

Abstract
BACKGROUND: Pediatric noninvasive ventilation (NIV) is used commonly in the acute care setting and is associated with high incidence of patient ventilator asynchrony.
METHODS: An ASL 5000 breathing simulator was used to model pediatric patients with varying patient efforts and lung conditions. For delivery of NIV, a commonly used acute care ventilator was used by connecting a nasal cannula interface to model nares produced with a 3-dimensional printer. The modes of ventilation were NIV pressure control continuous mandatory ventilation and NIV pressure control continuous spontaneous ventilation. Patient and ventilator waveforms were analyzed using the ASL 5000 software to assess for asynchrony events and determine the asynchrony index (AI).
RESULTS: Significant asynchrony (AI > 0.1) existed in the majority of scenarios for both pressure control continuous mandatory ventilation and pressure control continuous spontaneous ventilation (79% and 93%, respectively). The most common asynchrony event was ineffective trigger, accounting for 81.9% of events in pressure control continuous mandatory ventilation and 79.3% in pressure control continuous spontaneous ventilation. There were no statistically significant differences in the AI when comparing simulated patient effort or lung condition.
CONCLUSIONS: Significant asynchrony exists during NIV with a commonly used acute care ventilator and nasal cannula interface, which raises questions regarding its utility in clinical practice in the pediatric population.
Introduction
Noninvasive ventilation (NIV) is being used more frequently in acute care settings such as the pediatric ICU.1,2 NIV has several advantages in this clinical setting, including the avoidance of invasive procedures and associated complications of invasive mechanical ventilation. Studies have reported that NIV is useful in preventing intubation,3-11 decreasing extubation failure,9,12 and decreasing patient work of breathing,3,5,6,9,11,13-15 and that it has improved survival benefits.9,10,16
Although NIV offers advantages, there are problems associated with its use. A predictor of success with NIV is patient comfort, and one determinant of patient comfort is the presence of patient-ventilator asynchrony.17 Problems with asynchrony are a well-documented issue during invasive ventilation and have been associated with adverse outcomes.18-20 Similar results have been reported when examining asynchrony during NIV. Despite a variety of interfaces available for clinical use, asynchrony persists due to the presence of air leak.8,9,11 In the pediatric population specifically, Itagaki et al21 compared the ability of various acute care ventilators to compensate for leak during NIV delivered through the RAM cannula (Neotech, Valencia, California), a nasal cannula interface. In this bench simulation study, the authors reported that leak contributed significantly to asynchrony across a range of ventilators when interfaced with neonatal and infant lung models.21
In clinical practice, the amount of leak present with a nasal cannula interface varies but is at least partially due to incomplete occlusion (by the cannula flanges) of the nares, which is recommended to avoid skin breakdown. The purpose of our study was to simulate the use of NIV delivered through a nasal cannula interface that is being used in the pediatric ICU population with increasing frequency, particularly in infants but also in some pre school age children (1–5 y old).2,22 Our study focused on the clinical aspects of patient effort and lung conditions and how these factors might contribute to asynchrony, rather than on the ventilator’s ability to compensate for the leak. The specific aim of this simulation-based study was to examine the extent of asynchrony across a range of experimental conditions representing different patient sizes, patient efforts, and lung conditions during NIV with an acute care ventilator and a nasal cannula interface.
Quick Look
Current Knowledge
Noninvasive ventilation (NIV) is being used more frequently in pediatric ICUs, and patient-ventilator asynchrony is a documented issue. Previous studies indicate that ventilators used for NIV vary in their ability to compensate for the leak present in NIV and that asynchrony increases as the leak becomes more significant.
What This Paper Contributes to Our Knowledge
This study highlights the significant asynchrony that exists with the use of a nasal cannula interface to deliver NIV in a pediatric model simulation. Instead of controlling the amount of leak, as has been done previously, this study examined the effects of lung condition and effort on asynchrony by maintaining the recommended fit for the nasal cannula interface. This study should be used to help guide future clinical studies when using a nasal cannula interface to deliver NIV, as well as raise clinicians’ awareness to the degree of asynchrony at the bedside and how this may contribute to the NIV success or failure.
Methods
Study Design
This simulation-based study was conducted at the Cleveland Clinic Foundation (Cleveland, Ohio) using an ASL 5000 breathing simulator (IngMar Medical, software version 3.6) and a Servo-i (Getinge, Gothenburg, Sweden) acute care ventilator in the noninvasive modes classified as pressure control continuous mandatory ventilation and pressure control continuous spontaneous ventilation.23 A set of model nares produced with a 3-dimensional printer was attached to the ASL 5000 to simulate patient nares; these models were designed for the RAM nasal cannula interface to occlude approximately 75% of the nares (manufacturer recommends 60–80% occlusion). Three sizes of the nasal cannula interface were then attached to the model nares and connected to the ventilator. The ASL 5000 was programmed for 3 lung models (ie, normal, obstructive, and restrictive) based on existing data (see ASL 5000 Model Setup). Ventilator settings are discussed separately; however, all experiments were conducted without a humidifier. A neonatal patient circuit was used for the newborn model, and a pediatric circuit was used for the small and large models. A ventilator check was performed prior to each simulation. The model nares and nasal cannula interface were connected to the simulator and then the interface to the ventilator (Fig. 1).

Model setup. The model nares (A) were attached to the nasal cannula interface (B), which was connected directly to the ASL 5000 breathing simulator (C). The nasal cannula interface was then attached to the acute care ventilator.
ASL 5000 Model Setup
For this study, patient sizes were represented by using 3 sizes of the nasal cannula interface: newborn, small, and large. The lung models were normal, restrictive, and obstructive, based on examination of data from previous studies.21,24-26
For each patient size, 3 effort models were used to represent active inspiration. The modes are composed of a sinusoidal function for muscle pressure (Pmus) having the parameters of frequency, amplitude (Pmax), increasing effort (% increase), inspiratory hold (% hold), and relaxing effort (% release), where the percentage represents duration as a fraction of the ventilatory period. These were adjusted to simulate unsupported tidal volumes of 4 mL/kg (low effort, P1), 7 mL/kg (medium effort, P2), and 10 mL/kg (high effort, P3). Spontaneous breathing rates were adjusted to simulate physiologic rates appropriate for the simulated patient size and lung condition. The same lung models and effort models were used for both pressure control continuous mandatory ventilation and pressure control continuous spontaneous ventilation. The model parameters for all scenarios are shown in Table 1.
ASL 5000 Breathing Simulator Model Setup
Ventilator Settings
The acute care ventilator used in this study was the Servo-i. The noninvasive modes used were pressure control continuous mandatory ventilation and pressure control continuous spontaneous ventilation. Specific ventilator settings are shown in Table 2. In the noninvasive mode of the Servo-i, the ventilator uses an internal leak compensation algorithm; thus the trigger sensitivity cannot be set. Ventilation was initiated after 5 patient breaths, and the model continued for a total of 50 breaths for each scenario.
Ventilator Settings
Data Acquisition and Analysis
Using the ASL 5000 breathing simulator’s Post-Run Analysis software, the waveforms of 10 breaths were analyzed to identify asynchrony events. The Pmus (ie, simulated patient effort) and flow (ie, ventilator flow detected by the ASL 5000) waveforms were used to evaluate asynchrony by calculating trigger and cycle phase differences as previously described.27 Asynchrony was classified into trigger and cycle events. These were further delineated as ineffective trigger, early trigger, late trigger, early cycle, and late cycle:

Where Ventflow, start is the point at which ventilator flow began, [SoE]Pmus(t0) is the point at which the simulated patient began, Tinsp, patient is the inspiratory time of the simulated patient, Ventflow, end is the point at which ventilator flow ended, Pmus(peak) is peak simulated patient effort, and Texp(patient) is the simulated patient expiratory time (Table 3).
Definitions of Patient-Ventilator Asynchrony Error
An asynchrony index (AI) was then calculated by totaling the number of asynchrony events and dividing by the number breaths over which those events occurred:  , where IT = ineffective trigger, ET = early trigger, LT = late trigger, EC = early cycle, and LC = late cycle. An AI > 0.10 (10%) was considered clinically important, consistent with existing literature.8,17,19,21,28-30
, where IT = ineffective trigger, ET = early trigger, LT = late trigger, EC = early cycle, and LC = late cycle. An AI > 0.10 (10%) was considered clinically important, consistent with existing literature.8,17,19,21,28-30
Statistical Analysis
The Kruskal-Wallis test was used to compare AI among Pmax and lung condition groups. We further used the Dwass, Steel, Critchlow-Fligner (DSCF) method for pairwise multiple comparison. To assess the association between Pmax setting and AI under each setting of cannula size and lung condition, the data were analyzed using a multiple linear regression model with AI as a dependent variable and Pmax, cannula size, and lung condition as covariates; a negative slope in the linear regression model suggests a decreasing AI with increasing Pmax. The size–condition interaction, size–Pmax interaction, condition–Pmax interaction, and the size–condition–Pmax interaction were also included. Pmax was treated as a continuous variable, whereas cannula size and lung condition as categorical variables. All tests were 2-tailed and performed at a significance level of .05. SAS 9.4 (SAS Institute, Cary, North Carolina) was used for all analyses and plots.
Results
Clinically important AI (> 0.10) was observed in the majority of scenarios during both pressure control continuous mandatory ventilation (78.8%) and pressure control continuous spontaneous ventilation (92.6%) NIV with a nasal cannula interface. The most common type of asynchrony regardless of NIV mode was ineffective trigger, with 81.9% of error in pressure control continuous mandatory ventilation and 79.3% in pressure control continuous spontaneous ventilation. Cycle errors were rare, and there were no early cycle errors in any of the simulated scenarios (Table 4).
Total Model Patient-Ventilator Asynchrony Events for PC-CMV and PC-CSV
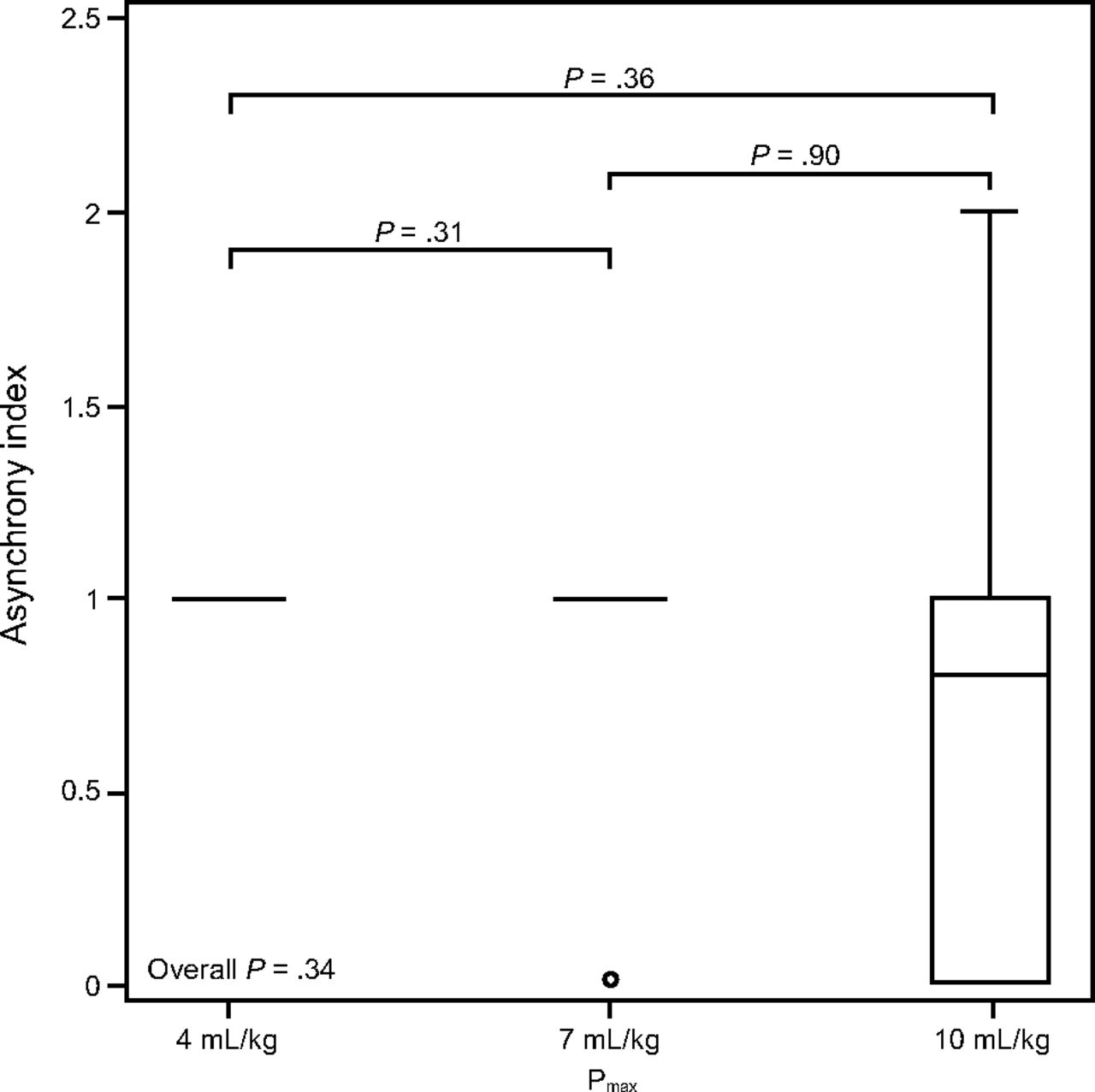
For the pressure control continuous mandatory ventilation mode, the AI ranged from 0.0 to 2.0 with a mean of 0.82. In the pressure control continuous spontaneous ventilation mode, AI ranged from 0.0 to 1.1 with a mean of 0.93. For both pressure control continuous mandatory ventilation and pressure control continuous spontaneous ventilation modes of NIV, there was no difference of the AI between different simulated inspiratory efforts or lung condition across all scenarios (Figs. 2–5).

Comparison of asynchrony index by lung conditions for pressure control continuous mandatory ventilation. Overall P value was obtained with the Kruskal-Wallis test; P values above boxplots were obtained with pairwise 2-sided multiple comparison analysis, with lines below indicating the targets of comparison.

Comparison of asynchrony index by simulated patient effort for pressure control continuous mandatory ventilation. Overall P value below boxplots was obtained with the Kruskal-Wallis test; P values above boxplots were obtained with pairwise 2-sided multiple comparison analysis, with lines below indicating the targets of comparison. Pmax = simulated patient effort (Pmus) to obtain different tidal volumes as listed.

Comparison of asynchrony index by lung condition for pressure control continuous spontaneous ventilation. Overall P value was obtained with the Kruskal-Wallis test; P values above boxplots were obtained with pairwise 2-sided multiple comparison analysis, with lines below indicating the targets of comparison.

Comparison of asynchrony index by simulated patient effort for pressure control continuous spontaneous ventilation. Overall P value was obtained with the Kruskal-Wallis test; P values above boxplots were obtained with pairwise 2-sided multiple comparison analysis, with lines below indicating the targets of comparison. Pmax = simulated patient effort (Pmus) to obtain different tidal volumes as listed.
There were no consistent trends of AI regarding changes in the simulated patient effort in either pressure control continuous mandatory ventilation (Table 5) or pressure control continuous spontaneous ventilation (Table 6).
Estimates for the Slope of Pmax for Each Group During PC-CMV
Estimates for the Slope of Pmax for Each Group During PC-CSV
Discussion
The nasal cannula interface is an option for delivery of NIV in the critically ill pediatric population and is currently being used in pediatric ICUs with reports of use primarily in infants but also in preschool and school-age children.2,22 The results of our study indicate that significant asynchrony exists during NIV when using an acute care ventilator and a nasal cannula interface in simulated pediatric patient models. Importantly, this was discovered using the clinically recommended nasal cannula fitting, which has not been done in similar studies. This error in synchrony held across a range of simulated patient sizes, patient efforts, and lung conditions. The substantial asynchrony encountered with our model, and the association of asynchrony with adverse outcomes, may suggest limited clinical utility of NIV with a nasal cannula interface as a therapy for spontaneously breathing critically ill pediatric patients.
Children admitted to the pediatric ICU often require invasive mechanical ventilation, exceeding 50% of cases in some reports.28,30 Despite abundant use of mechanical ventilation, optimizing synchrony remains a problem. Blokpoel et al20 reported that asynchrony was common in children receiving invasive mechanical ventilation, with ineffective trigger being the predominant type of asynchrony error. Their group noted that problems with synchrony occurred in all subjects, and that 80% had a significant AI > 0.1. Mortamet et al31 reported similar results in a single-center prospective study using diaphragmatic electrical activity via a neurally-adjusted ventilatory assist catheter to evaluate for asynchrony. This group noted a median AI of 0.25 with nearly all (97%) of subjects exhibiting an AI > 0.1. Poor synchrony contributes to prolonged use of invasive mechanical ventilation, increased ICU and hospital length of stay, and decreased 28-d ventilator-free survival.18,19,32 In addition, a trend toward increased mortality has been reported when significant asynchrony exists.19
NIV is being used more frequently in acute care settings with several beneficial effects.3-5,7,9,14,16 The evidence in pediatrics for NIV is not as robust as the adult literature but has yielded similar results.3-7,11,15,33 Despite its known advantages, NIV failure is associated with undesirable consequences. Ganu and colleagues reported that NIV failure was associated with prolonged use of invasive mechanical ventilation as well as an increase in length of pediatric ICU stay.7 Additionally, up to 16% of patients receiving NIV progress to invasive mechanical ventilation, and this failure may be associated with increased mortality.8
A documented predictor of NIV failure is the presence of asynchrony which is common, occurring in > 40% of patients receiving NIV. Although there is a growing body of evidence associating asynchrony with undesirable outcomes, little clinical evidence to this effect has been published in the pediatric literature. While not the sole cause of failure, the degree of asynchrony must be considered when applying NIV. Given our results, along with those of other bench and clinical studies, which suggest a high incidence of asynchrony during NIV, the use of a nasal cannula interface to deliver NIV should be exercised with caution and requires further clinical investigation.
The AI has been used extensively in the literature as a measure of patient-ventilator interaction; however, its use as an accurate reflection of this interaction can be challenged. Our results indicate that the majority of asynchrony events are failed trigger efforts, consistent with previous bench and clinical data from the literature. These events are the result of complete lack of patient-ventilator interaction throughout the respiratory cycle. Failed trigger efforts are an example of complete or true asynchrony (ie, 1 of 2 signals, inspiratory pressure, is missing the presence of the other, patient effort).34 Other errors in trigger and cycle events may be more properly described as dyssynchronous events (ie, 2 signals present but out of phase). Giving equal weight to ineffective trigger (true asynchrony) and other trigger and cycle events (dyssynchrony) undermines the qualitative difference between a complete lack of patient-ventilator interaction versus a less optimized interaction.
Sinderby et al27 described an objective approach to defining synchrony, dyssynchrony, and asynchrony. The authors defined synchronization windows during which a trigger or cycle event can occur and be considered synchronous. Using this methodology, they described trigger and cycle phase differences to classify asynchrony, which we used in our study to define error events (Fig. 6). Classification of asynchrony is important for aforementioned reasons. In our study, we found the AI to be significant in nearly all scenarios; however, because of its current definition, we may still be underestimating the significance of asynchrony when using this interface.

Graphical depiction of trigger and cycle windows, as well as the start and end of ventilator flow, used to calculate patient-ventilator synchrony error events.
We found no statistically significant trend among the AI with changes in patient effort. However, increasing simulated patient efforts yielded linear regression models with mostly negative slopes, suggesting an important trend (Tables 5 and 6). This is possibly due to increased patient effort causing an increased flow that overcomes the presence of a leak and is recognized by the ventilator. This hypothesis merits further investigation.
The results of our study should be interpreted considering the following limitations. First, this is a bench simulation project, so the direct applicability to clinical practice could be challenged. However, several studies have validated the use of simulation-based models with clinical data.17,24,25,30,35 For example, Carteux et al30 examined NIV in a simulated and clinical environment with the primary objective of assessing several ventilators’ ability to compensate for leaks in the system; they reported similar results during the bench and clinical portions of their study. Dexter et al24 validated the use of the ASL 5000 breathing simulator using respiratory mechanics taken from the pediatric literature. By using the manufactured and clinically recommended nares-cannula occlusion criteria and using a variety of patient efforts for different lung conditions, we simulated changes in patient conditions and efforts that may be seen between different patients in the pediatric ICU as well as for the same patient during the course of illness. While patient agitation, a well-documented cause of NIV failure,8,9 is difficult to replicate in bench research, it may be best reflected as variations in patient effort as was done in our study. It also should be noted that the RAM cannula is not approved as an interface for NIV but rather for high-flow oxygen delivery, although it is being used in this capacity in pediatric ICUs.2,22 Despite its accepted use in the literature as a measure of patient-ventilator interaction, the use of the AI may have limitations. Attempting to redefine an objective measure of asynchrony was not the aim of this study, but it is an area of future research that needs exploration.
Conclusions
The results of this study suggest that the presence of asynchrony is significant when using a nasal cannula interface for NIV in the younger pediatric population. There may be some improvement in asynchrony at higher levels of patient effort, although the high effort used in this study would likely require significant work by the patient and may not be sustainable clinically. Given the growing body of clinical data suggesting morbidity associated with asynchrony, the result of our study may have important clinical implications but require further validation with clinical studies. While this may be difficult, it might best be accomplished by comparing esophageal pressure or diaphragm electrical activity waveforms to ventilator waveforms during NIV. The results of this study raise the question of whether NIV with a nasal cannula interface is the most appropriate setup, or if other methods of trigger (eg, neurally-adjusted ventilatory assist) should be examined and employed more frequently when using this type of interface.
Footnotes
- Correspondance: Scott R Studeny MD, Cleveland Clinic Foundation, 9500 Euclid Ave, M-14, Cleveland, Ohio 44195–5243. E-mail: studens{at}ccf.org
Dr Studeny presented a version of this paper at the 2019 Critical Care Congress for the Society of Critical Care Medicine, held February 17–20, 2019, in San Diego, California.
Mr Chatburn has disclosed relationships with IngMar Medical, Vyaire Medical, Neural Research, and ProMedic Consulting. The remaining authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}