

Abstract
BACKGROUND: The 2009 pandemic influenza A (H1N1) virus was accompanied by high morbidity and mortality. The aim of this study was to describe the clinical characteristics of patients with documented 2009 influenza A (H1N1) virus admitted to a reference chest hospital, the disease outcome, and risk factors associated with ICU admission.
METHODS: We assessed 109 subjects admitted to the respiratory infection unit of a hospital for chest disease with signs and symptoms of the 2009 influenza A (H1N1) virus between April 2009 and December 2010. Demographic data, comorbidities, clinical signs and symptoms, laboratory tests, radiographic findings, treatment, and final outcomes were all recorded. Factors associated with severe disease requiring ICU admission were determined.
RESULTS: Ninety subjects (82.5%) had laboratory-confirmed 2009 influenza A (H1N1). Sixty-four percent of these subjects had pneumonia on admission, 26% had respiratory failure, and 11% required care in the ICU. Dyspnea and the presence of infiltrates on chest x-rays were the most common signs among the subjects with H1N1. All subjects were treated with antiviral therapy, and 75% received antibiotic treatment based on their clinical and laboratory findings. The predictive factors of ICU admission were severe hypoxemia and lymphocytosis.
CONCLUSIONS: The outcome of subjects with influenza A (H1N1) virus infection was influenced by the severity of the disease on admission, the subjects' underlying conditions, and complications during hospitalization.
Introduction
Following the first laboratory-confirmed 2009 influenza A (H1N1) case on May 18, 2009, Greece showed a moderate wave of transmission, followed by a stronger wave in October and a peak in incidence in November.1 The first 2009 influenza A (H1N1) cases were associated with imported transmission (eg, Greek students returning home from abroad and foreign tourists).2 During the pandemic period, there were 18,230 reported laboratory-confirmed 2009 influenza A (H1N1) cases and 88,244 visits to emergency departments and 10,040 hospitalizations due to an influenza-like illness. Among these cases, 294 were admitted to ICUs, and 149 died from causes related to 2009 influenza A (H1N1).2–7 Since that period, influenza epidemics have resulted in an estimated 3–5 million cases of severe illness and 250,000–500,000 deaths each year.1,8,9 The risk of complications from influenza, including lower respiratory tract infection, hospital admissions, and death, depends on varying determinants such as age and type of comorbidity that may be present.8,9 In this context, it is of importance to characterize the risk factors predisposing for adverse outcomes. The purpose of this study was to describe the clinical characteristics of subjects with documented 2009 influenza A (H1N1) admitted to a reference chest hospital, the disease outcome, and risk factors associated with ICU admission.
QUICK LOOK
Current knowledge
The H1N1 flu epidemic of 2009 was associated with severe hypoxemic respiratory failure in patients at risk, including those with pre-existing neuromuscular and respiratory disease, as well as obese and pregnant patients. Adjuncts to mechanical ventilation included extracorporeal membrane oxygenation, inhaled nitric oxide, and prone positioning.
What this paper contributes to our knowledge
Patients with H1N1 infection presented with greater dyspnea, tachycardia, cough, and sputum production compared with patients with flu-like symptoms but negative H1N1 swabs. Subjects with H1N1 also had more frequent infiltrates on chest radiograph, and hospital stay was twice as long. Secondary bacterial infections occurred in 76% of H1N1 subjects.
Methods
This was a retrospective analysis of patients admitted to the respiratory infection unit (RIU) of the First Department of Respiratory Medicine at the Medical School of the University Athens and the “Sotiria” Chest Diseases Hospital from April 2009 to December 2010. Patients either presented to the emergency department of the hospital on their own or were referred by primary care physicians, non-reference hospitals, or other health-care facilities. The Hellenic Centre for Disease Control and Prevention prepared and provided guidelines for case and contact management and for infection control, which were sent to all reference hospitals and published on the web site (http://www.keelpno.gr; Accessed December 29,2012).
The study sample consisted of subjects who presented to the emergency department with an influenza-like illness and were investigated for the 2009 influenza A (H1N1) virus and who were then admitted to the RIU due to underlying chronic conditions or to treat emerging complications. Influenza-like illness was defined as illness of a sudden onset with (1) fever, headache, malaise, or myalgias and (2) shortness of breath, cough, or sore throat.10 A confirmed case was defined as a positive test result for the 2009 H1N1 virus using real-time polymerase chain reaction.11 Nasopharyngeal swabs were collected and sent for analysis to a designated reference laboratory (Hellenic Pasteur Institute, Athens, Greece). All subjects admitted to the RIU were tested for the 2009 pandemic influenza A (H1N1) virus, and the results were available in < 24 h. The study was approved by the ethics committee of the hospital.
Data Collection
Data were retrospectively collected using a standard form that included demographic characteristics, past medical history, comorbidities, prehospital medication, H1N1 vaccination, travel to endemic countries, clinical presentation, body mass index, biochemical markers, chest radiograph findings, medical treatment, and outcomes (including discharge, ICU admission, and death).
Pneumonia was defined as the presence of a new infiltrate on a chest x-ray and fever (temperature of ≥ 38.0°C) and/or respiratory symptoms. A concomitant and/or secondary bacterial co-infection was diagnosed in subjects having at least one positive blood or sputum culture and/or a positive urinary antigen. Complications were defined as any adverse incident occurring during hospitalization. Obesity was defined as a body mass index of ≥ 30. Comorbidities were assessed by the Charlson comorbidity index.12
Statistical Analysis
Data are described as mean ± SD and median (range). The Wilcoxon rank-sum test was used for comparison of continuous variables in 2 groups. Relationships of categorical variables were examined by the chi-square test or the Fisher exact test, when appropriate. Furthermore, a multiple stepwise logistic regression analysis was performed to examine potential independent factors related to ICU admission. The statistical significance was set at < .05. Statistical analysis was conducted with SPSS 17.0 (SPSS, Chicago, Illinois).
Results
During the study period, 109 subjects (all adults) were admitted to the RIU. Of these, 90 (82.5%) proved to have positive nasopharyngeal swab results for the 2009 H1N1 virus, and 19 (17.5%) had negative swab results. The subjects with positive swab results had a mean ± SD age of 37 ± 15 y compared with those with negative swab results, who had a mean age of 40 ± 18 y (P > .05). The demographic data, symptoms, clinical manifestations, and outcomes are shown in Table 1. Twelve subjects required invasive mechanical support due to respiratory failure and were transferred to the ICU (mean ± SD age of 52 ± 12 y). The clinical and laboratory data for the subjects admitted to the ICU are shown in Figure 1. Forty-five of 109 subjects (41%) had at least one comorbidity, with the most common conditions being asthma (19 cases, 17%) and COPD (10 cases, 9%). Subjects with positive swab results had significantly more comorbidities as expressed by the Charlson comorbidity index compared with those with negative swab results (1.9 ± 1.2 vs 1.5 ± 0.7, P = .007).
Demographic Data, Symptoms, and Clinical Findings of Subjects Admitted to the Respiratory Infection Unit
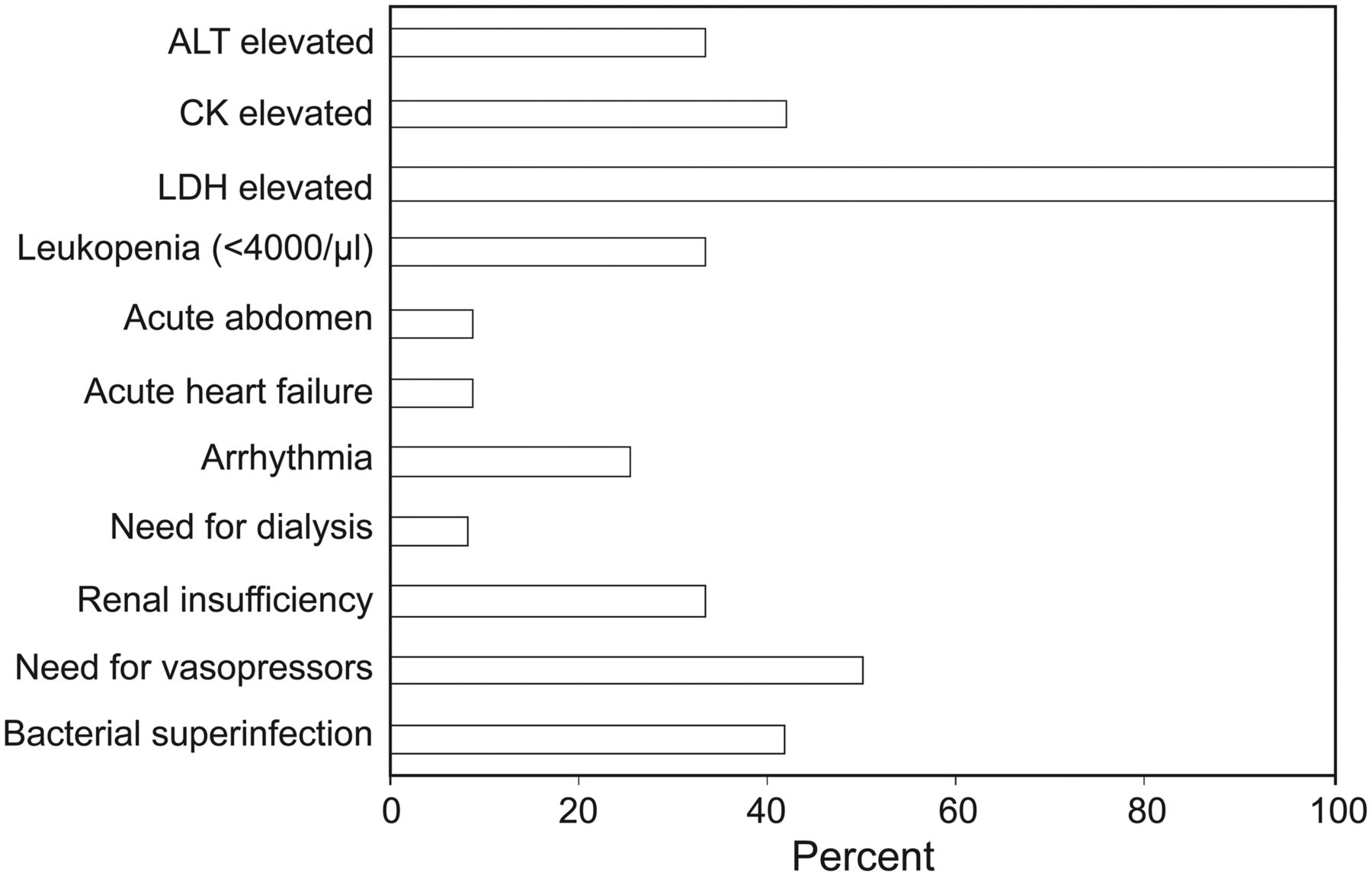
Clinical and laboratory data of subjects upon admission to the ICU. ALT = alanine aminotransferase; CK = creatine kinase; LDH = lactate dehydrogenase.
Upon hospital admission, the most common symptoms and signs were fever, tachycardia, and cough. Subjects with the 2009 H1N1 virus presented with significantly more dyspnea (42% vs 17%, P = .04), tachycardia (87% vs 66%, P = .034), expectoration (47% vs 5%, P = .001), and cough (91% vs 44%, P = .001) compared with subjects with an influenza-like illness (see Table 1). Furthermore, 64% of subjects with the 2009 H1N1 virus had infiltrates on x-rays at admission compared with 17% of subjects presenting with an influenza-like illness (P = .001).
The mean ± SD hospital stay was 7 ± 2 d for subjects with the 2009 H1N1 virus and 3 ± 2 d for subjects with an influenza-like illness (P = .001) (see Table 1). Twelve subjects were transferred to the ICU (all with a positive swab for the 2009 H1N1 virus). Overall, only one of the H1N1 subjects died in the ICU due to shock/multiple organ failure. This subject was immunosuppressed due to human immunodeficiency virus infection.
A concomitant and/or secondary bacterial co-infection was present in 76% of subjects with the 2009 H1N1 virus compared with 28% of subjects with an influenza-like illness (P = .001), whereas there was a statistically significant difference in the presence of a co-infection between the subjects admitted to the RIU and ICU (Table 2). Overall, Streptococcus pneumoniae (isolated from blood and sputum and by urinary antigen testing), Haemophilus influenza (isolated from sputum and blood), Moraxella catarrhalis (isolated from sputum), and Staphylococcus aureus (isolated from sputum and blood) were the most frequent causative bacteria. Other organisms isolated were Pseudomonas aeruginosa (isolated from sputum and blood), Candida albicans, and Acinetobacter baumannii.
Symptoms, Clinical and Laboratory Findings, and Comorbidities for Subjects With Positive Swabs Hospitalized in the RIU and Those Hospitalized in the ICU
Treatment
Overall, 99 subjects (91%) were treated with oseltamivir within 24 h of admittance at a dosage of 75 mg twice daily, but 18 subjects who had severe respiratory failure (12 of them were in the ICU) were treated from the beginning with 150 mg twice daily. Seventy-four subjects (68%) received antibiotics for a median of 7 d (range of 1–28 d).13 No subject admitted to the ICU received steroid treatment.
Factors Correlating With ICU Admission
The demographic data, symptoms, clinical and laboratory findings, and comorbidities for the subjects treated in the RIU and ICU are shown in Table 2. With regard to symptoms, subjects who were admitted to the ICU presented to the emergency department more often with productive cough, implying an underlying bacterial superinfection, and confusion (67% vs 39%, P = .04, and 17% vs 2%, P = .01, respectively).
With regard to clinical and laboratory findings, subjects who were admitted to the ICU presented to the emergency department more often with infiltrates on x-rays (92% vs 53%, P = .01), respiratory failure (67% vs 19%, P = .001), lower PaO2 (51 ± 15 vs 70 ± 13 mm Hg, P < .001), and a higher absolute number of lymphocytes (2,065 ± 1,350 vs 1,112 ± 613, P = .03) compared with subjects who were hospitalized in the RIU (Fig. 2, A and B; see Table 2). Finally, subjects in the ICU had significantly more respiratory (50% vs 29%, P < .05), cardiovascular (17% vs 3%, P < .05), and immunosuppressive (17% vs 7%, P < .05) conditions as comorbidities compared with subjects in the RIU (see Table 2).

Levels of PO2 in arterial blood gas measurement (median value, interquartile range) (A) and absolute number of lymphocytes in peripheral blood (median value, interquartile range) (B) on admission of subjects to the respiratory infection unit (RIU) and ICU.
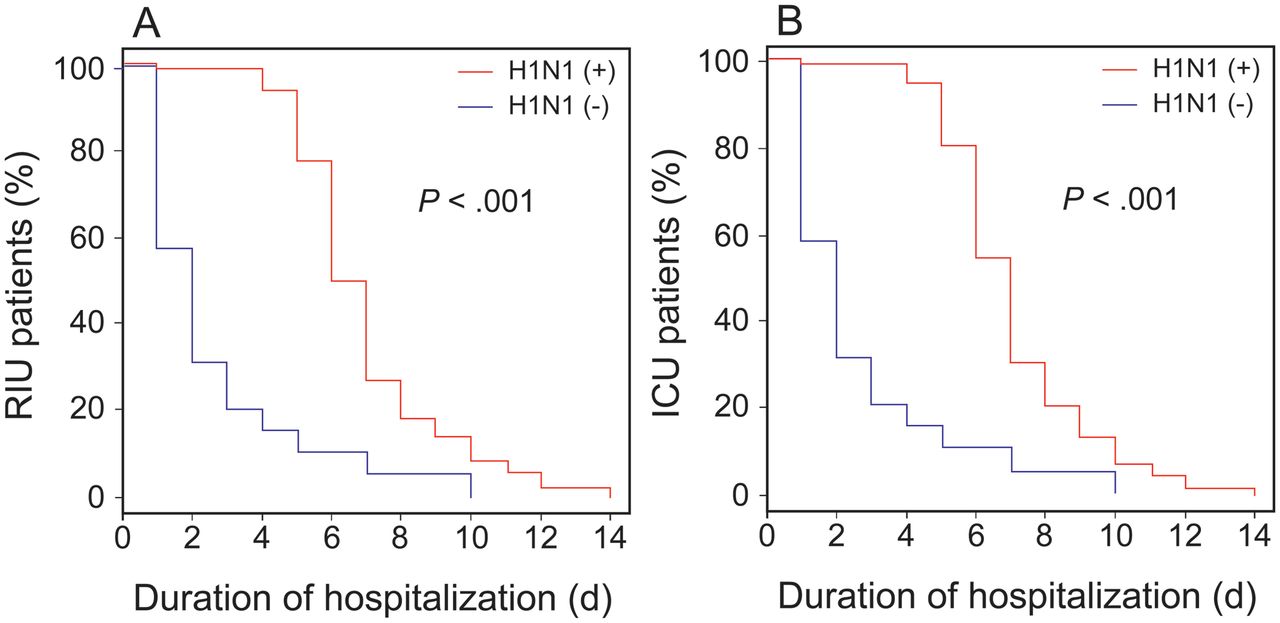
The presence of the 2009 influenza A (H1N1) virus significantly prolonged the hospital stay in both groups of subjects treated in the RIU or ICU (Fig. 3). Furthermore, among the subjects admitted to the ICU, those who had respiratory failure at presentation in the emergency department had a significantly higher hospital stay compared with those without respiratory failure at presentation (Fig. 4).

The presence of the 2009 influenza A (H1N1) virus significantly prolonged the hospital stay of subjects treated in the respiratory infection unit (RIU) or ICU. H1N1 (+) = H1N1-positive; H1N1 (−) = H1N1-negative.

Hospital stay of subjects who were positive for influenza A (H1N1) in the ICU in relation to the presence or absence of respiratory failure on admission to the hospital.
With the application of multiple logistic regression analysis, the prognostic factors for a subject's admission to the ICU were hypoxemia and lymphocytosis in peripheral blood (Table 3 and Fig. 5). Receiver operating characteristic analysis demonstrated that a PaO2 of 57.5 mm Hg had a higher sensitivity (90%) and specificity (83%). The cutoff point for the number of lymphocytes in peripheral blood with the best predictive power for ICU admission was 2,400 cells/μL (sensitivity of 59%, specificity of 97.6%).
Prognostic Factors for ICU Admission
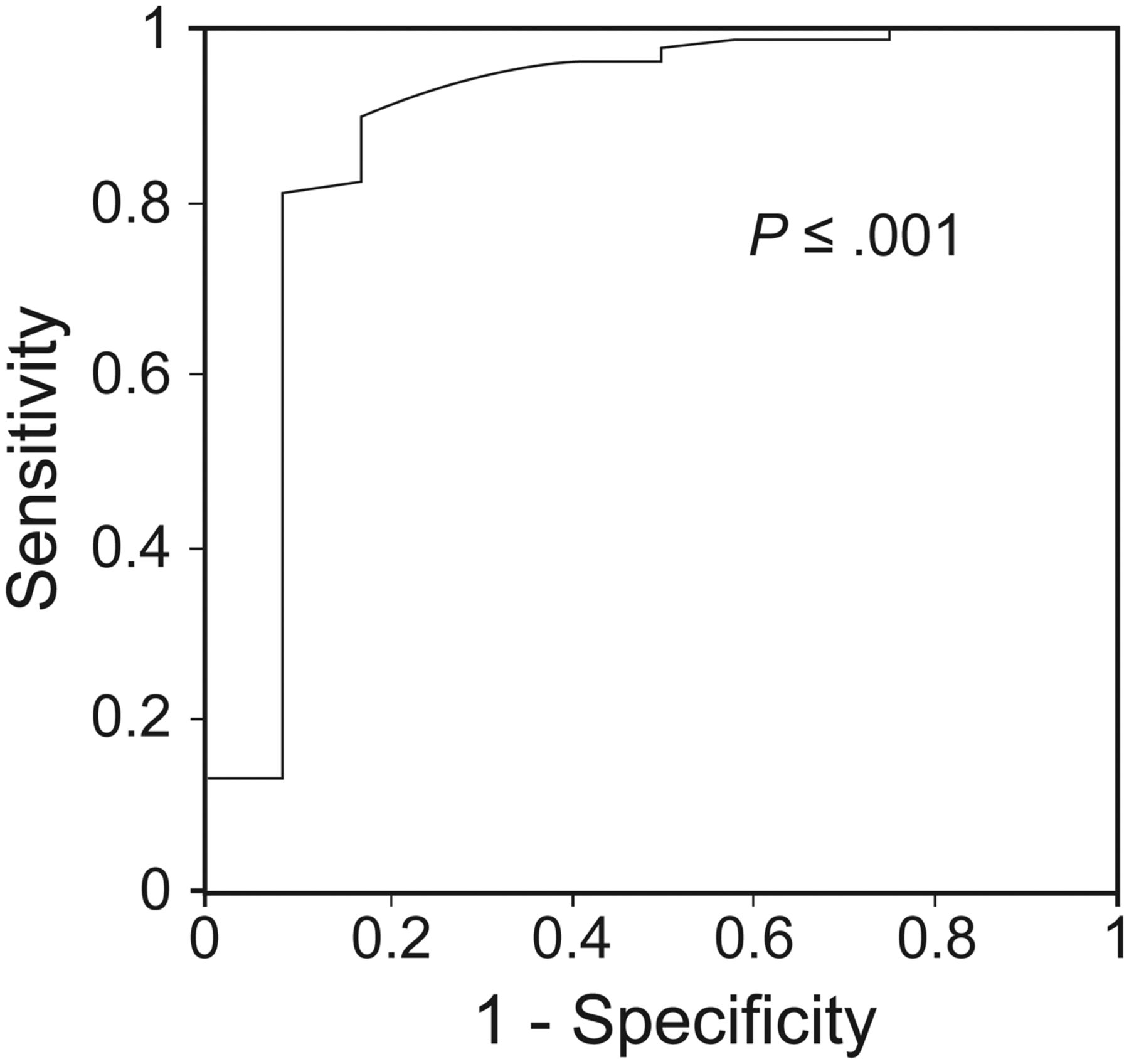
Hypoxemia as a strong prognostic factor for a subject's admission to the ICU.
Discussion
This study summarizes the demographic characteristics of subjects who presented to the emergency department of a reference hospital with an influenza-like illness requiring hospitalization and who were investigated for the 2009 influenza A (H1N1) virus during the pandemic. Furthermore, it defines the characteristics of the subjects in this sample who required mechanical ventilation and management in the ICU.
The mean age of hospitalized subjects with the 2009 influenza A (H1N1) virus in our sample was 37 y, with 52 y being the mean age of subjects admitted to the ICU. Our data are in accordance with previous studies showing that younger adults are more often hospitalized.14–16 This could probably be attributed to the fact that older people are partially protected by the presence of pre-existing antibodies from natural exposure to the A (H1N1) strains that circulated in the year following 1918 or to vaccine-induced cross-reactivity.17–19 Although several studies have shown that current and past pandemics affected mainly younger adults,20,21 with patients younger than 50 y having a higher risk of death,22 in a recent meta-analysis, a significant increase in the risk of hospitalization and death was found in elderly compared with non-elderly subjects, but this risk was associated with the existence of comorbidities.23 Multivariate analyses in several studies confirmed that the presence of concomitant diseases strictly related to age and probably not independent of it might represent a greater risk factor for ICU admission and death.14–16 Forty-two percent of the subjects in our sample who were hospitalized had at least one comorbidity, with the most common conditions being asthma (19 cases, 17%) and COPD (10 cases, 9%), whereas the remaining subjects had no comorbidities. This finding is in agreement with worldwide clinical data on 2009 H1N1 virus infection, which show that 25–50% of 2009 H1N1 patients who were hospitalized or died had no underlying comorbidities.24–27 Of the subjects admitted to the ICU, only one died. This was a subject who was positive for human immunodeficiency virus and who initially developed severe respiratory failure and finally multiple organ failure. Data show that immunosuppression increases the risk of death from pandemic influenza, and immunocompromised patients are more likely to be admitted to the hospital.23,28 In the remaining ICU subjects, the most common comorbidities were chronic respiratory diseases, namely, COPD and asthma. As shown in a recent meta-analysis,23 the presence of any chronic lung disease increased the risk of death and hospital or ICU admission, and COPD was specifically associated with ICU admission.23,29,30 Similarly, several international studies show a notable incidence of asthma in subjects hospitalized with H1N1 infection.31–36 Other recognized comorbidities complicating the course of our subjects in the ICU were cardiovascular disease and immunosuppression. Cardiovascular disease is a recognized comorbidity that increases the risk of hospitalization and ICU admission25,37 and is associated with increased risk of death.23,37 Although there was a rather low percentage of subjects with the 2009 influenza A (H1N1) virus and cardiovascular disease on the ward (3%), the relevant percentage of subjects admitted to the ICU was 17%. This could be explained by the fact that the subjects treated on the ward were significantly younger than those admitted to the ICU and had less possibility of having cardiovascular health problems. The lack of evidence associating obesity, a well-defined risk factor,23,32 with hospitalization and ICU admission in our study may be due to the small size of our study groups.
In our sample, 42% of the confirmed 2009 influenza A (H1N1) cases reported travel in an endemic country. This is not an odd finding because Greece is a popular tourist destination. The first 2009 H1N1 cases in Greece were associated with imported transmission (eg, students returning to Greece from abroad and foreign tourists).1,2 Subjects with an influenza-like illness presented with fever, tachycardia, and cough as the most frequent symptoms and signs on hospital admission. Subjects with the 2009 influenza A (H1N1) virus presented with significantly more dyspnea and productive cough compared with subjects with an influenza-like illness, with a documented concomitant and/or a secondary bacterial co-infection in 76% of the 2009 influenza A (H1N1) cases. Bacterial co-infections were similar to those reported in other case series.20,38,39 Although the ratio of subjects with a bacterial co-infection admitted to the RIU and ICU was relatively high, this did not affect the outcome of these subjects. This is in line with the report of Cillóniz et al,40 who showed that bacterial co-infection with H1N1 infection in subjects admitted with community-acquired pneumonia, although associated with higher severe scales on admission, did not influence the mortality. However, the significance of bacterial co-infections in the outcome of patients with influenza H1N1 should not be undermined or discarded. Several studies have shown increased morbidity and mortality in post-influenza bacterial pneumonia or co-infection.41,42 This has also been confirmed in numerous preclinical studies.43,44
Previous reports have shown that radiologically confirmed pneumonia is associated with severe outcomes.3,4,8,20,32 Although multivariate analysis did not reveal that pneumonia on admission was a significant clinical risk factor for a severe outcome in our study, it is noteworthy that 64% of subjects with 2009 H1N1 had infiltrates on x-rays at admission (92% for ICU subjects) compared with 17% of subjects presenting with an influenza-like illness, underlining its significance in complicating the confirmed cases requiring hospitalization.
The majority of our subjects received antiviral treatment (oseltamivir) within 24 h of admission. Timely administration of antiviral treatment has been correlated with better outcomes and with lower prevalence of respiratory failure in patients with 2009 influenza A (H1N1) virus infection.45–48 There is a consensus that treatment should be offered to 2009 H1N1-infected individuals with a high risk of complicated influenza or with signs of lower respiratory tract involvement, and therapy should start as soon as possible after symptom onset, regardless of the clinical severity at presentation.46 Although no solid conclusions can be drawn based on this observational study, the fact that 99% of the subjects were cured suggests the importance of the timely initiation of antiviral treatment for hospitalized patients with the 2009 pandemic H1N1 virus.
Only one of the subjects in our sample had been vaccinated against the 2009 H1N1 virus. Our findings are similar to those of other international studies that report an extremely low percentage of vaccinated patients.49,50 In Greece, vaccination against the 2009 H1N1 virus started at the end of November 2009, with the intention to be administered free of charge to anyone wishing to be vaccinated, aiming for global coverage. However, up to February 28, 2010, an extremely low percentage of the Greek population (3.2%) had been vaccinated,51 whereas the relative percentage in the United States and territories for the same time period was ∼23.9%.46 The main reason explaining the low vaccination percentage in Greek population was a belief that the vaccine might not be safe.51,52
Some limitations of the study should be noted. The sample size of the study was small, and this may have affected the statistical power to detect small effects. However, regardless of that, differences in the clinical presentation of subjects and outcomes were detected. In addition, factors that influenced ICU admission were observed.
In summary, in this study, the outcome of subjects with influenza A (H1N1) virus infection was influenced by the severity of the disease on admission, the subjects' underlying conditions, and complications during hospitalization.
Acknowledgments
We thank Konstantinos Vougas and Christina Sotiropoulou, Athens, Greece for their valuable contribution to the statistical analysis of the study data.
Footnotes
- Correspondence: Nikoletta Rovina MD PhD, Intensive Care Unit, First Department of Respiratory Medicine, Medical School, National and Kapodistrian University of Athens and “Sotiria” Chest Diseases Hospital, 152 Mesogeion Avenue, 11527 Athens, Greece. E-mail: nikrovina{at}med.uoa.gr.
The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}