

Abstract
BACKGROUND: The majority of prescriptions for supplemental oxygen are written when patients are discharged to home from the hospital and the evaluation of these patients is inconsistent. Respiratory Therapists receive training in the evaluation and management of patients needing oxygen. The primary goal of the study was to estimate the frequency with which respiratory therapists (RTs) evaluate the need for home oxygen in patients hospitalized for COPD exacerbations before discharge.
METHODS: An online questionnaire was distributed to RTs in the United States by the American Association for Respiratory Care. RTs were asked to indicate how frequently they evaluate the need for home oxygen on an ordinal scale: Never, Rarely/occasionally, Sometimes, Most of the time, Almost every time, or Every time. Consistent evaluation for home oxygen was defined as performing an evaluation for home oxygen therapy Almost every time or Every time (ie, > 75% of the time). Bivariate and multivariable analyses were assessed using the Fisher exact test and logistic regression models.
RESULTS: Of 611 respondents, 490 were eligible for analysis. Fifty-eight percent of RTs reported consistently evaluating patients for home oxygen at rest, whereas 43% reported doing so during activity and 14% during sleep. Consistent evaluation for home oxygen requirements at rest was significantly associated with more years of practice (P = .03; highest among RTs with ≥ 30 y of practice at 40%), region of practice (P = .001; highest in the Midwest at 44%), and greater familiarity with criteria for home oxygen (P < .001; highest among RTs who selected Very familiar with guidelines from the Centers for Medicare and Medicaid Services at 58%). Practice in the Midwest and greater familiarity with criteria for home oxygen was associated with consistent evaluation for home oxygen during activity. Practice in the Midwest (vs Northeast; adjusted odds ratio 2.56, P < .001) and being very familiar with home oxygen criteria (vs not at all familiar; adjusted odds ratio 5.66, P < .001) were independently associated with a higher odds of evaluating for home oxygen at rest and with activity. Only 25% of RTs were involved in making decisions about home oxygen equipment.
CONCLUSIONS: RTs do not consistently evaluate patients hospitalized for COPD exacerbations for home oxygen prior to discharge, and only a minority of RTs are involved in selecting home oxygen equipment.
- home oxygen
- home oxygen evaluation
- COPD
- COPD exacerbation
- respiratory therapist
- hospital to home transition
Introduction
COPD is a common respiratory disorder that affects 15 million individuals in the United States. COPD is the fourth leading cause of death in the world and is projected to be the third leading cause of death by 2020 (https://goldcopd.org, Accessed July 5, 2020). The majority of prescriptions for supplemental oxygen are written when patients are discharged to home (ie, home oxygen) following an acute cardiopulmonary illness, rather than in the out-patient setting.1,2 However, a recent study in subjects hospitalized for COPD exacerbations suggests that the evaluation of patients for home oxygen is inconsistent.3 Moreover, patients with COPD report various concerns about home oxygen therapy following hospitalization, including malfunctioning oxygen equipment, lack of education about the use of the equipment, and inadequate access to appropriate home oxygen equipment.4
Respiratory therapists (RTs) receive training in the evaluation and management of patients with COPD and other lung disorders (https://www.aarc.org, Accessed July 5, 2020).5 The American Association for Respiratory Care (AARC), the largest professional organization for RTs in the United States, estimates that there are > 170,000 RTs in the United States alone, working primarily in hospitals and other acute care settings. However, the role of RTs in the evaluation for home oxygen before discharge in patients hospitalized for COPD has not been studied. This study was commissioned by the AARC as part of its efforts to support the U.S. COPD National Action Plan, the first-ever framework for action to reduce the public health impact of COPD in the United States (https://www.aarc.org/copd-national-action-plan, Accessed July 5, 2020).
The primary goal of the Home Oxygen Evaluation by Respiratory Therapists in Patients Hospitalized for COPD Exacerbations (RIsOTTO) Study was to estimate the frequency with which RTs evaluate the need for home oxygen in patients hospitalized for COPD exacerbations at the time of transition from hospital to home. Secondary goals included identification of RT characteristics associated with consistent evaluation for home oxygen therapy and decision makers of selecting home oxygen equipment.
QUICK LOOK
Current knowledge
Home oxygen therapy is a significant burden, and the evaluation for home oxygen needs in patients hospitalized with COPD is not adequate. The role of respiratory therapists (RTs) in assessing home oxygen needs prior to hospital discharge in patients hospitalized with COPD has not been studied.
What this paper contributes to our knowledge
A cross-sectional study among RTs who are members of the AARC indicates that RTs do not consistently evaluate home oxygen needs in hospitalized patients with COPD and are rarely involved in selecting home oxygen equipment at the time of hospital-to-home transition. Less than half of surveyed RTs (42%) were very familiar with the Centers for Medicare and Medicaid Services criteria for home oxygen.
Methods
Study Population
The AARC invited its RT membership to participate in the RIsOTTO study. Questionnaire respondents were eligible to participate in the study if they were respiratory therapists, provided care for patients hospitalized for COPD exacerbations, worked in acute care settings, and practiced in the United States. Respondents did not receive compensation for participation in the study. The study was considered exempt from human subjects review by the Institutional Review Boards at the University of Illinois at Chicago (#2016-0936) and Rush University Medical Center in Chicago (#16112301-IRB01).
Questionnaire Domains
The study questionnaire included 3 domains: characteristics of RTs, evaluation for home oxygen therapy, and selection of home oxygen equipment. The questionnaire can be viewed in the supplementary materials at http://www.rcjournal.com.
Characteristics of RTs.
Based on the AARC Human Resource Study (https://www.aarc.org/resources/tools-software/aarc-respiratory-therapist-human-resource-study-2014/ Accessed November 5, 2020), respondents were asked to report their highest level of formal education (associate’s degree, bachelor’s degree, master’s degree, PhD, or other); credentials (registered respiratory therapist, certified respiratory therapist, certified pulmonary function technologist, registered pulmonary function technologist, other); years of practice (ie, < 10 y, 10–19 y, 20–29 y, or ≥ 30 y); and practice location (ie, name of state). We also asked respondents to report their degree of familiarity with U.S. Centers for Medicare and Medicaid Services (CMS) criteria for home oxygen (ie, Very, Somewhat, Not at all familiar; https://www.cms.gov/medicare-coverage-database/details/ncd-details.aspx?NCDId=169, Accessed July 5, 2020).
Evaluation for Home Oxygen.
In the United States, CMS criteria for coverage of home oxygen include the presence of severe lung disease or hypoxia-related symptoms that might be expected to improve with oxygen therapy; qualifying room air arterial blood gas or  results at rest, during activity, or during sleep; and that these clinical tests be obtained no earlier than 2 d prior to hospital discharge.6 We therefore asked RTs to report the frequency with which they evaluated patients hospitalized for COPD exacerbations for home oxygen according to these CMS criteria: Never, Rarely/occasionally (ie, 1–25% of the time), Sometimes (ie, 26–50% of the time), Most of the time (ie, 51–75% of the time), Almost every time (ie, 76–95% of the time), or Every time (> 95% of the time). The question was repeated 3 times to assess the frequency of evaluation at rest, during activity, and during sleep.
results at rest, during activity, or during sleep; and that these clinical tests be obtained no earlier than 2 d prior to hospital discharge.6 We therefore asked RTs to report the frequency with which they evaluated patients hospitalized for COPD exacerbations for home oxygen according to these CMS criteria: Never, Rarely/occasionally (ie, 1–25% of the time), Sometimes (ie, 26–50% of the time), Most of the time (ie, 51–75% of the time), Almost every time (ie, 76–95% of the time), or Every time (> 95% of the time). The question was repeated 3 times to assess the frequency of evaluation at rest, during activity, and during sleep.
Selection of Home Oxygen Equipment.
RTs were asked to identify individuals in their institution who make decisions regarding selection of types of home oxygen equipment; options included RT, registered nurse, social worker, physician, durable medical equipment company, I do not know, and Other). Respondents had the option to select > 1 of these categories.
Questionnaire Administration
The RIsOTTO questionnaire was piloted among 4 RTs at 1 institution and reviewed for content and clarity prior to data collection. The AARC sent a newsletter via e-mail to all members in October 2016 with an invitation that included a link to the online questionnaire (SurveyMonkey, San Mateo, California). Two reminder e-mails were sent 2 and 5 weeks after the initial e-mail. The questionnaire was closed in February 2017. Response rate was determined by counting unique internet provider addresses, with duplicate addresses removed before analysis. The results of the pilot questions were not included in the final analyses.
Analysis
Responses were expressed as a frequency and proportion of participants. In the analyses, we combined some response options to simplify interpretation. For the characteristics of RTs, we presented the highest level of education as bachelor’s degree or higher versus less than bachelor’s degree, and credentials as registered respiratory therapist, certified respiratory therapist, or other. Responses regarding the state in which RTs practiced were re-classified into regions (ie, Midwest, Northeast, South, or West), as defined by the U.S. Census Bureau (https://www2.census.gov/geo/pdfs/maps-data/maps/reference/us_regdiv, Accessed July 5, 2020). If participants listed more than one state in their answer, they were assigned to the U.S. region of the first state listed. Differences in RT characteristics between respondents from the Midwest and other U.S. regions (ie, Northeast, South, or West) were evaluated with chi-square tests. The frequency of evaluation for home oxygen was presented as a dichotomous variable, defined as consistently (> 75% of the time) versus not consistently.
We examined the association between baseline characteristics of RTs and the frequency of consistent evaluation for home oxygen in bivariate (Fisher exact tests) and multivariate (logistic regression models) analyses. RT characteristics that were significantly (P < .05) associated with evaluation for home oxygen in bivariate analyses were included in the multivariate logistic regression models to identify independent predictors of consistent evaluation. These results were presented as adjusted odds ratios with 95% CIs. A 2-sided P value < .05 was used to define a statistically significant difference. Analyses were performed using Stata 14 (StataCorp, College Station, Texas) and SAS 9.4 (SAS Institute, Cary, North Carolina).
Results
RT Characteristics
Of 611 respondents, 490 (79%) were included in the analyses. Four duplicate responses (based on internet provider addresses) were excluded. The most common reasons for ineligibility were not working in acute care settings (n = 51, 8%) and not providing care for patients hospitalized for COPD (n = 47, 8%; see the supplementary materials at http://www.rcjournal.com). The study participants were recruited from 49 of 50 states in the United States (see the supplementary materials at http://www.rcjournal.com).
Just over half (53%) of RTs had a bachelor’s degree or higher (Table 1). A majority (85%) were credentialed as registered respiratory therapists. More than a third (36%) of RTs had at least 30 y of work experience. RTs worked in all regions in the United States, most commonly in the Midwest (36%) and least commonly in the West (17%). Only 2 participants reported that they practiced in > 1 state in different U.S. regions. There were no significant differences between RTs from the Midwest compared to the other U.S. regions with regard to education, credentials, years of practice, or familiarity with the CMS home oxygen criteria (see the supplementary materials at http://www.rcjournal.com). Fewer than half (42%) of all RTs reported being very familiar with CMS criteria for home oxygen.
Respondent Characteristics
Evaluation for Home Oxygen Associated With RT Characteristics
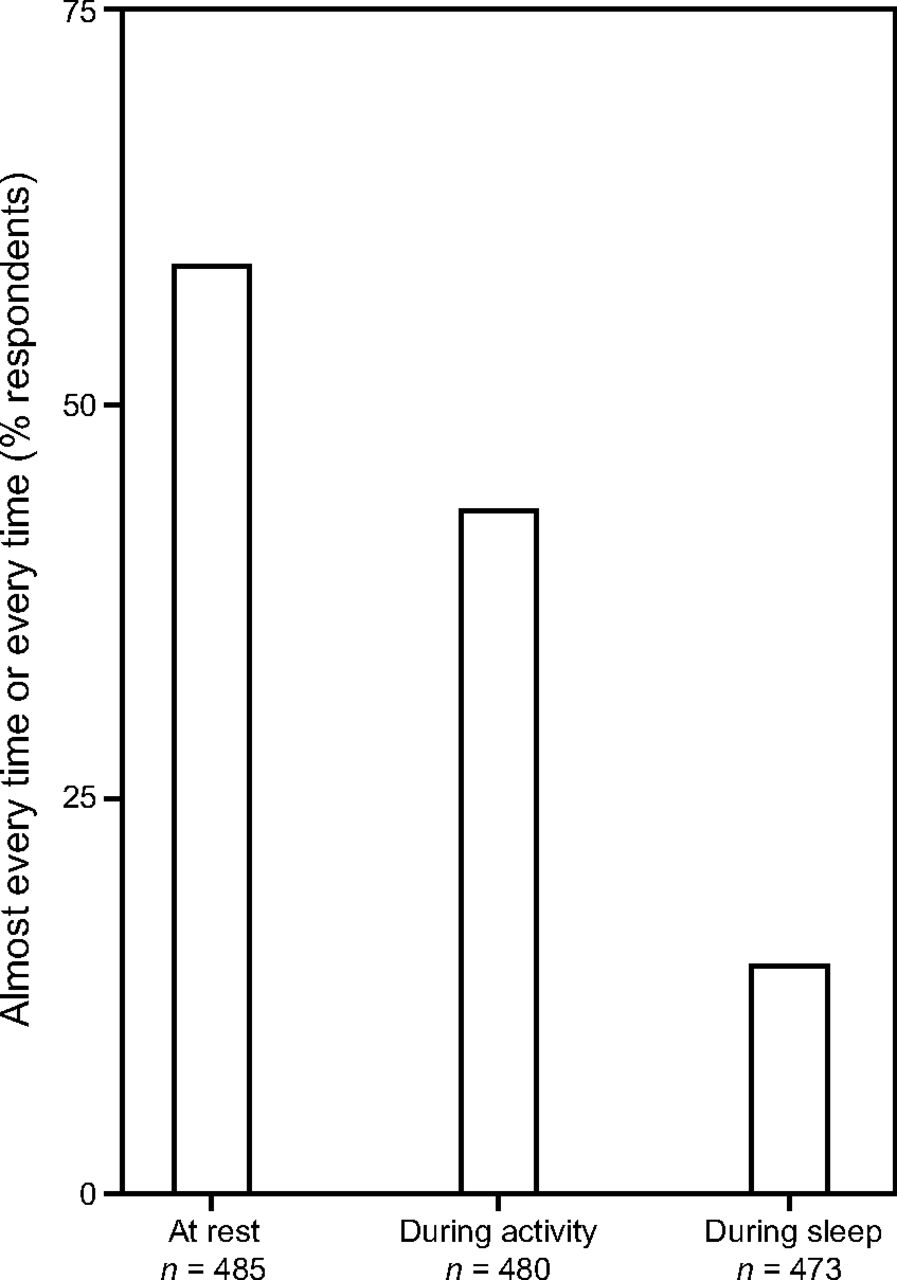
RTs indicated that they consistently (ie, > 75% of the time) performed evaluation for the need of home oxygen in patients in the 48 h prior to hospital discharge in just over half (58%) of patients at rest and in a minority of patients during activity or sleep (43% and 14%, respectively; Fig. 1).

Respiratory therapist responses as to how consistently they evaluate the need for home oxygen therapy before patient discharge. Also shown are the number of respondents who answered in each patient evaluation scenario (at rest, during activity, and during sleep; N = 490).
In bivariate analyses, consistent evaluation for home oxygen at rest was significantly associated with more years of practice (P = .03), region of practice (P = .001; highest in the Midwest), and greater familiarity with CMS home oxygen criteria (P < .001) (Table 2). A similar pattern was noted for RT characteristics associated with consistent evaluation with activity, but there was no significant association with the number of years of practice (P = .10). None of the RT characteristics we examined were associated with consistent evaluation during sleep.
Consistent Evaluation for Home Oxygen and Association With RT Characteristics
Multivariable analyses indicate that practice in the Midwest (vs practice in the Northeast) was independently associated with higher adjusted odds ratios of consistently evaluating for home oxygen at rest and during activity of 2.56 (95% CI 1.43–4.58, P = .001) and 2.52 (95% CI 1.42–4.50, P = .002), respectively (Figure 2). Similarly, being very familiar with CMS home oxygen criteria (vs not at all familiar) was associated with higher adjusted odds of consistently evaluating the need for home oxygen at rest and during activity, but not during sleep (adjusted odds ratio 5.66 [95% CI 2.56–12.48, P < .001], 5.37 [95% CI 2.20–13.10, P < .001], and 2.26 [95% CI 0.73–7.01, P = .16], respectively).

Forest plot. Multivariable analyses adjusted for years of practice, region of practice, and familiarity with CMS home oxygen criteria. Results of these analyses indicate that practice in the Midwest (vs. practice in the Northeast) and being Very familiar with CMS criteria for home oxygen (vs. Not at all familiar) were independently associated with higher odds of consistently evaluating for home oxygen at rest and with activity. CMS = Centers for Medicare and Medicaid Services.
Selection of Home Oxygen Equipment
Only 25% of RTs reported being involved in selecting the home oxygen equipment for patients before discharge, including 3% reporting joint decisions with physicians and 3% reporting joint decisions with others (Figure 3). In 18% of cases, respondents indicated that durable medical equipment companies made decisions about home oxygen equipment.

The selection of home oxygen equipment involved RTs in 25% (19% RTs, 3% RTs and physicians, 3% RTs and others). Others included alone or in combination with nurses, discharge planners, case managers, social workers, DME companies, and patients. 12.8% (63/490) of the answers were missing. RT = respiratory therapist; DME = durable medical equipment.
Discussion
In this national study of RTs conducted by the AARC, we found that RTs do not consistently evaluate patients hospitalized for COPD exacerbations for home oxygen prior to hospital discharge. RTs who practice in the Midwest and who report being very familiar with CMS criteria for home oxygen were more likely to consistently evaluate patients for home oxygen at rest and with activity. Also, only a minority of RTs are involved in selecting home oxygen equipment prior to hospital discharge.
To our knowledge, the RIsOTTO study is the first study to examine the role of RTs in assessing the need for home oxygen in patients hospitalized for COPD exacerbation. Previous studies have focused on RT practices regarding noninvasive ventilation, tracheostomy decannulation, and airway clearance.7,8 RT training requires 2–4 y of formal education at accredited respiratory therapy programs (https://www.aarc.org/education/educator-resources/find-an-accredited-respiratory-care-program, Accessed July 5, 2020) in the evaluation and management of patients with lung diseases and in the use of mechanical ventilation and associated devices and equipment (eg, nebulizers, inhalers, ventilators, oxygen equipment). RTs also play an essential role in educating patients on proper management of their home oxygen equipment. However, only 58% of RTs reported consistently (ie, > 75% of the time) evaluating hospitalized patients for home oxygen at rest, 43% during activity, and only 14% during sleep. The low proportion of RTs evaluating patients for home oxygen at rest was disappointing given the well-known survival benefits of home oxygen in patients with COPD and severe hypoxemia.9,10 Moreover, studies also suggest that supplemental oxygen improves dyspnea and exercise tolerance in patients with hypoxemia during physical activity.11-13 While it is possible that evaluation for home oxygen is performed by other clinicians besides RTs (eg, nurses, medical residents), a previous study in 2 hospitals indicates that gaps in evaluation for home oxygen are common.3 In this previous study, only 22% (73 of 335) of subjects hospitalized with COPD had an adequate evaluation for home oxygen and only 16% (54 of 335) had adequate documentation of home oxygen requirements.
Recent reports have described that clinicians feel mostly unprepared when addressing patient concerns about home oxygen therapy.4,6 In a study of 507 subjects with COPD on home oxygen therapy, subjects reported different types of home oxygen equipment (eg, stationary concentrator, portable gas tanks, oxygen-conserving device, oxygen refill system, liquid oxygen, portable concentrator).14 Participants reported one or more of these types of home oxygen equipment in 25 different combinations (eg, stationary concentrator plus gas tanks; stationary concentrator plus gas tanks with oxygen conserving device; liquid oxygen only). Home oxygen equipment should be tailored to the patient’s needs based on their need for oxygen flow (eg, 2 L/min continuously vs 4 L/min continuously), length of time they expect to be out of the home per day, and ability to lift or carry oxygen equipment. These issues can complicate the evaluation of a patient for home oxygen and providing adequate patient education about home oxygen, especially if the same home oxygen equipment is not available in the hospital setting prior to discharge.
The variability in the evaluation for home oxygen by region of practice among RTs is unexplained. Among RTs in the RIsOTTO study, education, credentials, and years of practice did not differ significantly across U.S. regions. Also, according to the AARC, training requirements do not differ significantly across the United States. Regional variation in care by physicians and nurses across the United States has been well documented and may relate to differences in reimbursement, state regulations, and other factors (https://www.dartmouthatlas.org, Accessed July 5, 2020). However, we are not aware of similar reports about regional practice variation among RTs. The factors that contribute to regional practice variation among RTs in home oxygen evaluation deserve further investigation.
There appears to be no clear explanation as to why RTs are not routinely involved in selecting home oxygen equipment. In clinical practice, RTs generally work under the direction of and together with physicians to make decisions regarding home oxygen therapy and equipment. This might explain the low reported rate of RTs as the only decision-makers for home oxygen equipment in our study. Interestingly, durable medical equipment providers were reported to be involved in selecting home oxygen equipment in nearly 20% of patients, which raises concern for possible conflicts of interest.
The lack of routine RT participation in the selection of home oxygen equipment may also be due to the lack of defined roles and responsibilities. There is increasing recognition about the importance of multidisciplinary teams, including RTs, physicians, nurses, and physical therapists, to liberate patients from ventilators.15,16 This is supported by the CMS advisory to hospitals in §482.43(b)(2) of its Interpretive Guidelines, which states that a “well-designed discharge planning evaluation uses a multidisciplinary approach […] to ensure that all of the patient’s post-discharge needs are identified” (https://www.cms.gov, Accessed July 5, 2020).
This study has 2 strengths. This is the first study to date to examine the role of RTs in the evaluation for home oxygen before discharge in patients hospitalized for COPD. The RTs in our study were recruited from almost all states in the United States and are comparable with those described in the AARC Human Resources study with regard to surveyed characteristics, therefore increasing the likelihood that our findings reflect national practice patterns of RTs who are members of the AARC.12 This study has some limitations. Respondents were all members of the AARC and self-selected to participate, and they may differ in some important ways from non-respondents or from RTs who are not members of the AARC. The data were self-reported, so we cannot exclude the possibility of social desirability bias resulting in an overestimate of reporting consistent evaluation for home oxygen. Our report also did not examine barriers and facilitators in assessing the need for home oxygen in patients hospitalized for COPD exacerbations, post-hospital care practices, nor access to home oxygen equipment.
Conclusions
Our results indicate that RTs do not consistently evaluate for home oxygen in patients hospitalized for COPD exacerbations and are rarely involved in selecting home oxygen equipment. Our study provides information that could contribute to future interventions incorporating RTs in the assessment for home oxygen needs prior to hospital discharge. Further research is needed to study multidisciplinary interventions and successful initiation of home oxygen therapy incorporating RTs at the time of the transition from hospital to home.
ACKNOWLEDGMENTS
The authors thank Hannah Nguyen MPH, and Richard Gallardo III MPH, for their assistance in data analysis as well as the staff at the executive office of the American Association for Respiratory Care for their assistance in conducting the study.
Footnotes
- Correspondence: Ai-Yui M Tan MD, Loyola University Medical Center, Division of Pulmonary and Critical Care, 2160 S 1st Ave, Maywood, IL, 60153. E-mail: Ai-Yui.Tan{at}lumc.edu
See the Related Editorial on Page 347
Dr Tan presented a version of this paper at the American Thoracic Society 2017, held May 19–24, 2017, in Washington, DC.
Supplementary material related to this paper is available at http://www.rcjournal.com.
Dr Tan has disclosed a relationship with the National Institutes of Health (NIH). Dr Krishnan has disclosed relationships with the NIH, the Patient-Centered Outcomes Research Institute, ResMed, and Regeneron. Dr Vines has disclosed a relationship with Ohio Medical. Dr Prieto-Centurion has disclosed relationships with the NIH and ResMed. Mr Kallstrom is Executive Director of the American Association for Respiratory Care and Publisher of Respiratory Care.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}