to hypoxemia and become activated starting at a PaO2 less than 100 mm Hg, whereas the aortic bodies respond to reductions in arterial pH, regardless of whether they are of respiratory or metabolic source.
Pulmonary stretch receptors, irritant receptors, and J receptors constitute the neuromechanical input to the respiratory controller. The pulmonary stretch receptors are within the airway smooth-muscle cells and are activated by stretch consequent to lung inflation. Such lung inflation initiates the Hering-Breuer inflation reflex, which prolongs expiratory time and thereby slows respiration. The irritant receptors and the J receptors play a role in lung response to noxious stimuli (cough) and pulmonary edema (rapid shallow breathing), respectively.
The effectors of the respiratory system begin with the upper motor upper neurons that are housed in the dorsal respiratory group in the medulla, and lead on to the lower motor neurons in the anterior horn cells of the spinal cord. These nerve impulses activate the respiratory muscles (upper airway, intercostal, and diaphragm muscle), which, in turn, generate negative intrathoracic pressure. The intrathoracic pressure overcomes the resistive and elastic forces of the respiratory system to achieve effective ventilation. This entire loop that is depicted in Figure 1, responding to a derangement in PaCO2 (stimulus), leading to stimulation of the controller, and resulting in augmented ventilation through the effectors would constitute the integrated response of the respiratory system to CO2.
The response of the respiratory system to changes in PaCO2 or PaO2 during wakefulness have certain characteristic features. During wakefulness, decrements in arterial oxygen saturation would lead to stimulation of the respiratory controller and consequent increments in minute ventilation (Fig. 2). In Figure 2 the increments in minute ventilation, even prior to an oxygen saturation of 90%, may be attributable to oxygen sensing by glomus cells of the peripheral chemoreceptors in the carotid bodies. Similarly, minute ventilation can increase by 2–3 L/min with a 1 mm Hg increase in PaCO2 (Fig. 3). Such a ventilatory response is responsible for maintaining PaCO2 and arterial pH in the desired range for the optimal functioning of the cellular proteins and enzymes. Such a homeostatic response is vital for any organism.
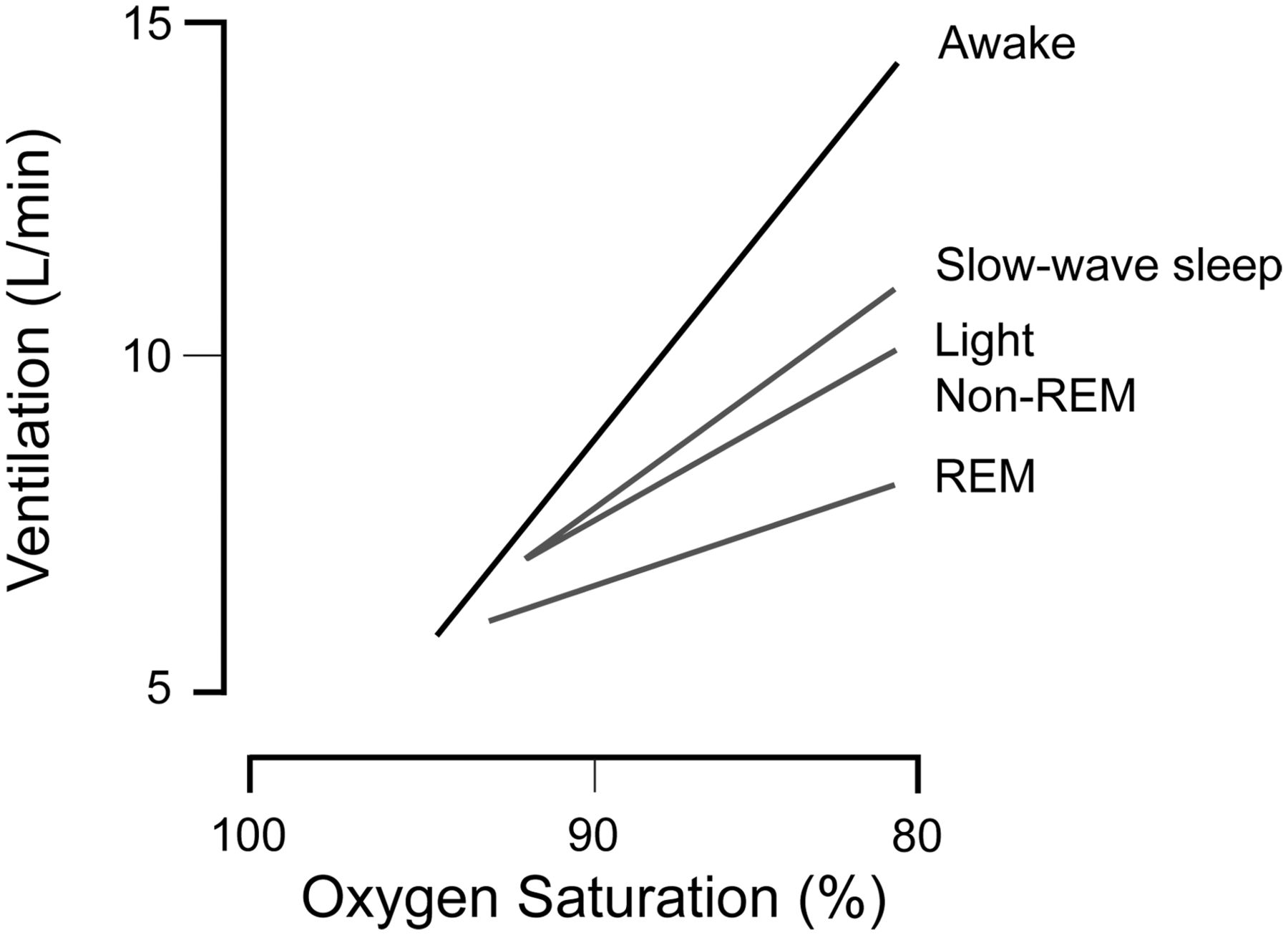
Integrated response of the respiratory controller to changes in hypoxic stimuli, depicted as ventilatory response to changes in oxygen saturation. Change in ventilatory response during wakefulness is depicted by the black line. Changes in ventilatory response during slow-wave sleep, rapid-eye-movement (REM) sleep, and non-REM sleep are depicted by gray lines. Note the rightward shift and slope decrease of the ventilatory response when transitioning from wakefulness to sleep.

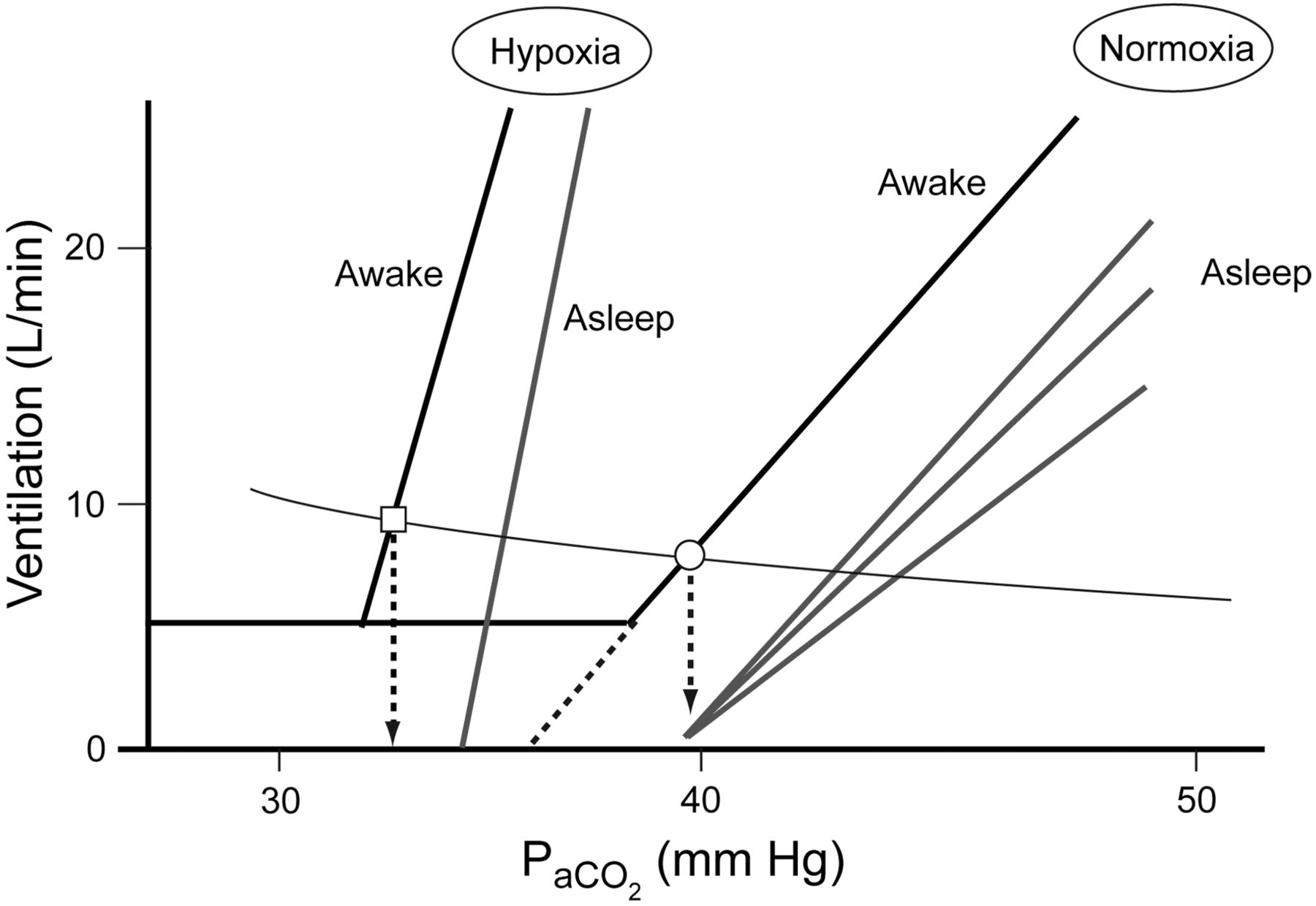
Integrated response of the respiratory controller to changes in hypercapnic stimuli, depicted as ventilatory response to changes in PCO2. Changes in ventilatory response during wakefulness are depicted by black lines. Changes in ventilatory response during various sleep stages are depicted by gray lines. Note the rightward shift and slope decrease of the ventilatory response when transitioning from wakefulness to sleep. Also note the interplay of hypoxic and hypercapnic stimuli, characterized by leftward shift and steeper slope of the PCO2 response curve. The circle and square represent the operating point during calm resting breathing during wakefulness in normoxic (circle) and hypoxic (square) conditions. The vertical dashed arrows depict change in operating conditions when there is sudden sleep onset.
State-Dependent Changes
During sleep, however, there is a reduction of the magnitude and slope of the ventilatory response to hypoxia and hypercapnia (see Fig. 3). Such sleep/wakefulness state-dependent differences are evident during wakefulness as well. Specifically, despite a reduction of PaCO2 below 36 mm Hg in Figure 3, the minute ventilation remains stable at about 5 L/min, exemplifying that there is an inherent wakefulness drive to breathe. Conversely, during sleep there is no such horizontal line or “hockey-stick” appearance of the CO2 response curve (ie, wakefulness drive to breathe). Therefore, in a patient receiving mechanical ventilation, when such wakefulness drive to breathe is removed by the onset of sleep, if a patient were to be hypocapnic and there were no backup rate, then a central apnea may ensue.2,3
Exemplar 3: Apnea During Invasive Mechanical Ventilation
A 54-year-old man recovering from cardiogenic pulmonary edema secondary to acute myocardial infarction is awaiting cardiac catheterization in the morning. Although he is intubated and mechanically ventilated, he is alert but agitated as he has difficulty breathing with the machine. The respiratory therapist changes him from VC-CMV to pressure support of 15 cm H2O and maintains the PEEP and FIO2 at 8 cm H2O and FIO2 0.50. The patient becomes less agitated and appears more comfortable and is generating tidal volumes between 700 mL and 900 mL. At 10:00 pm he receives an aliquot of midazolam for nighttime sedation, to ensure adequate rest. The nighttime nurse notices recurrent ventilator alarming and notes that the apnea ventilation has been triggered off and on. The patient is placed back on VC-CMV and the apnea alarms are prevented.
In this exemplar, the patient with heart failure and J-receptor stimulation is more likely to be hypocapnic, and with sleep onset in the absence of a backup rate (pressure support only), the central apneas ensued. Previous studies demonstrated that apneas during mechanical ventilation are not unique to healthy subjects receiving assisted ventilation under experimental conditions, but can occur in critically ill patients receiving mechanical ventilation.3–5 However, the clinical implication of the occurrence of such central apneas during mechanical ventilation is unclear. Conceivably, such central apneas could disrupt sleep and lead to unfavorable stress responses or even neurological effects, such as delirium.6–8
While the occurrence of central apneas are gross changes in patient-ventilator interactions in response to sleep/wakefulness state changes, more subtle changes can occur as well. For instance, inspiratory time can increase by 23% and expiratory time can increase by 126% with the change from wakefulness to sleep,3 which would reduce the respiratory rate, which during pressure support ventilation is used as a measure of respiratory unloading. Conceivably, clinical decisions, such as determination of the pressure-support level, could be influenced by the sleep/wakefulness state when the physician is setting the ventilator. This is particularly important when more profound changes are anticipated, as in the exemplar below.
Exemplar 4: Going to Surgery
A frail 33-year-old woman is admitted with severe acute respiratory distress syndrome and is receiving low-tidal-volume mechanical ventilation. Her ventilator settings are VC-CMV with a backup rate of 14 breaths/min, a spontaneous rate of 32 breaths/min, tidal volume of 360 mL, FIO2 of 0.70, and PEEP of 12 cm H2O. Her arterial blood gas values are pH 7.25, PaCO2 44 mm Hg, and PaO2 71 mm Hg. Serum chemistries reveal a large anion-gap metabolic acidosis, elevated serum lactate, and acute renal insufficiency (serum creatinine 2.1 mg/dL and serum potassium 4.5 mEq/dL). The patient is easily arousable and cooperative, and grimaces when her abdomen is touched. She is quickly diagnosed with a perforated duodenal ulcer and she needs to undergo emergency laparotomy. She is taken to the operating room and general anesthesia is induced easily, as she was already intubated. Before surgery can commence, she develops profound bradycardia and severe hypotension with broad QRS complexes, and arterial blood gas analysis reveals pH 6.95, PaCO2 69 mm Hg, and PaO2 61 mm Hg, and serum potassium concentration is 6.2 mEq/dL.
State-dependent changes in control of breathing that occur with deep sedation during anesthesia could lead to life-threatening situations. In this exemplar the patient's spontaneous respiratory rate was 32 breaths/min, despite a machine-set (backup) rate of 14 breaths/min. Following induction of anesthesia, her respiratory rate fell from 32 breaths/min to 14 breaths/min, with worsening of respiratory acidosis (compounded by large dead space in this patient with acute respiratory distress syndrome) due to the loss of wakefulness drive to breathe and CO2 responsiveness following induction of anesthesia.
Other mechanisms besides chemical influences may play a role in the state-dependent changes in ventilation. In critically ill patients receiving pressure support, an increase in tidal volume, achieved by small increments in pressure assist, prolonged (neural) expiratory time and decreased respiratory rate.9 Such a prolongation of expiratory time in response to lung inflation (the Hering-Breuer reflex) is known to be operational during sleep and not during wakefulness, and is mediated by the neuromechanical sensors of the respiratory control system (see Fig. 1).10
Interplay of Stimuli
The integrated system responses to alteration of stimuli (such as hypercapnia or hypoxia) are more than additive.11 In Figure 4, during hypoxia the ventilatory response to increments in PaCO2 is shifted to the left and is steeper than that during normoxia. Such a shift in the ventilatory response can result in ventilatory instability, which was exemplified in exemplars 3 and 4 above. Such complexity in the respiratory system's operation can be used as a schematic to model and test responses to interventions and therapy. The stability of the integrated response of the respiratory system to ventilatory stimuli, depicted in Figure 1, can be summed up as loop gain. Loop gain is essentially an engineering term that describes the stability of a system controlled by feedback loops, such as the human respiratory system. A loop gain close to zero indicates stability, whereas a loop gain close to, or greater than, one indicates an unstable system.12 Various factors besides the coexistence of hypoxia can destabilize the respiratory controller. Specifically, arousals from sleep, rapid transitions from wakefulness to sleep state (as in exemplar 4), hypocapnia, and administration of pressure assist such as pressure support could augment the CO2 responsiveness slope and thereby increase loop gain and ventilatory instability.11 Moreover, slow circulation (eg, in a patient with congestive heart failure, as in exemplar 3) could create delays in the respiratory controller's response “sensing,” and therefore response to changes in PaCO2 could cause oscillations in the system and ventilatory instability.5

Integrated response of the respiratory controller to changes in hypercapnic stimuli, depicted as ventilatory response to changes in PCO2. Changes in ventilatory response during wakefulness are depicted by black lines. Changes in ventilatory response during various stages of sleep are depicted by gray lines. Note the interplay of hypoxic and hypercapnic stimuli, characterized by leftward shift and steeper slope of the PCO2 response curve, and how various other factors (eg, PEEP, FIO2, sedatives, acetazolamide, and external CO2 administration) can stabilize the respiratory controller, whereas hypoxia, pressure support (PS), and sedatives can destabilize the respiratory controller. The circle and square represent the operating point during calm resting breathing during wakefulness in normoxic (circle, point B) and hypoxic (square, point A) conditions. The vertical dashed arrows depict change in operating conditions when there is sudden sleep onset. Note how the sudden onset of sleep at point A could result in minute ventilation of zero (central apnea), whereas a similar situation at point B would result in reduced ventilation but not apnea.
Alternatively, ventilatory instability can be improved by administering acetazolamide, or increasing CO2 by increasing dead space, or administering CO2 gas.3,13 Moreover, correcting hypoxia by increasing FIO2 or PEEP could attenuate the steep slopes in the ventilatory response curves to hypercapnia, and thereby stabilize breathing. For example, in the presence of hypoxia a patient could be operating at point A in Figure 4. If this patient were to suddenly fall asleep, then ventilatory response would fall to 0 L/min, resulting in a central apnea. In contrast, if the patient were not hypoxic, the patient would have been operating at point B in Figure 4, and sudden sleep onset would decrease ventilation but not cause an apnea. Also, reducing the pressure assist (pressure support) level could prevent such ventilatory instability and apneas.4,14,15 Such an integral knowledge of applied physiology could help the bedside clinician troubleshoot the problem and take corrective action.
Three Pumps
In general, during mechanical ventilation the relationship between the respiratory system and the mechanical ventilator is considered to be 2 pumps working in concert. However, a commonly overlooked layer of complexity is that during mechanical ventilation there are actually 3 pumps that need to be working in synchrony: the ventilator, and the inspiratory and expiratory muscle pumps (Fig. 5). The complex respiratory controller, replete with chemical and neural “servo” inputs and cortical inputs, is attached to the mechanical ventilator, which is controlled by a rudimentary set of microcircuitry. The interaction between these 2 systems, 3 pumps, and 2 controllers—one servo-operated and the other rules-based with lack of any relevant feedback (servo) loop—is a clear mismatch and needs rethinking. Why do we need to study the interaction between the respiratory controller and the circuitry and algorithms that control the ventilator pump? The study of the interaction between these 2 systems and 3 pumps is vital to ensure adequate patient-ventilator synchrony, which, in turn, would ensure adequate respiratory muscle rest, gas exchange, and patient comfort. For these goals to be achieved, we need to have an in-depth understanding of respiratory control during mechanical ventilation, and more importantly, ultimately we need to model the circuitry and algorithms of the mechanical ventilator to parallel that of the respiratory controller.

The interaction between 3 pumps (inspiratory, expiratory, and ventilator) acting on the same column of air, that are differentially controlled by a complex feedback-based respiratory neural controller in humans, as opposed to a simple bank of microcircuitry of the mechanical ventilator that is devoid of (chemical or neural) feedback loops.
The interaction between the patient and the ventilator can be dissected during the course of a single breath and over multiple breaths in order to better understand control of breathing as it pertains to patient-ventilator interaction. Over a single breath, as shown in Figure 6, the breath could be broken into 5 time segments: the trigger phase (ie, the switch from expiration to inspiration); the post-trigger phase; the inspiratory phase; the cycle phase (ie, the switch from inspiration to expiration); and the expiration phase.

The phases of a breath during mechanical ventilation.
Delay of triggering can result in a delay between when the patient's (respiratory controller) effort commences and when the ventilator's inspiratory valve is triggered,16 which can increase respiratory effort, and which could spill into the post-trigger and inspiration phases (Fig. 7).17–19 While flow triggering could reduce the inspiratory effort during triggering (compared to pressure triggering), in the post-trigger phase the inspiratory effort is comparable for flow and pressure triggering. Research on newer methods for predicting and timing inspiratory triggering, by going further upstream in the effector arm of the respiratory controller (see Fig. 1), is ongoing, and some of these devices are available for patient care. For example a noninvasive “shape signal” method, wherein the shape of the flow curve during the tail end of expiration is used to predict the next inspiratory effort, has been used in mechanical ventilation of critically ill patients.20 Such efforts have been preceded by similar tracking of flow mechanisms for bi-level positive airway pressure ventilation in ambulatory patients with sleep-disordered breathing, to ensure adequate cycling of bi-level devices.

The juxtaposition of the patient's respiratory cycle (inner ring) versus the corresponding phases of the mechanical ventilator breath (outer ring) can be depicted by this dial-within-a-dial concept. Left: Perfect patient-ventilator synchrony. Right: Phase lag in mechanical cycles that can be easily conceptualized as a slight turn of the outer (ventilator) dial. Note how the mismatch in the inspiratory phase between the patient and the ventilator spills over to the exhalation phase (red arrowhead): the patient has begun exhalation but the mechanical ventilator is still in its inspiration phase. Such a failure to terminate inspiration (ie, cycle delay) could lead to dynamic hyperinflation.
Changes in transdiaphragmatic pressure or diaphragm excitation would be further upstream in the effector arm of the ventilator circuitry (see Fig. 1), but these techniques are invasive and require the placement of an esophageal probe.21,22 Nevertheless, such techniques can reduce triggering and cycling delays and ensure adequate patient comfort, even in awake patients who are receiving invasive mechanical ventilation.21 Moreover, such techniques would ensure adequate ventilatory support during inspiration.23 Such instantaneous feedback from the respiratory controller to the mechanical ventilator would ensure an optimal balance between patient effort and ventilatory assist, after overcoming the work load posed by respiratory resistance and elastance.24
Delays between the onset of the patient's inspiratory effort and respiratory controller and mechanical inspiration could lead to asynchrony at the expiratory-to-inspiratory switch point (see Fig. 7), because the expiration time is truncated by the delay in opening of the expiratory valve.16 Experimental manipulation of the ventilator settings to induce such a delay have been shown to induce asynchrony at the expiratory-to-inspiratory switch point, which, in turn, could lead to dynamic hyperinflation.25 Such dynamic hyperinflation, in turn, can lead to non-triggering effort of the subsequent breath in experimental human models as well as real-life circumstance.16,26 The non-triggering efforts in turn could lead to patient discomfort. However, while the rationale for achieving adequate synchrony between the patient's respiratory controller and the mechanical ventilator is strong, there are currently no outcomes-based studies to confirm the benefit of this approach.
Time
During mechanical ventilation the critically ill patient undergoes many changes that influence the ventilatory responses to various stimuli and state-dependent changes (see Fig. 3). In ambulatory patients with sleep-disordered breathing and daytime hypercapnia, significant increments in ventilatory responses to changes in PaCO2 occurred following 2 days and 2 weeks of continuous positive airway pressure treatment.27 Such changes, which reflect resetting of the medullary centers, can certainly occur in critically ill patients receiving mechanical ventilation, so constant changes can occur over various time frames, ranging from a breath to multiple breaths to minutes to days in the critically ill patient. However, it is not feasible for the intensivist or the therapist to stand at the bedside to keep making adjustments, so closed-loop mechanisms with such protective caveats are needed to effect such time-based changes. While such advances are being made, ambulatory patients receiving noninvasive adaptive servo ventilation or volume-assured pressure support, and similar closed-loop systems, are lacking in the critical care arena, due to regulatory concerns that stem from runaway phenomena in a closed-loop system.28–30 However, such concerns could be mitigated by current sophisticated, multi-layered, rules-base algorithms and miniaturization of computer technology.31
Who Is the Boss?
A key question when designing closed-loop systems is to conceive the parameters and boundaries that will guide the settings and the functioning of the ventilator. Specifically, the question remains as to who is right: the patient or the physician's notion of what is ideal for the patient? (Fig. 8)
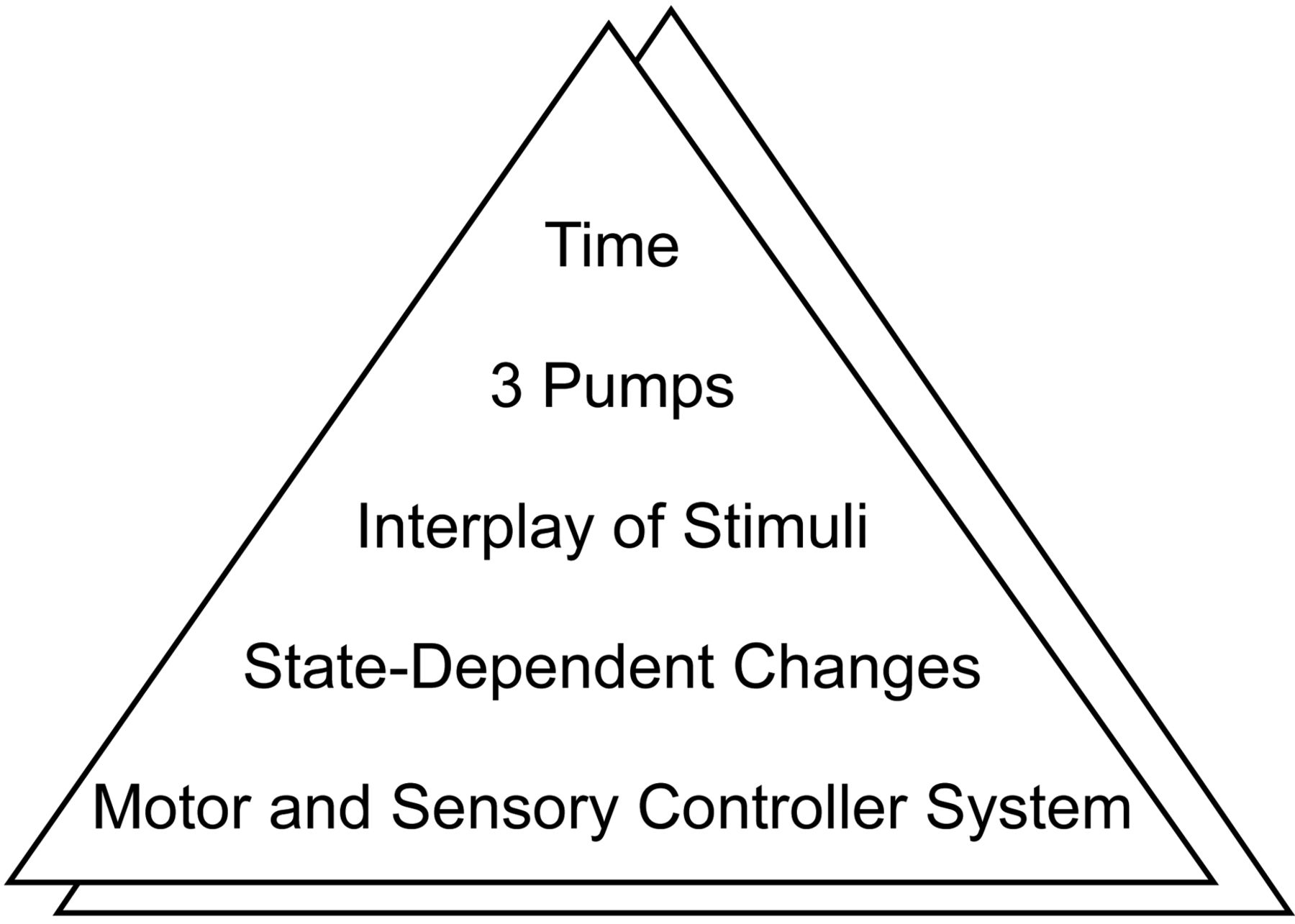
The pyramid depicts concepts that are integral to our understanding of control of breathing in the context of mechanical ventilation. The basic understanding of the motor and sensory components of the respiratory controller form the foundation of this understanding, but sleep-wakefulness state-dependent changes, interplay between various respiratory stimuli, the nature of three (inspiratory, expiratory, and ventilator) pumps acting on the same column of air, and the effects of time compound and nuance our understanding of respiratory control during mechanical ventilation. The identical triangle in the background reflects a parallel universe, and much ignored, or concept of what the patient desires versus the triangle in the forefront that reflects the providers' understanding and construct of control of breathing during mechanical ventilation. Such a paradigm can overturn some of the assumptions a provider or researcher makes on a day-to-day basis.
Specifically, in determining the optimal ventilatory strategy, is allowing the patient's intact respiratory controller to respond to a given clinical state paramount, or is the avoidance of the adverse effects of ventilatory effort on respiratory muscle more important? And are there trade-offs? And, if so, how much do we unload or load a patient? These gnarly questions need to be untangled so as to allow us to advise the closed-loop system appropriately. The above dilemma could be better understood with the following exemplar.
Exemplar 5: To Unload or Not to Unload: That Is the Question
A 42-year-old man is recovering from status asthmaticus and steroid-induced myopathy. His oxygenation and ventilatory mechanics are adequate, but, due to profound weakness, he has repeatedly failed attempts to liberate him from mechanical ventilation. Between the spontaneous breathing trials, the patient is placed on VC-CMV. But a new episode of ventilator-associated pneumonia and acute respiratory distress syndrome requires deep sedation and low-tidal-volume ventilation.
Passive mechanical ventilation is associated with marked atrophy of the diaphragm and increased diaphragmatic proteolysis, so in clinical practice we try to avoid suppressing the patient's spontaneous respiratory effort.32 In this “difficult-to-wean” patient with profound respiratory muscle weakness, the administration of VC-CMV and deep sedation may lead to periods of passive mechanical ventilation that are difficult to monitor and adjust-for at the bedside.33,34 Animal studies have not clearly defined the minimal duration of controlled mechanical ventilation that invariably results in ventilator-induced diaphragmatic dysfunction.35 Therefore, state-dependent changes in respiratory rate may lead to excessive respiratory muscle resting and resultant muscle atrophy.32 In exemplar 5, both VC-CMV and pressure support were valid options, and there are animal data to suggest that pressure support is less likely to cause muscle atrophy.34 But pressure support may be associated with sleep-related central apneas and sleep disturbances,3 so the ideal ventilation settings would be pressure support with a backup rate, which would sense patient-triggered versus machine-mandated breaths and guarantee a certain proportion of patient-triggered breaths.
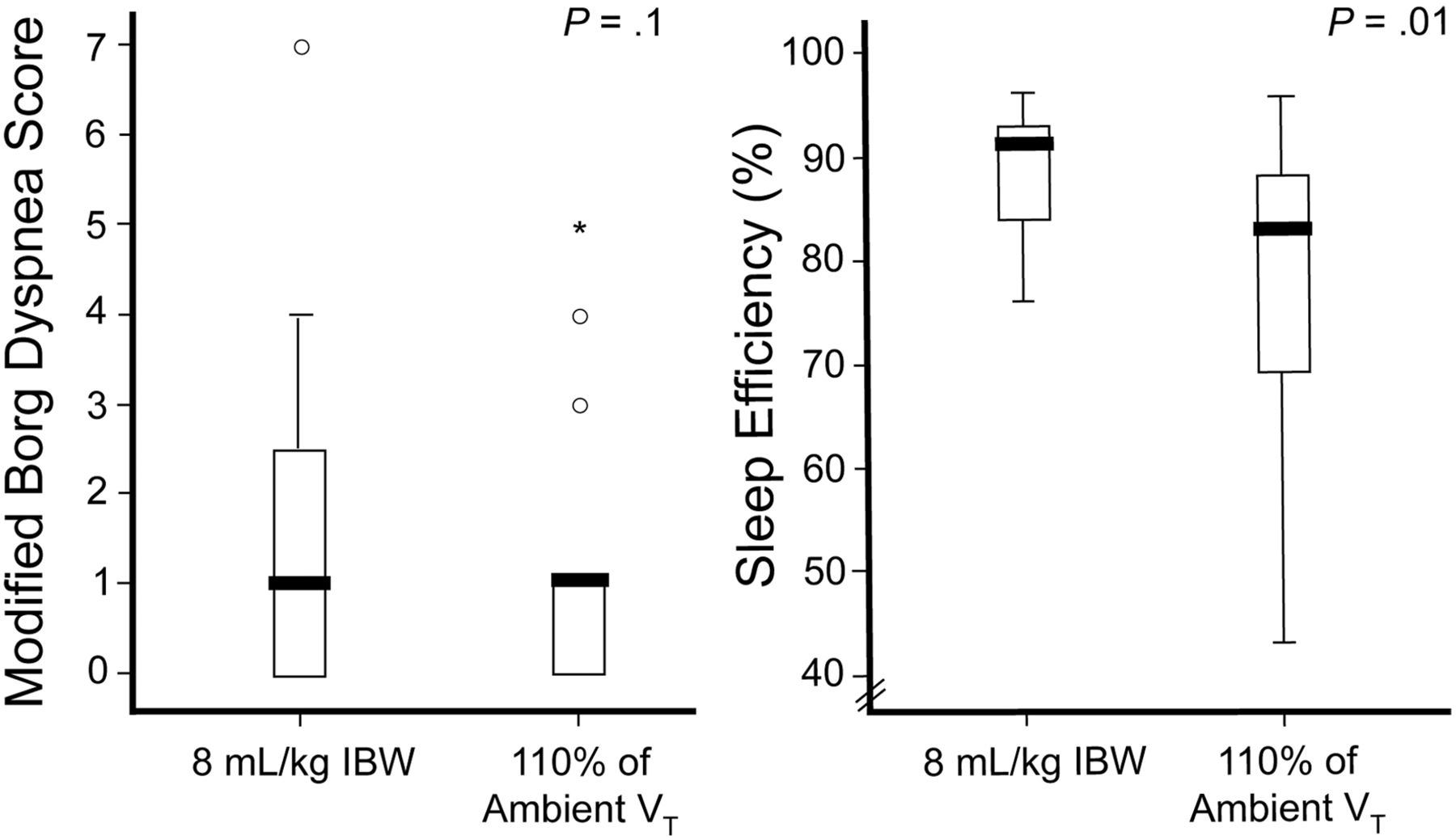
Similarly, the choice of tidal volume may be influenced by the state of the respiratory controller: sleep or wakefulness.30 In patients with chronic respiratory insufficiency receiving averaged volume-assured pressure support, tidal volume was chosen with 2 methods: one based on patient preference (110% of ambient tidal volume during calm wakefulness), and another based on ideal body weight (8 mL/kg ideal body weight) (Fig. 9). The patients preferred (as measured via dyspnea) 110% of ambient tidal volume during wakefulness, but the patients slept better (as measured via sleep efficiency) when receiving tidal volume based on ideal body weight.30 On the one hand, this state-dependent change in the respiratory controller can significantly impact intermediate physiological endpoints such as sleep and dyspnea. Moreover, such data would suggest that ventilators that can sense sleep/wakefulness may be warranted. More importantly, such data further underscore that it is unclear as to who knows what ventilator setting is best: the patient or the provider.
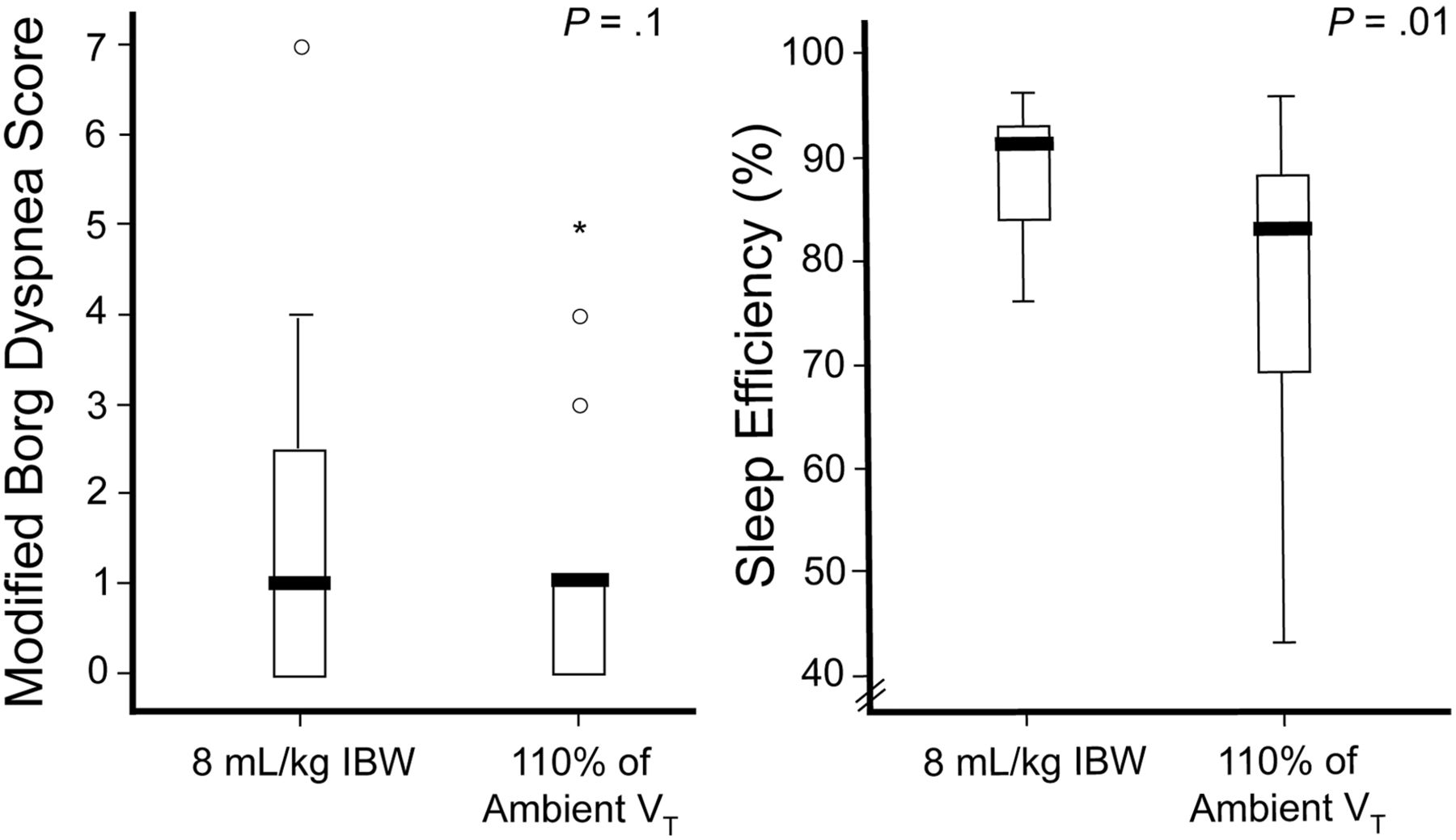
State-dependent and patient-dependent differences in intermediary physiological end points. In patients with chronic respiratory insufficiency receiving averaged volume-assured pressure support, tidal volume was administered based on 2 different methods: one based on ideal body weight (8 mL/kg IBW), the other based on patient preference (110% of ambient tidal volume during calm wakefulness). The patients preferred (as measured by subjective dyspnea ratings) 110% of ambient tidal volume during wakefulness (left), but the patients slept better (as measured by polysomnography-based sleep efficiency) (right) when receiving tidal volume based on ideal body weight. (Adapted from Reference 30.)
Future Directions
Market forces are a factor that needs to be dealt with when contemplating new computerized “intelligent” systems that enable adequate mechanical ventilation while addressing the control-of-breathing issues. Whereas the sleep medicine field has benefited from a larger sales market, the same has not been the case for mechanical ventilation in the acute critical care unit. Another obstacle is the regulatory concern over closed-loop systems and the lack of clear scientific data that would guide ventilator settings in different patient populations. While the current focus of patient-ventilator interactions in the context of control of breathing addresses intermediate physiological endpoints such as dyspnea and gas exchange, more long-term studies that measure tangible outcomes such as ventilator dependence and mortality are needed.
Discussion
Hess:
I was intrigued by your discussion of apnea and periodic breathing. Should we consider no effort at all also a form of asynchrony?
Parthasarathy:
It also depends upon the duration. The absence of breath—in fact, when we were trying to figure out these apneas, we found there were some patients who had short apneas, and I wanted to score them because I was biased, but we did not score them. We used the same methods as the sleep laboratory. In pediatric patients two missed breaths is considered an apnea, because they breathe at a faster rate, and so there isn't a 10-second requirement. One could make the argument that even one missed breath is a form of asynchrony, and I would probably agree.
Kacmarek:
If we look at traditional modes versus new modes such as NAVA [neurally adjusted ventilatory assist] and PAV [proportional assist ventilation], from the sleep perspective, are the new modes better or worse?
Parthasarathy:
In the ICU [intensive care unit] population, I don't know about NAVA, but Karen Bosma found that PAV was superior to pressure support, and there was more REM [rapid eye movement] sleep and less sleep fragmentation.
Kacmarek:
How about assist control? You showed that it was better than pressure support.
Parthasarathy:
I don't know of any data on PAV versus assist control in critically ill patients.
Kallet:
Sai, you said you were going to come up with something provocative, and your last statement—that mechanical ventilation should move to something fully automated—certainly delivers! The current state of things is that we have simple volume-control or pressure control ventilation. The advantage of these modes is their simplicity. We can very quickly troubleshoot a patient's situation, so if there's a change we can diagnose the problem and intervene rapidly. But in closed-loop ventilation you have a sophisticated controller, and the clinician is outside of the decision loop. The problem I see is when you have a patient who is unstable, hypotensive, hypoxemic, and maybe acidotic, and their condition is rapidly changing. How do you troubleshoot the condition clinically, unless you had some neural network that could just read out something?
Parthasarathy:
There should always be an escape mechanism. There should be a complex neural network type of thing that every patient gets, including variability in breathing, which affords better oxygenation and benefits from all of such concepts. But if your patient gets into a dire strait and is in trouble, you should be able to opt out of that and go to the ventilation mode that you're comfortable with.
Kallet:
I think this will radically change the respiratory care profession, because therapists are going to have to be trained differently. If we have a sophisticated neural network controlling the ventilator, then it doesn't seem very realistic that we're going to continue doing ventilator checks. If anything, we'll be assessing trends or overseeing assessment outputs from the ventilator telling us what's happened. The therapist of the future is going to have to start interpreting patterns and become much more sophisticated. I think that if fully automated closed-loop ventilation really comes to fruition, it's going to change the respiratory care profession; we're not going to have the same kind of respiratory therapists we've had for the past 30 years! They're going to have to be much more sophisticated to work in the ICU and provide that type of ventilation.
Parthasarathy:
I think the focus will be more on therapy rather than troubleshooting the ventilator. I know a robotics surgeon who says the entire field of surgery is moving towards robotics surgery. He forecasts that everyone is going to be doing robotics surgery, and there will come a time when the robot malfunctions and they'll have to find an old retired surgeon who can do surgery without a robot. That happens when there's a huge reliance on machines.
The flip side of the argument is that it's probably a reflection of my background and my training. I'm one of the few in Tucson who looks at static lung compliance and airway resistance on a daily basis on the ventilator. Few practitioners—no offense to them, as they are excellent practitioners—use such monitoring. It all depends on where they came from. Few look at a patient's percent of expected static lung compliance today and compare it to the patient's static compliance yesterday, and ask if the lung compliance is helping or hurting his chances of getting him off the blower? I use this on a daily basis and it serves me well, I think. If the resistance is high, I crank up their bronchodilators or I kick in some steroids. Some practitioners are not practicing that, and so the respiratory therapists are just marking those numbers on the flow sheet but their patients are doing just the same. I'd like to think that my patients are doing better. Something as simple as that and we haven't been able to get it out into the field and have everyone conform.
Newt Gingrich, in a plenary speech to the National Governors Association almost a decade ago, compared the system used by the aviation industry that allows correction of major errors within 48 hours, to the estimate by the National Institute of Medicine that it can take up to 17 years for doctors to adopt a new procedure that can save lives. Seventeen years after two randomized controlled trials have shown the desired change before physicians change their practices. We really need to get to more expeditious dissemination and implementation of research findings, and I think it's possible.
Younes:*
Sai, I am very impressed by your observations about the change in breathing pattern when people go to sleep on a ventilator. I'm just wondering whether a difference in breathing pattern, volume, frequency, or whatever, when someone goes to sleep is not a good indicator that the ventilator is not set properly. I'm sure everyone here has breathed on a ventilator and knows it's very uncomfortable if not set properly. The difference between the asleep and awake breathing pattern may be that the patient is trying to adjust to the poorly set ventilator when awake, but this conscious adjustment disappears during sleep. Maybe when we see a big difference between the awake and asleep pattern we should adjust the ventilator to minimize that difference.
I support Dr Hess's comment about apneas being asynchrony, and I've done a lot of theoretical work about that. When a patient is over-assisted, he will have to drop breaths, because if you force him to have a tidal volume of one liter and the respiratory rate is 30 breaths a minute and he doesn't need 30 L/min of ventilation, he'll have to drop breaths. The difference between dropping a breath now and then, such as with ineffective efforts, or dropping a bunch of breaths, as in central apnea, is basically the mechanical time constant of the respiratory system. If the mechanical time constant is short, the patient will develop central apneas if they're over-assisted. If the mechanical time constant is long, the patient will develop ineffective efforts.
de Wit:
I'd like to expand on the apneics. I see 3 to 6 of these patients per year, and they're typically patients with hepatic encephalopathy who have received no sedation, and they're unresponsive to outside stimuli. They're apneic, but as soon as air flow enters the trachea, they have an exuberant response and they will try to pull a liter or a liter and a half of tidal volume. But if you put these patients on pressure support, they are apneic. Would you comment on the control of breathing in these patients?
Parthasarathy:
I think it's an individual trait. It can also be an effect of sedation and intrinsic benzodiazepine-like substances. Some have made the observation that sedatives and narcotics cause central apneas in some of them. It's multifactorial, just as there is a long list of causes of central apnea, and it's essentially a mismatch of the minute ventilation asleep versus awake. It could happen on the falling-asleep side (ie, rapid sleep onset), as I showed on those tracings. It could also happen on the arousal response, characterized by an exuberant ventilatory response to awakening, which sets them up for hypocapnia, which in turn sets them up for apnea when they descend back into sleep.
Branson:
I want to say that I'm a fan of closed-loop control, and that we've had closed-loop control in some forms that most people aren't aware of. Even back to the Puritan Bennett 7200, the gain changed based on the strength of the patient effort. There's already a lot of closed-loop control going on: it's just not stated. My problem with closed-loop control is no different from what Rich Kallet mentioned: that it is, in fact, the controller. Now the ARDS Network “mafia” doesn't want us to let anybody have a tidal volume more than 6 mL/kg, no matter what, and we can make that happen with closed-loop control. What we really need is what Rich Kallet suggested: the machine has to adapt to the patient and allow the patient to have a variable ventilatory pattern, because that's what people do: that's normal. I'm not suggesting that we have to somehow program biologically variable ventilation, as some have suggested. I'm suggesting that we have to do a better job of following the patient's wants and needs versus imposing our will. If we impose our will, it doesn't matter what it is, because it's the same end result.
Parthasarathy:
I don't know the answer when it comes to what the patient wants versus what we think they need. We don't really know who's right. We should do a multicenter trial to figure that out. But before we do that we need to devise a machine that can actually do all these things well. We'd then randomize patients to that device or a conventional ventilation mode. It all starts with us coming up with a device that can do all of that, and I think the FDA [Food and Drug Administration] needs to loosen some of the controls in this area. In other words, it should be an automatic thing that the physician is comfortable with. Until we do that, we're always going to be asking ourselves questions.
Epstein:
I love what you said about the need to automate this process and how essential that is, but that doesn't exist now and it may not for some time. Poor Dave Pierson has to summarize this conference, and hopefully part of that summary will be practical recommendations to people who care for these patients. We need to make sure that we have something in the future, but there are a lot of folks who have to take care of these patients tomorrow, and we want to give them recommendations—limited though they may be—for how to manage patient-ventilator interaction.
Gentile:
A growing population in ICUs in North Carolina is obese patients, many with OHS [obesity hypoventilation syndrome], chest-wall issues, and hypoxemia. How does that patient population fit in with your ongoing trial? They are difficult to synch with the ventilator because of mechanics and drive to breathe.
Parthasarathy:
In our ongoing trial of patients with sleep-disordered breathing, the EPAP [expiratory positive airway pressure] or PEEP level, the backup rate, and the pressure support are all automatically determined. And the EPAP is automated to obstructive events, so in an obese patient on noninvasive ventilation the EPAP is automatically titrated based on the flow tracings and the “flattening index.” One of the algorithms looks at snoring and things of that nature, and there are 5 algorithms that determine the EPAP. So, regardless of whether it's a patient with central apnea or an obese patient with obstructive and central apneas, all three of those numbers are automatically adjusted, and each one is predicated on 4 or 5 algorithms. It's a pretty complex operation, but it's feasible, and it works in obese patients too. We just have to do that.
Gentile:
I think in noninvasive ventilation that's OK, as long as there's some safety stops. Invasively, I think that the majority of the people in the room here are not going to turn PEEP titration over to the machine because of potential negative effects on hemodynamics.
Parthasarathy:
That concern has been raised. We need a multicenter trial of whether such therapy affects mortality. That is a huge concern for folks like Javaheri and colleagues [personal communication], because of concerns about the effects of PEEP on cardiac output, because of what PEEP does to venous return, and things of that nature. You can set parameters and say, “I don't want the CPAP level to go beyond a certain level because I think it could be injurious to this patient,” and you can set that range, and then it will oscillate within that range and alert you if it's not an effective range.
Hess:
To get to your point, Mike, I think we could do that if we were sophisticated enough. I don't think we should have to worry about the effect of the ventilator adjusting PEEP on blood pressure because we can measure blood pressure very easily at the bedside, and that should come into the algorithm. We need to think beyond just what the ventilator is monitoring. We can feed all kinds of information into our decision control tool—all the information we get from the bedside monitor: what kinds of hemodynamic support the patient is getting, whether the patient is receiving vasopressors, what the dose is. It's just a matter of how sophisticated we make the system.
Chatburn:
I agree with that Dean, but the other issue is the reliability of the signal. If it loses the signal or there's noise in the signal, it has to revert back to a simpler control scheme.
Hess:
Correct. There is the issue of artifact rejection, for example.
Footnotes
- Correspondence: Sairam Parthasarathy MD, Research Service Line, Southern Arizona Veterans Affairs Health Care System, University of Arizona, 3601 S Sixth Avenue, Mail Stop 0-151, Tucson AZ 85723. E-mail: spartha{at}arc.arizona.edu.
-
This work was partly supported by National Institutes of Health grant HL095748.
-
The authors have disclosed no conflicts of interest.
-
Dr Parthasarathy presented a version of this paper at the 46th Respiratory Care Journal Conference, “Patient-Ventilator Interaction,” held March 19-21, 2010, in Cancún, Quintana Roo, Mexico.
↵* Magdy Younes MD FRCP(C) PhD, Department of Medicine, University of Manitoba, Winnipeg, Manitoba, Canada.
- Copyright © 2011 by Daedalus Enterprises Inc.
References





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Basics of Control of Breathing
- Exemplar 1: Respiratory Controller Versus Preventing Lung Injury
- Exemplar 2: Spurious Ventilator Dependence Due to Exuberant Ventilation
- State-Dependent Changes
- Exemplar 3: Apnea During Invasive Mechanical Ventilation
- Exemplar 4: Going to Surgery
- Interplay of Stimuli
- Who Is the Boss?
- Exemplar 5: To Unload or Not to Unload: That Is the Question
- Future Directions
- Discussion
- Footnotes
- References
- Figures & Data
- Info & Metrics
- References