

Abstract
BACKGROUND: The incidence of community-acquired pneumonia (CAP) is relatively high in elderly subjects. Cough peak flow (CPF) is an objective indicator of cough strength, and CPF evaluation might be useful to assess whether food intake can be restarted. We aimed to examine whether cough strength assessed with CPF can be used as an indicator of the aspiration risk when restarting food intake in elderly subjects with CAP.
METHODS: This cross-sectional study included 82 elderly subjects with CAP between August 2016 and March 2018. CPF was measured using a peak flow meter, and we performed the repetitive saliva-swallowing test (RSST), which is a videoendoscopic evaluation of swallowing and is used to assess dysphagia and aspiration. Receiver operating characteristic (ROC) curve analysis was performed. The cutoff value was determined, and the area under the ROC was calculated.
RESULTS: The areas under the RSST and CPF curves were 0.87 and 0.83, respectively. The RSST value for identifying the aspiration risk was 2.5 swallows. The sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio were 70.0%, 71.7%, 2.5, and 0.42, respectively. The CPF for identifying the aspiration risk was 190 L/min. The sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio were 82.6%, 69.4%, 2.7, and 0.25, respectively.
CONCLUSIONS: Our findings suggest that cough strength assessed with CPF can be used as an indicator of the aspiration risk when restarting food intake in elderly subjects with CAP and that CPF evaluation is not inferior to the RSST. However, CPF evaluation should be performed together with swallowing screening tests to determine the aspiration risk.
Introduction
Pneumonia is the fourth most common cause of death among individuals aged ≥ 65 y in Japan, and the incidence and treatment rates tend to increase with age.1 According to a multi-center collaborative study conducted in the United Kingdom, the frequency of community-acquired pneumonia (CAP) increases with age among hospitalized subjects with pneumonia.2 Additionally, a previous study reported that the frequency of CAP or health care–associated pneumonia (ie, aspiration pneumonia) was approximately 20% among people in their 50s, approximately 50% among those in their 60s, approximately 70% among those in their 70s, approximately 80% among those in their 80s, and approximately 90% among those age ≥ 90 y.3 Dysphagia has also been reported to be an independent risk factor of CAP and a cause of aspiration in elderly subjects with CAP.4
In addition to dysphagia, a decline in the voluntary cough strength contributes to pneumonia. A strong cough has been shown to decrease the incidence of pneumonia in stroke subjects with dysphagia.5 A decline in the voluntary cough strength among stroke subjects has been shown to increase the risk of aspiration.6,7 In addition, a decreased cough strength has been reported to be a strong predictive factor of respiratory complications in subjects with dysphagia.8 The results of these previous studies suggest that the cough strength should be evaluated when considering oral intake resumption in elderly CAP patients with dysphagia.
Considering the potential for aspiration, many elderly patients with CAP are required to temporarily fast after admission to our hospital. The severity of dysphagia and the presence of aspiration are confirmed using a swallowing function test before food intake is restarted. Because restriction of oral food intake due to dysphagia can lead to nutritional deficiencies, pulmonary complications, dehydration, and other complications,9 food intake should be resumed as quickly as possible in elderly patients with CAP, while making sure to avoid aspiration. The accepted standard methods for the diagnosis of dysphagia and aspiration are videofluoroscopic examination of swallowing and videoendoscopic evaluation of swallowing.10 However, these examinations can be performed in only a limited number of facilities because they are invasive, they present environmental equipment problems, and there is a shortage of skilled staff. The repetitive saliva-swallowing test (RSST)11,12 and the modified water-swallowing test13,14 are often used as simple screening tests for dysphagia and aspiration. Among dysphagia screening tests that are used to evaluate whether oral food intake should be restarted in patients with acute pneumonia, the RSST (cutoff value, once) has been reported to be the most useful due to its sensitivity of 81% and specificity of 67%.15 However, the RSST does not adequately detect micro-aspiration or silent aspiration; thus, it is important to identify the presence of the coughing reflex and the cough strength required to expel aspirated foreign objects.16 Cough peak flow (CPF) has gained attention as an objective indicator of cough strength and has been used to evaluate the cough strength in various diseases.17–20 Additionally, peak flow meters, which are used to measure CPF, are inexpensive and easy to use, and thus they are frequently adopted in clinical practice. Therefore, we believe that CPF evaluation using a peak flow meter, in addition to dysphagia screening tests, would be useful to rapidly and safely assess whether food intake can be restarted in elderly patients with CAP during the early stages of hospitalization, when respiratory status and function are unstable.
The purpose of this study was to examine whether cough strength assessed with CPF can be used as an indicator of the aspiration risk when restarting food intake in elderly subjects with CAP. We also compared CPF evaluation with the RSST.
QUICK LOOK
Current knowledge
Cough peak flow (CPF) has gained attention as an objective indicator of cough strength and has been used to evaluate the cough strength in various diseases. CPF is important to assess whether food intake can be safely resumed in elderly patients with community-acquired pneumonia (CAP) during the early stages of hospitalization, when respiratory status and function are unstable. Previous studies suggest that cough strength should be evaluated when considering resumption of oral intake.
What this paper contributes to our knowledge
Our findings suggest that cough strength assessed with CPF is an indicator of aspiration risk when restarting food intake in elderly subjects with CAP, and that evaluation of CPF is not inferior to the repetitive saliva-swallowing test. However, CPF evaluation should be performed together with swallowing screening tests to determine the aspiration risk.
Methods
This study was approved by the institutional review boards of Showa Inan General Hospital (No. 2016-8) and Shinshu University (No. 3559). After explaining the content of the study in detail, consent was obtained in writing from all subjects. Additionally, this study was performed according to the provisions of the Declaration of Helsinki. Patient information was sufficiently anonymized.
This cross-sectional study was performed when restarting food intake (7 d after hospitalization) in subjects with CAP who were hospitalized and treated at Showa Inan General Hospital. The study was performed between August 2016 and March 2018. Background data include age, sex, body mass index, body temperature, pneumonia severity (CURB-65 score), medical history (eg, cerebrovascular disease, respiratory disease include interstitial pneumonia and COPD, heart disease, diabetes mellitus, and smoking), functional independence measure (FIM), blood data, oxygen therapy use, respiratory function data, and swallowing function data. Cognitive function was evaluated using the Mini-Mental State Examination (MMSE) in all subjects.
Subject Eligibility Criteria and Exclusion Criteria
The study included elderly subjects with CAP aged 65 y or older. The subjects had normal oral food intake prior to hospitalization. CAP was diagnosed according to the American Thoracic Society/Infectious Diseases Society of America guidelines.21 The exclusion criteria were inability to cooperate sufficiently with the tests due to poor control of subjective symptoms such as dyspnea, disturbance of consciousness (Glasgow Coma Scale score < 15 points), and psychiatric symptoms such as hallucinations and cognitive function decline (MMSE score <23 points). Additionally, patients with drug allergies (ie, lidocaine) were excluded.
Blood Biochemistry Tests
Blood test data included the C-reactive protein level and white blood cell count, which reflect inflammation, and the albumin level, which reflects the nutrition level.
Pulmonary Function Tests
The respiratory frequency at rest was measured when restarting food intake. Tidal volume, percent of vital capacity (%VC), and percent of FEV1 (%FEV1) were measured with a spirometer (Autospiro AS-407; Minato Medical Science, Osaka, Japan).
Cough Peak Flow
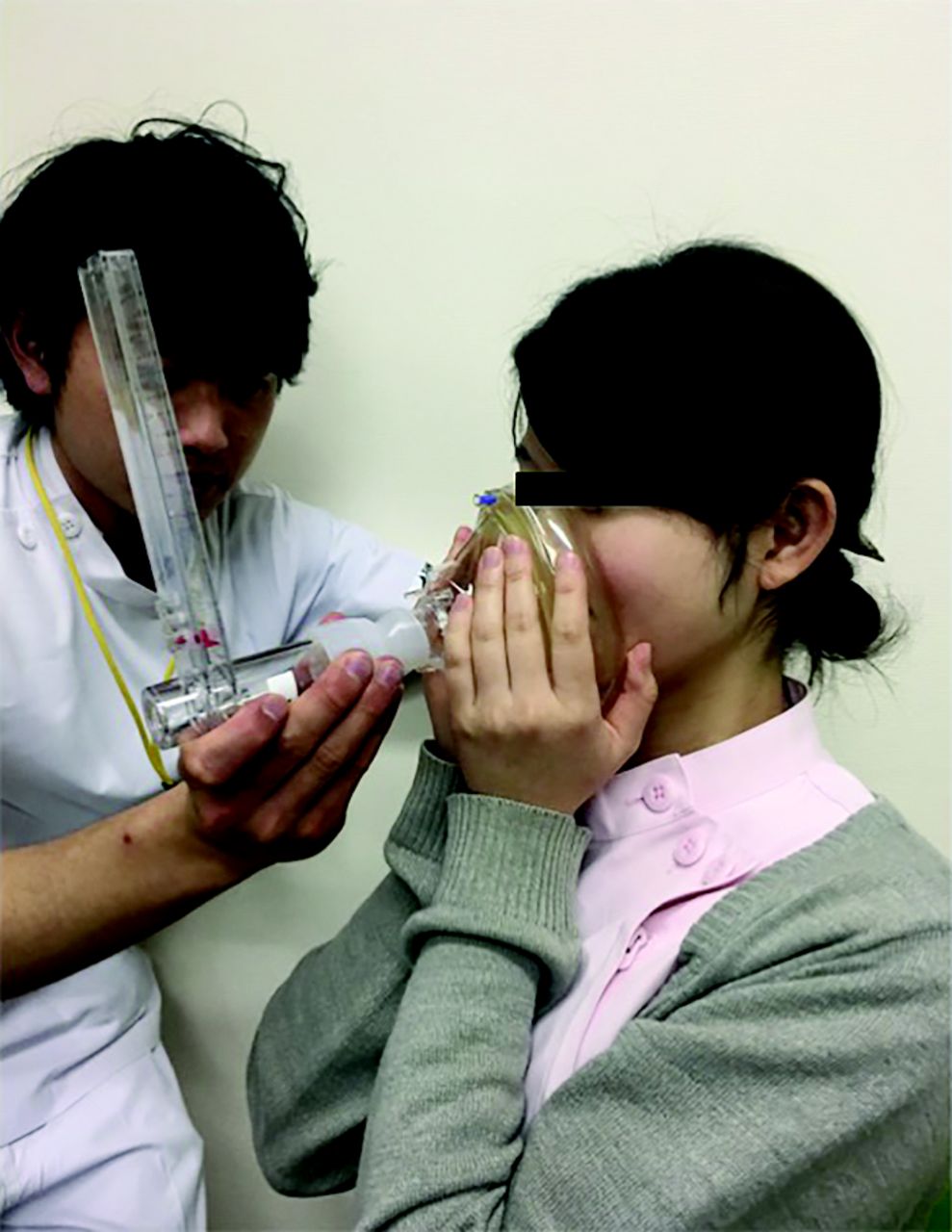
CPF was measured using a peak flow meter (Fuji Respironics, Saitama, Japan) connected to a face mask.18 According to a previous report,22 measurements were performed in a seated position; for subjects with an unstable sitting position, the wheelchair seated position was used (Fig. 1). The measurement equipment was attached firmly to the face to prevent air leakage, and subjects were instructed to breathe deeply and produce the strongest cough possible, so that voluntary coughing would be performed at the maximum inspiratory level. Subjects could cough at any point, and there was no set cough timing. Three measurements were obtained, and the maximum value was used as the CPF value. Before measurement, subjects were provided with an orientation and demonstration of the measurement method, and 2–3 rounds of practice were allowed. Subjects had 30 s between measurements.

Measuring cough peak flow.
Videoendoscopic Evaluation of Swallowing
Videoendoscopic evaluation of swallowing was performed by a physician (FNL 10RBS; Pentax, Tokyo, Japan). The insertion approach was above or below the inferior nasal concha. Lidocaine gel 2% (Xylocaine; AstraZeneca, Osaka, Japan) was used on the scope tube as a demulcent/surface anesthetic. Subjects underwent the endoscopic swallowing evaluation while sitting in a chair or sitting up in bed. A lubricated endoscope was passed transnasally, typically on the floor of the nose, to obtain a superior view of the hypopharynx. The endoscope was then moved throughout the examination between the swallowing and post-swallow positions to collect images. The obtained images were scored according to the fiberoptic endoscopic evaluation of swallowing (FEES) system.23
RSST
Generally, with the subjects in a seated position, the examiner used the index finger to palpate the lingual bone and the middle finger to palpate the thyroid cartilage while the subjects swallowed, and the swallowing count in 30 s was determined. A swallow was only counted when the thyroid cartilage sufficiently rose past the middle finger.24
Statistical Analysis
To assess the usefulness of cough strength evaluation for determining aspiration risk, subjects with an FEES total score of ≥ 7 points were classified into a restricted oral intake group, and those with an FEES total score < 7 points were classified into an unrestricted oral intake group, according to a previous report.25
Initially, the chi-square test and Mann-Whitney U test were used to compare age, sex, body mass index, CPF, respiratory frequency, tidal volume, % VC, % FEV1, RSST results, CURB-65 scores, and medical history between the restricted oral intake and unrestricted oral intake groups. Subsequently, the aspiration risk determination predictive power (ie, sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio) was assessed using RSST results and CPF as independent variables and FEES results as dependent variables, with receiver operating characteristic curve (ROC) analysis. The area under the ROC was calculated for the RSST and CPF ROCs, and the efficacy of each test was compared. We used net reclassification improvement and integrated discrimination improvement to compare the ROC.26 The cutoff value of each test was considered as the value of the point closest to the upper-left corner along the ROC.15
For data analysis, calculations were performed with descriptive statistics (mean ± SD). All analyses were performed using SPSS 24.0 (IBM Corp, Armonk, New York) and the statistical package R 3.1.0 (R Project for Statistical Computing, Vienna, Austria). In all statistical analyses, P < .05 was considered to indicate statistical significance.
Results
Subjects
A total of 114 patients were considered for this study. Of these patients, 21 had decreased cognitive function, and 11 died or had condition deterioration (data not reproducible); these patients were excluded. Thus, 82 subjects were included in the final analysis (Fig. 2).
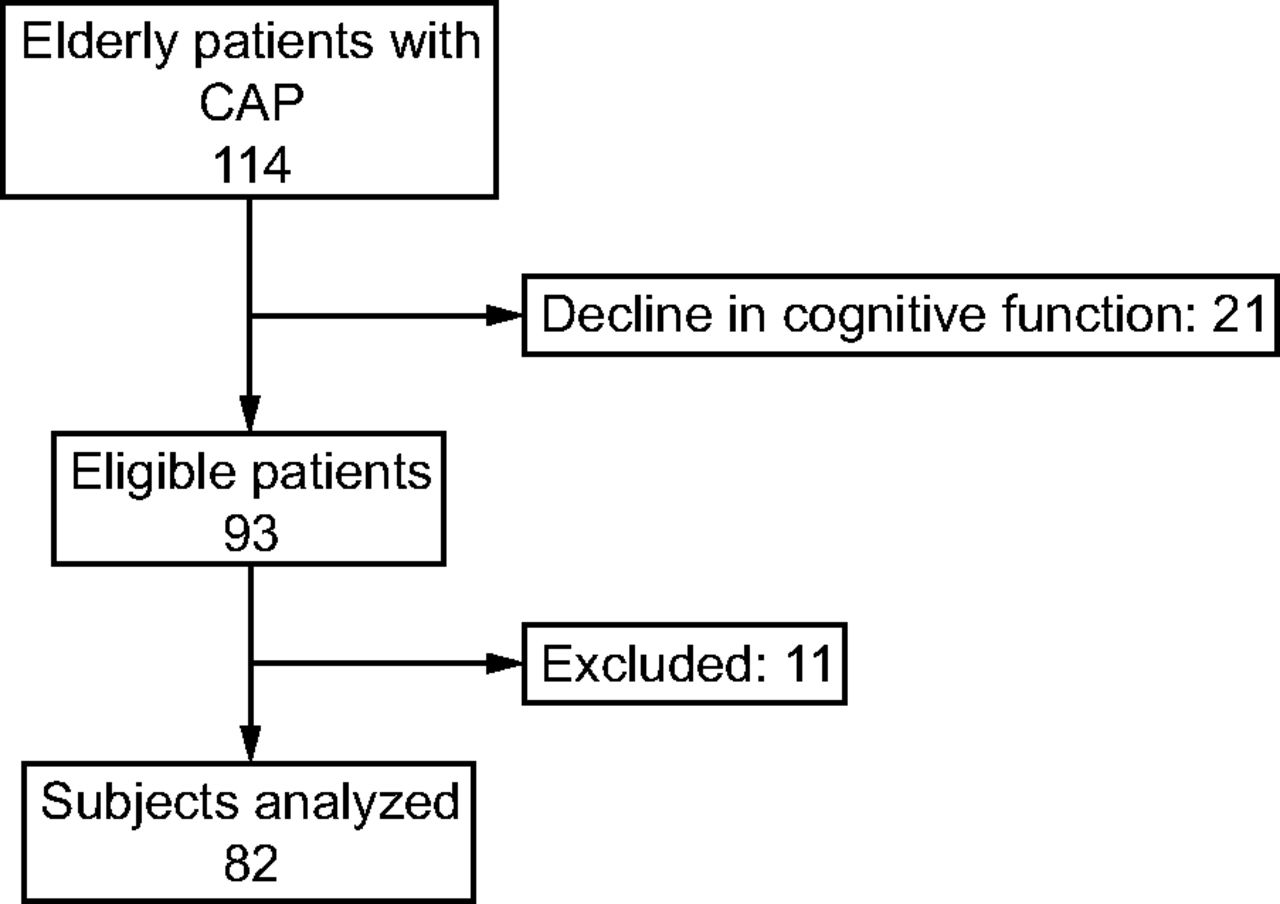
Flow chart. CAP = community-acquired pneumonia.
Characteristics of Subjects in the Unrestricted and Restricted Oral Intake Groups
The characteristics of subjects in the unrestricted and restricted oral intake groups are presented in Table 1. The mean subjects age was 77.1 ± 8.37 y in the unrestricted oral intake group and 80.6 ± 7.6 y in the restricted oral intake group. CURB-65 scores were significantly higher and FIM scores were significantly lower in the restricted oral intake group than in the unrestricted oral intake group (P = .044 and P = .049, respectively). Additionally, the CPF, % VC, % FEV1, and FVC were significantly lower in the restricted oral intake group than in the unrestricted oral intake group (P < .001, P < .001, P = .043, and P = .02, respectively). There were no significant differences in age, sex, body mass index, medical history, body temperature, blood data, or oxygen therapy use between the groups.
Comparison of Oral Intake Independence Group and Oral Intake Restriction Group
Cutoff Values and Sensitivity/Specificity of RSST Results and CPF
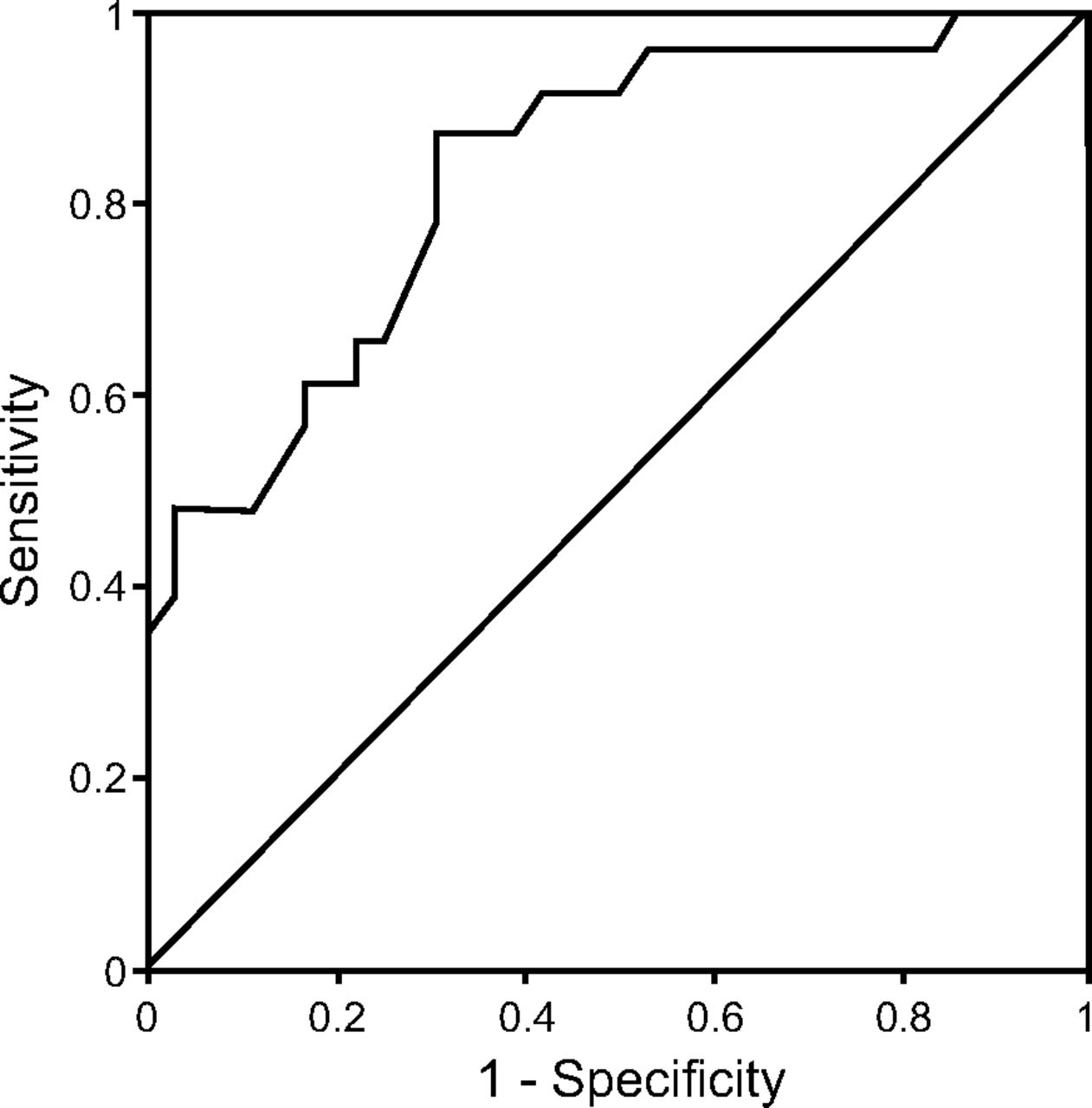
Figures 3 and 4 present the RSST and CPF ROCs, respectively, which were used to determine the aspiration risk when restarting food intake. The areas under the RSST and CPF curves, which represented the usefulness of RSST results and CPF as indicators of aspiration risk when restarting food intake, were 0.87 (P < .010) and 0.83 (P < .010), respectively, and there was no significant difference between the 2 values (P = .42). The RSST value for identifying the aspiration risk was 2.5 swallows, with a sensitivity of 70.0% and a specificity of 71.7%, and when the RSST cutoff value was considered as 2.5 swallows, the positive likelihood ratio and negative likelihood ratio were 2.5 and 0.42, respectively. On the other hand, the CPF for identifying the aspiration risk was 190 L/min, with a sensitivity of 82.6% and a specificity of 69.4%, and when the CPF cutoff value was considered as 190 L/min, the positive likelihood ratio and negative likelihood ratio were 2.7 and 0.25, respectively (Table 2). The positive likelihood ratio of CPF was similar to that of RSST results, but both values were low. Meanwhile, the negative likelihood ratio of CPF was superior to that of the RSST results. In addition, when the reference values were set at an RSST cutoff value of 2.5 swallows and a CPF cutoff value of 190 L/min (even when the RSST value was < 2.5 swallows), 23.2% of the subjects scored < 7 points in the FEES, which is considered to indicate unrestricted oral intake. Meanwhile, when CPF was < 190 L/min, only 10.9% of the subjects scored < 7 points in the FEES, which is considered to indicate unrestricted oral intake.

Receiver operating characteristic curve to predict swallowing function by the repetitive saliva swallowing test.
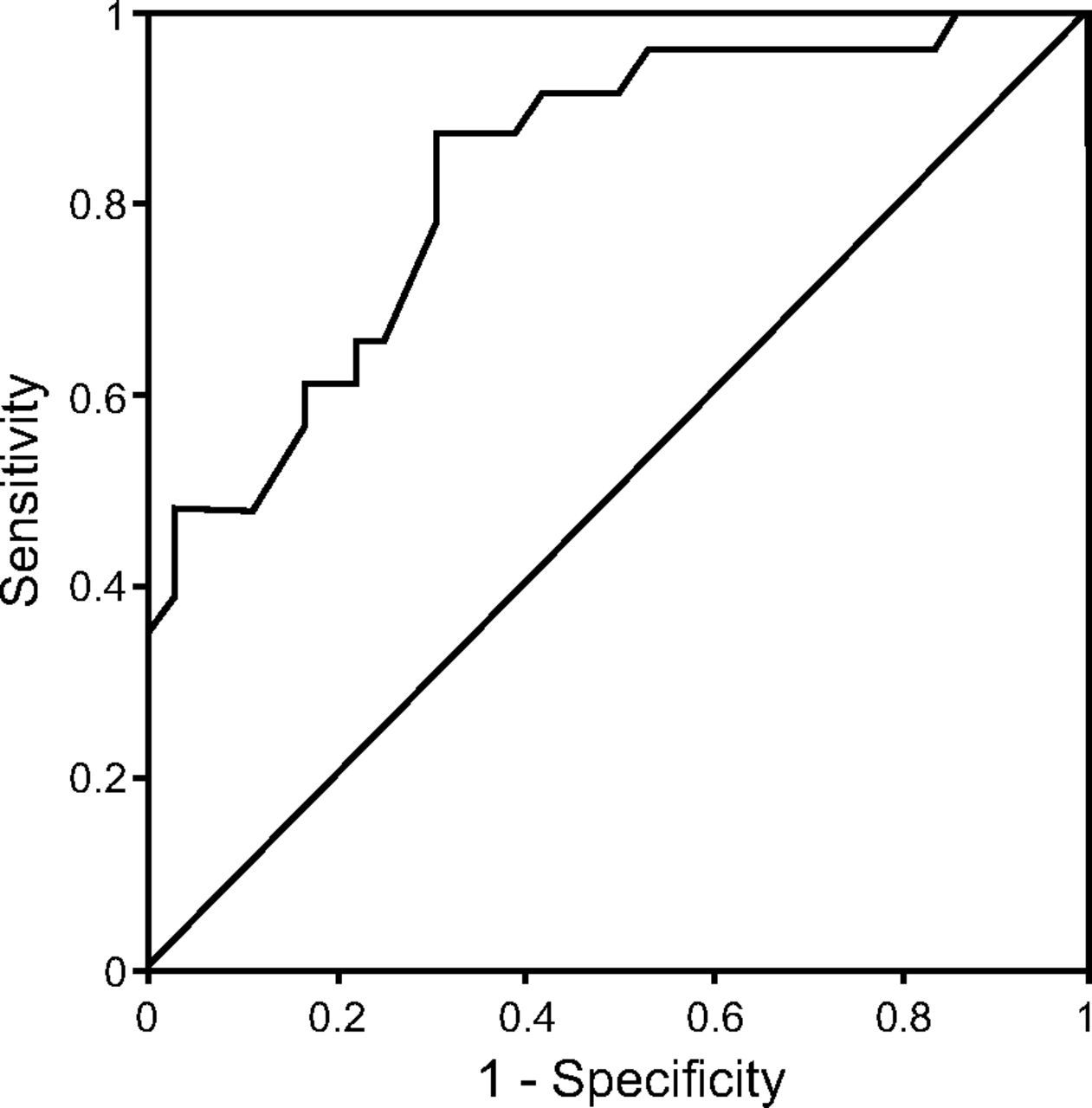
Receiver operating characteristic curve to predict swallowing function by cough peak flow.
Cut-off Values, Sensitivity, Specificity, Positive Likelihood Ratio, Negative Likelihood Ratio and AUC of RSST and CPF Value for Identifying the Aspiration Risk
Discussion
CPF and Respiratory Function in the Unrestricted and Restricted Oral Intake Groups
The general clinical symptoms of CAP include cough, fever, chills, fatigue, dyspnea, and chest pain from pleurisy.27 Our results indicated that CPF in the restricted oral intake group was far below the 240–270 L/min cutoff value for individuals capable of self-expectoration.22,28 In addition, CPF in the unrestricted oral intake group was below the cutoff value for individuals capable of self-expectoration. It has been reported that a decline in CPF is related not only to respiratory function but also to a decreased FIM,29 suggesting that a decreased FIM is another possible reason for CPF decline, in addition to respiratory function. Therefore, we believe that the low CPF values in both groups might have been affected by the higher age of subjects in our study compared with the age of subjects in previous studies22,28 and a decreased FIM due to the residual clinical symptoms of CAP.
The cough mechanism involves the following 3 phases: phase 1, inspiration; phase 2, compression; and phase 3, expulsion.30 % VC is related to phase 1 (inspiration), and % FEV1 is related to phase 3 (expulsion)31; therefore, both % VC and % FEV1 are related to cough strength. CPF is a useful predictive factor of the risk of pulmonary complications in patients with dysphagia.8 In our study, % VC was lower in both groups than the age-related reference value, and CPF was lower than the values reported in previous studies.22,28 Therefore, we believe that both groups had many elderly subjects with low foreign object expulsion ability and insufficient maintenance of airway clearance when swallowing, (ie, a potential aspiration pneumonia risk).
Cutoff Values and Sensitivity/Specificity of RSST Results and CPF
Cough is important for removing intratracheal secretions and foreign objects and for improving pharyngeal clearance; thus, cough strength is related to the onset of aspiration pneumonia.32 The fact that voluntary cough strength in stroke subjects with dysphagia is related to pneumonia onset5 and that decreased voluntary cough strength represents a high risk of aspiration6,7 shows the importance of evaluating cough strength. The CPF cutoff value that represents self-expectoration ability has been reported to be 240–270 L/min, and subjects with CPF values above this cutoff are considered to be able to expel intratracheal secretions and foreign objects.22,28 In this study, we used a CPF cutoff value of 190 L/min, which is below the value reported in previous studies, because CPF was used only to evaluate the risk of aspiration and not expectoration ability. In addition, previous studies required an expulsion ability higher than that indicated by the CPF cutoff value in our study because these studies evaluated the usefulness of CPF according to sputum expiration. In our study, when the RSST value in elderly subjects with CAP was < 2.5 swallows, 23.2% of the subjects scored < 7 points in the FEES (considered to indicate unrestricted oral intake). Meanwhile, when CPF was < 190 L/min, 10.9% of the subjects scored < 7 points in the FEES (considered to indicate unrestricted oral intake). Most of the cases of CAP in elderly subjects in this study were believed to have developed because of aspiration because most cases of CAP and health care–associated pneumonia in elderly patients are associated with aspiration pneumonia.3 Currently, no standard exists for the timing of oral intake restart in a patient who has risks, such as aspiration and asphyxiation. With regard to the clinical importance of the CPF cutoff value identified in this study, a CPF value of ≥ 190 L/min might be useful as an indicator for restarting oral intake in elderly patients considered to have aspiration-related CAP according to a swallowing test. Therefore, CPF evaluation might allow food intake to be reconsidered early in many elderly patients with CAP.
In this study, the RSST sensitivity, specificity, and area under the curve resembled previously reported values.15 Among swallowing screening tests for patients with acute pneumonia, the RSST (once or more every 30 s) has been reported to be the most useful test for determining whether to restart food intake.15 The CPF sensitivity, specificity, and area under the curve for evaluating the risk of aspiration when restarting food intake were similar to the RSST values, and there was no significant difference especially for the area under the curve (P = .42), which suggests that the precision of CPF is not inferior to that of the RSST, which is a conventional swallowing screening test. The sensitivity, specificity, and area under the curve might have been similar between CPF and the RSST because the glottic closure is involved in both CPF and the RSST. Considering FEES end points, a swallow function test includes parameters that show glottic closure, which affects the compression phase of coughing,19 and is believed to be involved in RSST. Glottic closure by air stacking in the subjects included in this study was also reflected during the CPF evaluation. From an anatomical perspective, commonly functioning organs and movements, such as pharyngeal muscle group movements for closing the nasopharynx and adductor muscle movements of the vocal cord for closing the glottis, are believed to be involved in swallowing and coughing. This might explain why the sensitivity, specificity, and area under the curve of the RSST and CPF are similar. However, the RSST does not adequately detect micro-aspiration or silent aspiration; thus, it is important to identify the presence of the coughing reflex and the cough strength required for expelling aspirated foreign objects.16 Additionally, considering that CPF reflects not only sputum expectoration ability but also glottis closure function by air stacking, evaluations that include CPF should be performed as part of the effort to avoid aspiration risk. It is important to note that, because the positive likelihood ratio for CPF was low, CPF should only be used together with swallowing screening tests as part of the approach to determine the aspiration risk.
For restarting food intake early and safely in elderly patients with CAP, CPF evaluation in addition to the RSST will provide the most appropriate approach to assess the aspiration risk. Evaluations that include CPF, which reflects not only sputum expectoration ability but also glottis closure function by air stacking, are preferred. Furthermore, as CPF can be used to quantitatively evaluate cough strength, CPF evaluation is required when assessing the current status and the efficacy of physical therapy.
Study Limitations
Glottic closure function is involved in both cough strength and swallowing function, and the interactions can be physiologically explained. However, the degree to which glottic closure function affects coughing force and swallowing ability is unclear, so further studies are needed in the future. In addition, because the mechanism of coughing is complex and the airway obstruction is verified by % FEV1, it would be important to verify the strength of the expiratory musculature, especially of the abdomen.
We should have excluded patients with a history of smoking and those with a diagnosis of obstructive or restrictive diseases, given that CPF and % FEV1 may be reduced in subjects with respiratory conditions. Our study did not evaluate the sputum expectoration status. Finally, because this was a cross-sectional study with no follow-up, no investigation was performed to assess whether CPF at the time that food intake is restarted affects the subsequent morbidity of pneumonia. Therefore, a follow-up study should be performed to assess whether CPF affects the morbidity of pneumonia.
Conclusions
Cough strength assessed with CPF is an indicator of aspiration risk when restarting food intake in elderly subjects with CAP. CPF evaluation has high sensitivity, specificity, and area under the curve, indicating that it is not inferior to the RSST for evaluating aspiration risk when restarting food intake. Although CPF is a required parameter along with RSST results when evaluating aspiration risk, in elderly patients with CAP that is not considered to be associated with aspiration according to the RSST, CPF evaluation provides a different perspective that is important when assessing the aspiration risk.
Acknowledgments
We thank Mr Ohira and Mr Yokokawa. We also thank Editage (www.editage.jp) for English language editing.
Footnotes
- Correspondence: Yasunari Sakai MSc, Department of Rehabilitation, Shinshu University Hospital, 3-1-1 Asahi, Matsumoto-shi, Nagano 390-8621, Japan. E-mail: yasunari_sakai1028{at}yahoo.co.jp.
The authors have disclosed no conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}