

Abstract
BACKGROUND: Measuring and monitoring end-tidal carbon dioxide (PETCO2) is an important aspect of caring for critically ill patients. The 2 methods used for PETCO2 measurement are the mainstream and sidestream methods.
OBJECTIVE: To assess the agreement between PETCO2 measurements performed by mainstream and sidestream methods with the PaCO2 values.
METHODS: This was a prospective observational study. A total of 114 subjects were enrolled in the study. PETCO2 measurements using mainstream and sidestream methods were performed simultaneously with the arterial blood sampling in subjects who were observed in the emergency department and required arterial blood gas analysis. Agreement between the PETCO2 measurements and the PaCO2 values obtained from arterial blood gas analysis were evaluated using the Bland-Altman method.
RESULTS: Sixty subjects (52.6%) were female, and the mean age was 60.9 years (95% CI 58.3–63.6). The mean PaCO2 was 35.16 mm Hg (95% CI 33.81–36.51), the mainstream PETCO2 was 22.11 (95% CI 21.05–23.18), and the sidestream PETCO2 was 25.48 (95% CI 24.22–26.75). Bland-Altman analysis showed an average difference between mainstream PETCO2 and PaCO2 values of 13 mm Hg (95% limits of agreement −0.6 to 25.5) and moderate correlation (r = 0.55, P < .001). The average difference between the sidestream PETCO2 and PaCO2 values was 9.7 mm Hg (95% limits of agreement −5.4 to 24.7) and poor correlation (r = 0.41, P < .001).
CONCLUSIONS: PETCO2 values obtained by mainstream and sidestream methods were found to be significantly lower than the PaCO2 values. There was essentially no agreement between the measurements obtained by 2 different methods and the PaCO2 values.
Introduction
Measuring and monitoring end-tidal carbon dioxide (PETCO2) is an important aspect of caring for critically ill patients. While PETCO2 monitoring was initially used by clinicians to confirm the place of the endotracheal tube and mechanically ventilated patients in the emergency department (ED), today there is a greater utilization of it for purposes such as monitoring the quality of cardiopulmonary resuscitation and evaluating the causes of bronchospasm.1–5 Furthermore, PETCO2 measurement has been studied to predict PaCO2 or bicarbonate levels.6,7
PETCO2 measures the amount of CO2 in the patient's exhaled air by a sensor. Depending on the location of the sensor, the measurement method is called sidestream or mainstream. The method is called sidestream if the air exchange is taking place via a circuit placed in the patient's air passage and the sensor is reading CO2 values from a sampling port connected to this circuit. If, on the other hand, the sensor is directly placed on the patient's air passage and the sensor directly performs CO2 readings, it is then called mainstream method.8,9 The sidestream method can be used in both intubated and non-intubated patients. However, the accuracy of this method is diminished due to increase in dead space resulting from suction catheters or blocking of the catheter by fluids and secretions. The mainstream method has advantages by directly performing the measurement through the air passage, and therefore is reported to yield more accurate results.10 While the mainstream methods were performed only on intubated patients, due to the size and weight of the sensors in the past, it is now practiced noninvasively on non-intubated patients through reduced size and weight of sensors.
Studies evaluating the agreement between the PaCO2 and sidestream PETCO2 values yielded no favorable results.6,11,12 On the other hand, there is insufficient information on the degree of agreement between PaCO2 values and mainstream PETCO2 measurements performed on non-intubated patients. The future benefit of establishing such a correlation will lie in the reduced need for obtaining blood samples through invasive and painful arterial procedures. The aim of this study was to assess the agreement between noninvasive PETCO2 measurements performed by the mainstream and sidestream methods with PaCO2 values.
QUICK LOOK
Current knowledge
Monitoring end-tidal carbon dioxide (PETCO2) is a standard of care in the operating room, and can provide useful information in the ICU. The relationship between PETCO2 and PaCO2 is affected by cardiac output, minute ventilation, and ventilation/perfusion matching. Both mainstream and sidestream sampling are used by capnometers.
What this paper contributes to our knowledge
The relationship between PaCO2 and PETCO2 was poor in patients with and without lung pathology. The type of gas sampling (sidestream versus mainstream) did not impact the PaCO2/PETCO2 relationship.
Methods
Study Design and Setting
We conducted a prospective observational trial in an academic ED that has an annual census of 30,000 patient visits. The study was between February and May 2011. The study was approved by the institutional review board, and informed consent was obtained from all subjects (project 2011/25, KAEK 2/10).
Selection of the Subjects
We enrolled ED adult patients who required arterial blood gas (ABG) analysis for their diagnostic evaluation. Patients with trauma, altered mental status, mechanical ventilation, and those who did not provide consent were excluded from the study.
Study Protocol, Measurements, and Data Collection
Once informed consent was obtained, subjects' demographic and clinical data were recorded on the standardized study forms. PETCO2 measurements were conducted by both methods, simultaneously with the ABG sampling. One researcher (MY), with the requisite experience with the relevant equipment, performed all of the measurements. Subjects were asked to breathe normally. The highest PETCO2 value on the capnometer was recorded. A Nihon Kohden TG-921T3 sensor kit (Nihon Kohden, Tokyo, Japan) was used for mainstream measurements. Original adapters obtained from the manufacturer were used for mainstream measurements (Fig. 1). The PETCO2 module on the Mindray BeneView T5 monitor (Shenzen Mindray Bio-Medical Electronics, Nanshan, Shenzhen, China) was used for sidestream readings. Sidestream measurements were conducted by a sampling port adapted to a simple oxygen mask (Fig. 2). ABG samples were analyzed using a Roche Cobas 121 device (F Hoffmann-La Roche, Basel, Switzerland) in a central laboratory.
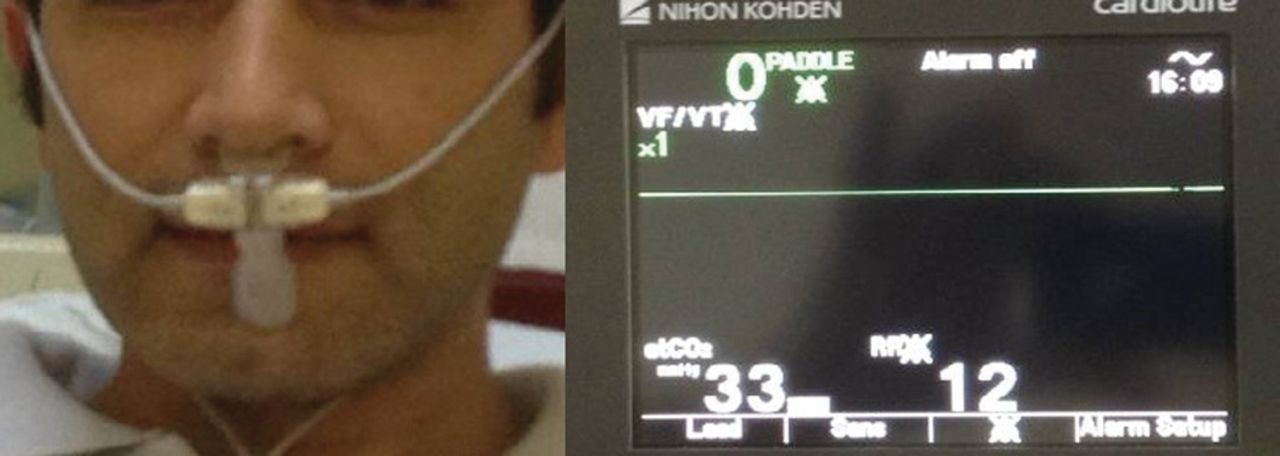
Noninvasive mainstream measurement with capnometer.
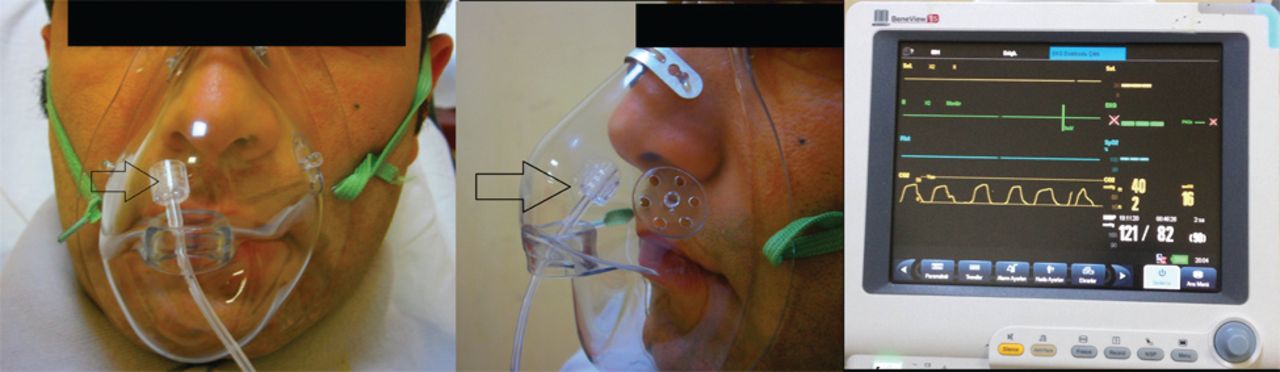
Noninvasive sidestream measurement with capnograph. The arrow points to tip of the sidestream line in the space of the face mask.
Primary Outcome Measure
The primary outcome measure was agreement between the PaCO2 measurements and the noninvasive PETCO2 measurements performed by the mainstream and sidestream methods.
Statistical Analyses
Software (MedCalc 12.1.4, MedCalcTurkey, Ankara, Turkey) was used for statistical analyses. Normal distribution was tested by the D'Agostino Pearson test. Continuous variables are represented by mean and 95% CI or median and 95% CI, whereas the categorical variables were represented with percentages. The independent t test was used for comparing mean values of subgroups. Pearson correlation analysis was conducted for testing linear relationship for each PETCO2 value obtained through noninvasive methods and PaCO2 value obtained by ABG analysis. Bland-Altman analysis was used to analyze agreement between the measurements.
The clinically acceptable limit of agreement was determined to be ± 5 mm Hg for this study. Software (G*Power 3.1.3, Franz Faul, Universitat Kiel, Kiel, Germany) was used to determine the sample size. During linear correlation analysis, the sample size was determined to be 111 for effect size = 0.3, alpha = 0.05 and power = 0.95. Furthermore, the sample size was determined to be 54 for mean differences of paired measurements (effect size = 0.3, alpha = 0.05 and power = 0.95). A P value < .05 was considered as statistically significant.
Results
The study was conducted with 119 subjects. Five subjects with outlying PaCO2 values were excluded from the study, and statistical analyses were performed on 114 subjects. Of those, 60 (52.6%) were female, and the mean age was 60.9 years (95% CI 58.3–63.6 y). Nineteen (16.7%) subjects were diagnosed with pneumonia in the ED, and 18 (15.8%) had cancer. Thirty-eight (33.3%) subjects were admitted to the wards. Demographic and clinical characteristics of subjects are presented in Table 1.
Main Characteristics of Subjects
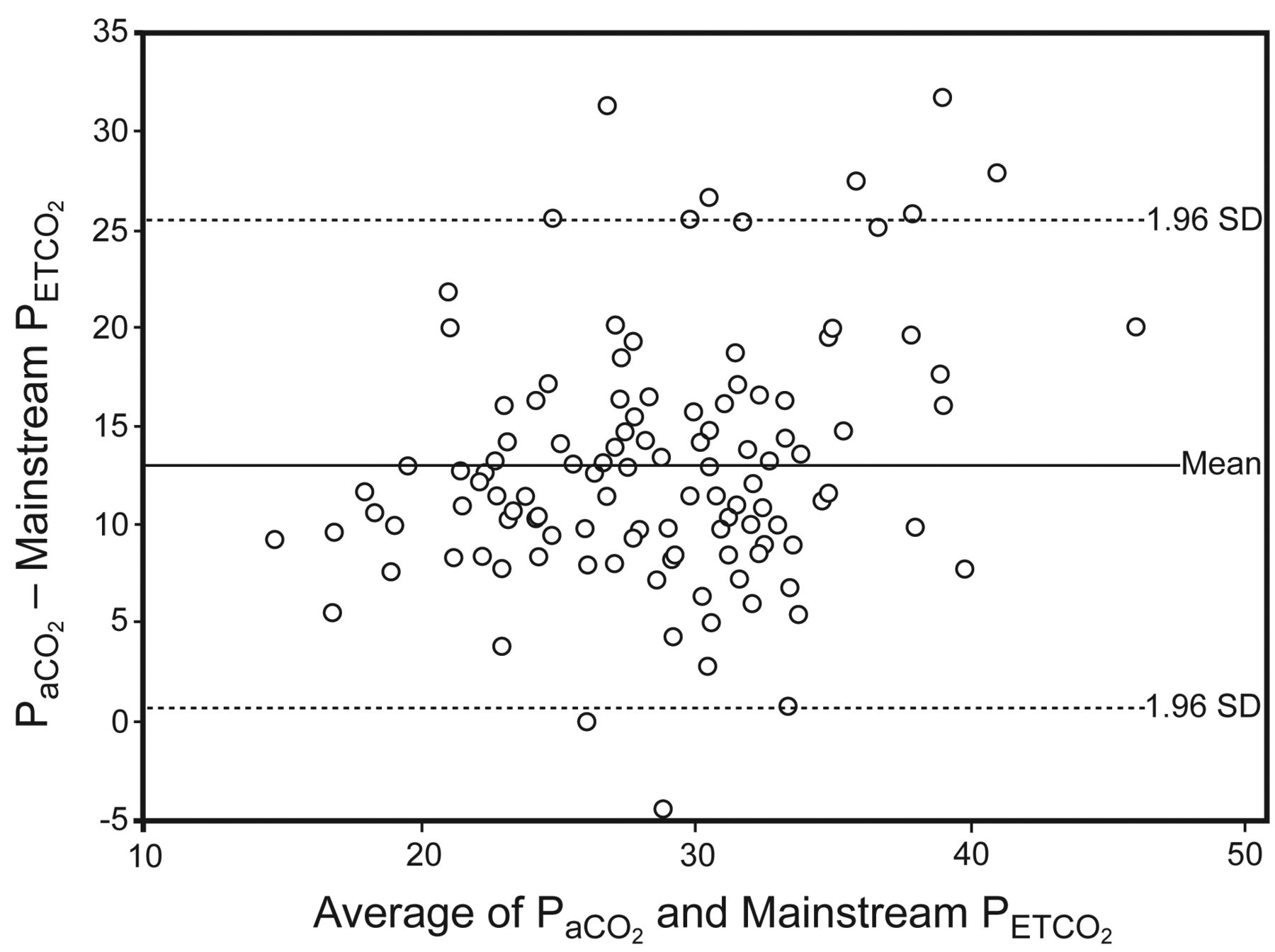
The mean PaCO2 was 35.16 mm Hg (95% CI 33.81–36.51 mm Hg), mainstream PETCO2 was 22.11 mm Hg (95% CI 21.05–23.18 mm Hg), and sidestream PETCO2 was 25.48 mm Hg (95% CI 24.22–26.75 mm Hg). Bland-Altman analysis showed an average difference between mainstream PETCO2 and PaCO2 values of 13 mm Hg (95% limits of agreement −0.6 to 25.5 mm Hg) with moderate correlation (r = 0.55, P < .001) between measurements (Fig. 3). Similarly, the average difference between sidestream PETCO2 and PaCO2 values was found to be 9.7 (95% limits of agreement −5.4 to 24.7); poor correlation (r = 0.41, P < .001) was noted (Fig. 4). Five (5.3%) PETCO2 measurements with the mainstream method and 31 (27.2%) with the sidestream method were found to be within the previously determined ± 5 mm Hg limits of agreement.

Bland-Altman plot of mainstream end-tidal carbon dioxide (PETCO2) compared with arterial carbon dioxide (PaCO2).

Bland-Altman plot of sidestream end-tidal carbon dioxide (PETCO2) compared with arterial carbon dioxide (PaCO2).
Study subjects were compared based on the presence of lung pathology. Mean values for PaCO2, mainstream PETCO2, and sidestream PETCO2 were similar (Table 2).
Mean PETCO2 and PaCO2 in Subjects With and Without Lung Pathologies
Discussion
This study revealed no agreement between noninvasive PETCO2 measurements with the mainstream and sidestream methods and PaCO2 values. While the acceptable difference caused by the alveolar dead space had been set at 5 mm Hg prior to the study, the actual difference was found to be 1 mm Hg following the data analysis.13 The mean bias in sidestream PETCO2 and PaCO2 values was reported to be between 3.5 mm Hg11 and 8.4 mm Hg.6 The difference increased to 6 mm Hg in subjects with respiratory or metabolic acidosis; however, the strong correlation continued.11 In a study conducted in 162 subjects who presented to the ED for complaints related to difficult breathing, a strong positive correlation was reported between the mainstream PETCO2 and the PaCO2 values. The mean bias was 0.5 mm Hg and the limits of agreement were −10.5 mm Hg and 9.5 mm Hg. In this particular study, a mainstream capnometry device designed for invasive measurement was used noninvasively with an adapter.10 Although we used the original mainstream sensor by the manufacturer, the bias was 13 mm Hg in the current study. Sidestream measurement, even though conducted similar to other studies in the literature, yielded a bias of 9.7 mm Hg. Unlike others, we enrolled subjects without shortness of breath. The subgroup analysis showed no difference between the mean PETCO2 values of the subjects with and without lung pathology.
The first study in which the sidestream and the mainstream methods were compared was carried out with invasive techniques on mechanically ventilated dogs. In that study, the bias between mainstream PETCO2 and PaCO2 was 3.15 mm Hg, while it was 5.65 mm Hg with the sidestream method. Regardless of the measurement method, the bias was reported to increase when PaCO2 values exceeded 60 mm Hg.14 In the first study comparing 2 noninvasive methods, the sidestream and microstream techniques, Casati et al measured the mean difference between PETCO2 and PaCO2 as 4.4 mm Hg by the microstream method, which was increased to 7 mm Hg with the sidestream method.15 Our study compared the sidestream and mainstream methods in the ED, and there was no agreement found between the PaCO2 and PETCO2 values obtained by both methods. For comparison of PETCO2 measurement techniques, the type and location of the sensor are important issues that can also affect the results. In a study that compared the distal sidestream, proximal sidestream, and mainstream methods, the reported differences were 6.6, 25.5, and 9.25 mm Hg, respectively.16 Despite the fact that we performed our study in a standardized condition, we measured significantly different PaCO2 and PETCO2 values obtained through both methods.
PaCO2 prediction with PETCO2 values has been diminished in patients with lung disease.17 Furthermore, structural defects of the lung (eg, hyaline membrane disease or meconium aspiration) in newborns have led to poor correlation between PETCO2 and PaCO2 values.18 In our study we found poor correlation and no agreement between the PaCO2 values and PETCO2 values obtained through 2 separate methods in patients with lung pathologies. Since the same lack of agreement and poor correlation were found in patients with no lung pathology, we believe that these differences arise from measurement methods. Technological improvements in the future may result in increase in agreement between PETCO2 and PaCO2 values.
Limitations
This study was conducted in a single center with one set of medical devices. All the devices used during the study had been calibrated by qualified technicians and all were functioning properly. However, errors resulting from functioning of devices can nonetheless affect the entire study results. Performing measurements by a single researcher minimizes the potential for variations that could be caused by an operator. Furthermore, the study group was heterogeneous, since it consisted of subjects requiring ABG analysis. However, the ABG analysis was performed in subjects suffering from a variety of conditions, such as poisoning, metabolic disorders, and respiratory problems, in the ED. In line with our initial goal of using noninvasive PETCO2 measurements in place of invasive PaCO2 readings, subjects from different subgroups were included in the study to determine agreement between measurements. Since the ability for deep breathing has an effect on PETCO2 readings, measurements conducted on subjects with various clinical conditions may not yield proper results. To overcome this disadvantage we considered the highest PETCO2 value obtained during our measurements. Besides, subgroup analyses showed no difference in PETCO2 readings between the subjects with and without lung pathologies. For this reason we believe there was no limitation inherent in our selection of the study group.
Conclusions
Noninvasive PETCO2 measurements performed both by mainstream and sidestream methods were found to yield significantly lower and unacceptable results, compared to the PaCO2 values. Thus, neither of these methods is recommended as a reliable predictor of PaCO2 values.
Footnotes
- Correspondence: Murat Pekdemir MD, Department of Emergency Medicine, Kocaeli University, Kocaeli, Turkey. E-mail: mpekdemir{at}yahoo.com.
Dr Pekdemir presented a version of this paper at the 7th Türkiye Acil Tıp Kongresi, held October 13–16, 2011, in Trabzon, Turkey.
The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}