

Abstract
BACKGROUND: Protective ventilation implementation requires the calculation of predicted body weight (PBW), determined by a formula based on gender and height. Consequently, height inaccuracy may be a limiting factor to correctly set tidal volumes. The objective of this study was to evaluate the accuracy of different methods in measuring heights in mechanically ventilated patients.
METHODS: Before cardiac surgery, actual height was measured with a height gauge while subjects were standing upright (reference method); the height was also estimated by alternative methods based on lower leg and forearm measurements. After cardiac surgery, upon ICU admission, a subject's height was visually estimated by a clinician and then measured with a tape measure while the subject was supine and undergoing mechanical ventilation.
RESULTS: One hundred subjects (75 men, 25 women) were prospectively included. Mean PBW was 61.0 ± 9.7 kg, and mean actual weight was 30.3% higher. In comparison with the reference method, estimating the height visually and using the tape measure were less accurate than both lower leg and forearm measurements. Errors above 10% in calculating the PBW were present in 25 and 40 subjects when the tape measure or visual estimation of height was used in the formula, respectively. With lower leg and forearm measurements, 15 subjects had errors above 10% (P < .001).
CONCLUSIONS: Our results demonstrate that significant variability exists between the different methods used to measure height in bedridden patients on mechanical ventilation. Alternative methods based on lower leg and forearm measurements are potentially interesting solutions to facilitate the accurate application of protective ventilation.
- protective mechanical ventilation
- tidal volume
- predicted body weight
- height
- ventilator-induced lung injury
- acute lung injury
- measure
Introduction
In patients with ARDS, ventilation with high tidal volumes (VT) increases mortality, and protective ventilation with lower VT is now widely recommended.1–4 Several studies suggest that prophylactic protective ventilation should be used in most mechanically ventilated critically ill patients to avoid acquired ARDS5–7 and to improve outcome.6,8
It is well established that a patient's lung volume is well correlated to height,9 and this important physiologic value cannot be overlooked in mechanically ventilated patients. Indeed, protective ventilation implementation requires the calculation of predicted body weight (PBW) based on gender and height.1 Consequently, height inaccuracy may be a limiting factor to adequately reduce the VT. In this regard, it should be emphasized that PBW rather than actual body weight must be used to calculate the prescribed VT.8,10 The use of actual body weight can lead to large errors in VT settings,11 especially in women and obese patients.8,12 Visual estimation of the patient's height is frequently used in mechanically ventilated patients.13,14 However, visual estimation of height and, even more so, of PBW can be inaccurate.15–18 In addition, despite strong evidence and recommendations, protective mechanical ventilation is not optimally implemented19–23; unavailability of the height may be an additional barrier.11
Considering the central role of the physiologic value of the patient's height and its impact on mechanical ventilation settings, we conducted this study to evaluate the accuracy of usual measurements of height in mechanically ventilated patients and to assess alternative measurements.
QUICK LOOK
Current knowledge
Implementation of a lung-protective ventilation strategy requires the calculation of predicted body weight, determined from a formula based on gender and height. Any error in the measurement of height can lead to inappropriately set tidal volumes and failure to provide lung protection.
What this paper contributes to our knowledge
A significant variability exists between the different methods of measuring height in bedridden mechanically ventilated patients. Alternative methods of determining height based on lower leg and forearm measurements are potential solutions to facilitate the accurate application of protective ventilation.
Methods
From July 2010 to December 2011, we conducted a prospective study to evaluate height measurement accuracy in patients requiring cardiac surgery at the Institut Universitaire de Cardiologie et de Pneumologie de Québec. Study approval was obtained from the local ethics committee, and informed consent was obtained from all subjects before surgery.
Subjects
The research coordinator screened patients before the surgery. The exclusion criteria were the inability of the patient to stand up for initial measurement, including emergent surgeries, and patients already on mechanical ventilation before surgery.
Study Measurements
Preoperatively.
The reference method used for comparisons was the subject's actual height, measured with a height gauge while the subject was standing up. We also measured the lower leg length to calculate the height using the Chumlea method.24–26 We measured the lower leg length with a special caliper while the subject was sitting with knees bent at a 90° angle. The length from the top of the knee (patella) to the bottom of the heel was measured. The subject's height was calculated using previously described equations.26 In addition, we measured the subject's forearm with a tape measure between the olecranon process of the elbow and the midpoint of the prominent styloid process of the radius. We then calculated the height based on a previously described chart.27 Each measurement was performed only once for each subject, and two different investigators were involved in these measurements (Fig. 1).

Different methods to measure height. Five methods to obtain patient heights were compared. Preoperatively, subjects were measured with a height gauge while standing upright (1); this measure was used as the reference method. Lower legs (2) and forearms (3) were also measured, and subject height was derived from previously validated formulas.26,27 Formulas to predict height based on lower leg measurement are provided, based on Reference 26. Postoperatively, heights were visually estimated (4) by one clinician, and (5) subjects (bedridden in a supine position) were subsequently measured with a tape measure.
Postoperatively.
Within the first minutes after arriving at the ICU, other data were recorded while subjects were on mechanical ventilation. First, each subject's height was visually estimated by a nurse or a respiratory therapist and then subsequently measured by a nurse with a tape measure while the subject was supine in bed. Nurses and respiratory therapists were not aware of the subject's preoperative height (see Fig. 1). The PBW was calculated using the previously validated equations.1
Statistical Analysis
Data are presented as means ± SD. Categorical variables are presented as counts. Agreement between results was expressed by the Bland-Altman method,28 and all data are presented using Bland-Altman plots. Estimated bias (average of the differences between the reference height [gauge] and the different measuring methods) and 95% CI (bias ± 1.96 × SD) were calculated. For errors of measurement, we calculated the mean of absolute difference between the reference and the different measuring methods. A generalized linear mixed model was performed using the normality or the binary model according to the data distribution. A compound symmetric structure was used to consider the dependence among measurements. Posteriori comparisons were performed using the Tukey technique. Relationships between the reference and the other methods of measurement were analyzed using Pearson correlation coefficients. All reported P values were declared significant at .05. Data were analyzed using a statistical package (SAS 9.3, SAS Institute, Cary, North Carolina).
Results
Subjects
One hundred subjects (75 men, 25 women) with a mean age of 66.0 ± 9.3 y were studied. A total of 500 measurements of subjects' heights were obtained (5 measurements per subject). The mean actual weight was 79.5 ± 17.6 kg; the mean PBW was 61.0 ± 9.7 kg. The median (interquartile) height measured by height gauge before surgery was 167 cm (159–174 cm). Data on height obtained with the different measuring methods and errors in comparison with the reference measure are shown in Table 1.
Difference Between Reference Values and Other Methods for Height Measurement
Differences Between Actual Height, Tape Measure Method, and Visual Estimation
The results obtained using a tape measure and visual estimation were well correlated with the reference (height gauge) (Fig. 2). Compared with the reference, bias with the tape measure was −3.7 ± 5.0 cm (95% CI −13.5 to 6.2), and bias with visual estimation was −4.0 ± 7.0 cm (95% CI −17.7 to 9.7) (Fig. 3). Maximum errors with tape measure and visual estimation were 19.0 and 20.5 cm, respectively.

Scatter plots with Pearson correlations between the reference values for height measurement and visual estimation (A), tape measure method (B), lower leg measurement (C), and forearm measurement (D). Solid lines represents the regression line, and dashed lines represent 95% CI.
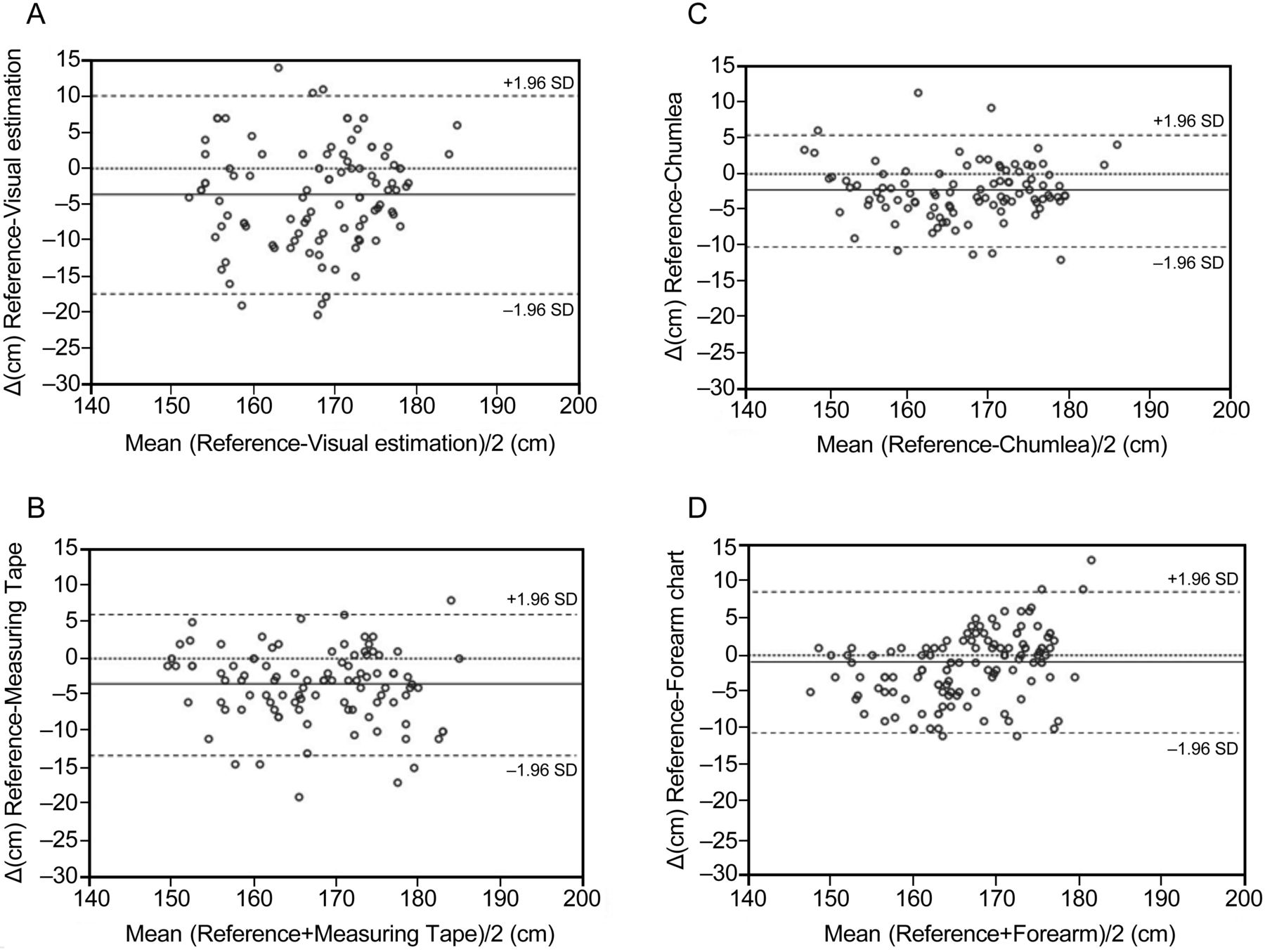
Bland-Altman graph comparison of the reference value for height measurement and visual estimation (A), tape measurement (B), lower leg measurement (C), and forearm measurement (D). The solid lines represent the bias, and the dashed lines represent 95% CI.
Error of visual estimation was inversely correlated to the subject's height (r = 0.52, P < .001). (See the supplementary materials at http://www.rcjournal.com.) Mean error of visual estimation was significantly greater with shorter subjects (those with a median height of ≤ 167 cm: 7.3 ± 6.7 vs 0.4 ± 5.5 cm, P < .001).
Alternative Methods: Height Derived From Lower Leg (Chumlea Method) and Forearm Length
Height derived from the lower leg and forearm correlated well with height gauge (Fig. 2). Compared with the reference, bias with the lower leg was −2.4 ± 3.9 cm (95% CI −10.0 to 5.2), and bias with the forearm was −1.3 ± 5.0 cm (95% CI −10.8 to 8.6) (Fig. 3). Maximum errors with the lower leg and forearm methods were 11.9 and 20.0 cm, respectively.
Potential Impact on Protective Mechanical Ventilation
The mean actual body weight was 30.3% higher than the PBW, and differences in the calculation of VT with actual body weight versus PBW were of similar amplitude. The errors for PBW were higher when the calculation of PBW was based on visually estimated heights and lower when the Chumlea method was used (Table 2). PBW errors of > 10% were present for 15% of the subjects when using the lower leg or forearm method, 25% when using a tape measure, and 40% when relying on visual estimation (Table 2). As expected, the error in VT settings was marked when actual weight, rather than PBW, was used (Table 3). We compared the impact of the errors for shorter and taller subjects based on the median height of the subjects (ie, 167 cm). The actual weight was higher than the PBW, from +21% (in subjects > 167 cm) to +35% (in subjects ≤ 167 cm) (Table 3). In comparison with the VT set with PBW, based on the reference height, maximal overestimation of VT settings in short subjects changed from 396 mL with an actual weight to 82 and 73 mL with the lower leg and forearm methods, respectively (See the supplementary materials at http://www.rcjournal.com.). Among shorter subjects (≤ 167 cm), the proportion of women was 45.1% (23/51), whereas among taller subjects (> 167 cm), the proportion of women was only 4.1% (2/49, P < .001) (Table 3). Of those measuring less than the median height, 92% were women.
Differences in PBW Based on Reference Height and Other Measurement Methods
Impact of Height Measurement Method on VT Setting
Discussion
Predicted rather than actual body weight should be used to determine the VT required for mechanically ventilated patients.1,8,10 However, the patient's height is required to calculate PBW.1 We compared different direct and alternative methods to measure height in 100 bedridden mechanically ventilated subjects. We showed that significant differences exist between these methods (tape measure, visual estimation, and lower leg and forearm length) and the reference standard (gauge measurement). We found that visual estimation of height was an inaccurate method with large potential errors. The alternative methods, which were based on lower leg and forearm length, were close to the reference method and were at least as efficient as the tape measure method. This study represents the largest evaluation of different methods to assess height in bedridden subjects and demonstrates the potential impact on protective ventilation implementation.
Despite the paucity of data, several studies suggest that height is not being used to set the VT11,14 or that height is unknown because as many as 40% of ARDS patients had no height listed in their medical records,29 and consequently, visual estimation of height or weight is frequently being used.13,14,30 In surgical units, patients are frequently measured preoperatively. In a recent study, heights measured before surgery were available for 3,763 patients and were missing for only 6 patients (0.16%).8 Although little data are available, it is likely that the tape measure method is also frequently used for medical bedridden patients when height is not known. In a survey of 20 ICUs in the United Kingdom, 15 measured patients with tape, and 5 estimated heights.13 Our results show that visual estimation and the tape measure method while subjects are supine are not accurate, with maximum errors being ∼20 cm. These errors were associated with large errors in VT settings. Our results are in agreement with previous data that showed inaccuracy of visual estimations in different populations.15–18,31,32 To our knowledge, there is no study evaluating accuracy of the tape measure method in bedridden patients in comparison with the reference method with a height gauge when patients are standing upright.
Several methods have been described to obtain a patient's height indirectly, among which lower leg measurement (knee-heel length, Chumlea method),24–26 forearm measurement (from elbow to wrist), and demispan (distance from the middle of the sternal notch to the tip of the middle finger in the coronal plane) are the most frequently evaluated.27,33 These alternative methods are potentially useful for bedridden patients or mobility-impaired patients.24 For these patients, the tape measure method may be difficult to use (the subject's position in bed or the use of a short tape measure is a potential source of error) and may not be accurate, as we describe in this study. The use of a flexible tape measure to measure the lower leg is a potentially interesting solution.34
The Chumlea method, which allows height estimation based on knee-heel length, has been validated in large cohorts.24–26,35 In elderly patients, who represent the majority of mechanically ventilated subjects, this method was accurate in determining height.25,26 Our study evaluated 2 indirect methods (based on lower leg and forearm measurements), and we showed that these methods were well correlated with the reference method and were at least as accurate in bedridden subjects as using tape measure. Maximum errors were equivalent (with forearm measurement) or lower (with lower leg measurement) in comparison with a tape measure.
Potential Impact on Implementation of Protective Ventilation
In this study, VT was much higher when actual body weight rather than PBW was considered, which is in line with previous reports.11 It is now recommended to set VT based on PBW rather than actual body weight.1,8,10 However, errors in the measurement or estimate of a patient's height are responsible for errors when calculating PBW and, consequently, VT settings. It is likely that visual estimation is frequently used in mechanically ventilated patients. In the present study, the error in height estimation was greater in short subjects. Importantly, in this subgroup of shorter subjects, almost all were women. Consequently, the impact on VT setting was greater in this subgroup. Patients of shorter height were less likely to receive protective ventilation in previous studies.36,37
The tape measure method was also associated with potentially high errors in VT settings. Overestimation of VT reached almost 150 mL when the tape measure method was used to calculate PBW rather than the reference height. With alternative methods (lower leg and forearm measurements), maximum errors in VT were limited to between 73 and 87 mL. In addition, because of the formula for the PBW calculation, an error in height measurement or estimation leads to higher errors in VT settings in women compared with men. (See the supplementary materials at http://www.rcjournal.com.) Our data help explain, in part, why women frequently receive higher VT compared with men.7,8,11,12,30,36
These data highlight the importance of height in effectively reducing VT, which may be difficult when accurate height measurements are not available. Consequently, finding an accurate and easy method to obtain height measurements in bedridden patients is of great importance.
Limitations
Our study has several limitations. The Chumlea method (based on lower leg measurement) was not recorded directly in bedridden subjects, but preoperatively in seated subjects with knees bent at a 90° angle, which limits the chance of errors. The results may therefore not be directly transposable to the situation of mechanically ventilated supine subjects. The present study is to be considered as a first step in assessing this method as a potential alternative method of measurement. In a subsequent study, we evaluated a modified Chumlea method using lower leg measurement in bedridden subjects. Preliminary evaluation of this new method showed promising results, with very close correlation with the reference method.38 In the present study, we did not test the reproducibility of the measurements with different investigators, and this will need to be performed in subsequent studies.
One must remember that the Chumlea stature prediction equations have been made specifically for defined populations25 and that specific equations have been developed and should be used for differing populations.39,40
VT may not be the optimum value to consider in mechanically ventilated patients. Indeed, some authors advocate the use of other physiologic surrogates, such as transpulmonary pressure or lung volumes, instead of VT per PBW, given the variable effect of a unique value of VT in a large population of subjects.41
Clinical Relevance
Protective mechanical ventilation is insufficiently implemented19–23 due to several identified barriers; it is likely that difficulty in accurately measuring a subject's height and the lack of availability of derived formulas to calculate PBW are additional barriers. We described in this study several potential indirect methods that are at least as accurate as the tape measure method in bedridden subjects and that are more achievable. The data presented here also point out the inaccuracy of the visual estimation method, which can lead to large errors in VT settings. Visual estimation of height should definitively be avoided, as well as the use of actual body weight to determine VT.10
The optimum VT to prevent5,42 or treat4 ARDS in mechanically ventilated patients is still not clearly defined. It is well accepted, however, that high VT increases mortality in ARDS patients 1,4 and is associated with poor outcome in patients without ARDS.5,6 To this end, implementation of low VT strategies requires patients' heights to calculate PBW and to choose VT based on PBW rather than on actual body weight. The formulas used in the present study have been implemented in a free smartphone application (iAnthropometer ICU) that may facilitate implementation of protective ventilation.43
Use of reliable methods to measure height is also desirable to homogenize practices in the clinical field and for research purposes. In a meta-analysis, Eichacker et al4 showed that among the 5 randomized controlled trials evaluating different VT values in ARDS subjects, 4 different methods were used to determine weight: actual weight, dry weight, ideal body weight, and PBW. These various surrogates of weight were acceptable when the rates of obesity (body mass index > 30 kg/m2) were ∼10%, but today, these rates now approach nearly 40% in many countries,44 and consequently, actual body weight cannot be used to set the ventilator because of the risk of delivering high VT.8 In daily practice, the alternative methods that we describe may be more accurate than visual estimation and easier to apply in comparison with the tape measure method.
Conclusions
We showed that the method used to obtain a patient's height during mechanical ventilation might not be accurate and may have an impact on VT settings. A VT set according to actual body weight leads to large errors and should not be used; PBW requiring the patient's height should be used instead. The use of height measured with a tape measure, as well as visual estimation of height, can also lead to large errors in VT settings. When reference height is not available in patients undergoing mechanical ventilation, alternative methods to obtain patients' heights based on lower leg and forearm measurements could be useful to facilitate the application of protective mechanical ventilation to prevent5 or treat1,2 ARDS. Knowledge and accurate application of a subject's height are low-cost therapeutic interventions based on basic physiology, as lung size is closely related to height.9 This simple yet under-recognized fact should not be overlooked, especially if one considers that the only proven treatment of ARDS relies on the application of appropriate ventilatory settings.1,2
Acknowledgment
We thank Dr Jed Lipes for manuscript revisions and English editing.
Footnotes
- Correspondence: François Lellouche MD PhD, Unité de Soins Intensifs de Chirurgie Cardiaque, Groupe de Recherche en Santé Respiratoire, Centre de Recherche, l'Institut Universitaire de Cardiologie et de Pneumologie de Québec, 2725 Chemin Sainte-Foy, Ville de Québec, Québec G1V 4G5, Canada. E-mail: francois.lellouche{at}criucpq.ulaval.ca.
Supplementary material related to this paper is available at http://www.rcjournal.com.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 1155
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}