

Abstract
BACKGROUND: Endotracheal tube (ETT) cuffs create a seal to protect against secretion entry to the lungs. Cuff inflation currently is recommended at 20–30 cm H2O pressure. ETT designs have variable seal performance in bench studies using rigid tracheal models lacking the dynamic characteristics of the human trachea. We compared ETT designs within a new, biorealistic tracheal model to assess cuff and suction performance in the setting of a compliant trachea.
METHODS: Three ETT designs (Mallinckrodt Hi-Lo, KimVent Microcuff, and Sheridan/HVT) were tested for performance by simulant leakage below the cuff and air leakage (measured as return tidal volume ≥ 80% delivered) over a range of cuff (5–25 cm H2O) and end-expiratory pressure (PEEP 0–15 cm H2O). Subglottic suction channel performance was tested in 2 ETTs (TaperGuard Evac [Covidien] and ISIS HVT [Teleflex]) as time to evacuate the simulant.
RESULTS: All ETT cuffs provided effective seals at an inflation pressure of 12 cm H2O when PEEP was ≤ 5 cm H2O. The Microcuff ETT sealed at the lowest pressure of 6 cm H2O, whereas the Sheridan/HVT cuff sealed at 12 cm H2O (P = .01). With a PEEP of 15 cm H2O, a reciprocal increase in air leak occurred, requiring a cuff inflation up to 22 cm H2O to maintain a return tidal volume at ≥ 80% delivered. Suction channel performance improved in the lateral position compared with supine for both ETT designs during continuous 15 mm Hg suction pressure (P = .001).
CONCLUSIONS: Within a novel model with normal trachea compliance, we found all ETT designs tested to seal at lower than current recommended cuff pressures.
Introduction
Ventilator-associated pneumonia has often been attributed to secretion leak around the endotracheal tube (ETT) cuff. Costs of ventilator-associated pneumonia are estimated to average 9 extra hospital days and greater than $40,000 additional expense per patient.1,2 Bundles of care that reduce the risk of ventilator-associated pneumonia include oral hygiene, semi-recumbent positioning, and suctioning techniques. Modifications of ETT cuff geometry, materials, and suction channels can further reduce risk of ventilator-associated pneumonia.3–5 Pliability and thickness of the cuff materials have been found to affect cuff seal performance, as has shape and length of the cuff.6–10
Recommended cuff inflation pressures are 20–30 cm H2O,11,12 which is about equal to tracheal perfusion pressure reported to be 22 mm Hg in a healthy trachea13 and may be lower with disease. Higher ETT cuff pressure may cause injury to the mucosa and lead to complications.13,14 Distribution of cuff pressure to the tracheal wall is heterogeneous, with regions of the tracheal wall receiving higher than the set internal cuff pressure.6
In vitro studies of ETT performance have typically used rigid trachea models.7–9,15 Although these allow for comparison between ETT designs, they do not represent the dynamic motion of the human trachea and its effect on ETT cuff performance. The airway motion is dynamic, leading to cross-sectional changes in response to airway pressures.16,17 A new biorealistic trachea model replicating the compliance of adult human tracheae has been developed.18 Our study's aim was to evaluate ETT performance within this trachea model, which mirrors intrinsic tracheal compliance. ETT cuff performance was assessed by measuring secretion leakage below the cuff and effective return tidal volume (VTe) over a range of cuff inflation pressures and airway pressures. Subglottic suction channel efficiency was also evaluated. The study was performed in the Department of Pediatrics, Virginia Commonwealth University School of Medicine (Richmond, Virginia).
QUICK LOOK
Current knowledge
The endotracheal tube cuff allows positive pressure ventilation and protects the airway from aspiration. Standard cuff pressures of 20–30 cm H2O are typically used to prevent leakage of fluid around the cuff and to prevent mucosal injury. In recent years, laboratory evaluations of cuffs in glass models have demonstrated reduced fluid leakage, but clinical studies have not confirmed these findings in vitro.
What this paper contributes to our knowledge
In a realistic viscoelastic model of the trachea, endotracheal tube cuffs of different designs provided an adequate seal at a pressure of 12 cm H2O. With increased PEEP, higher cuff pressures were required. Tubes with a subglottic suction channel performed best in the lateral position.
Methods
Biorealistic Tracheal Model
A 2-piece model with dimensions, surface topography, and rheology matched to that of a normal adult human trachea was used for testing. The model consisted of a mouth-throat component19 and trachea through the bifurcation of the main stem bronchi that approximates the cross-section profiles reported for the adult human airway.20 The trachea component was scaled to match the cross-sectional area from images of the tracheal airway of adults16 and was prototyped using Tango Plus FullCure 930 (Objet Geometries, Billerica, Massachusetts), a viscoelastic material.18 Adjustments of cartilaginous ring thickness, esophageal interface thickness, esophageal interface width, and esophageal indention were made and tested to match reported non-linear in vivo data.18 The final dimensions of the tracheal model were 2 mm thickness for cartilaginous rings, 0.75 mm for esophageal interface thickness, 15 mm for esophageal interface width, and 2.15 mm for esophageal indention with a distance ratio between the anterior tracheal surface and the posterior esophageal crest to trough of 0.82. Validation of compliance matching was performed by inserting a 7.0-mm ETT with a standard cuff to the mid-tracheal position and using pressures of 0–30 cm H2O by incremental cuff inflation of 5 cm H2O pressure as measured by the Cufflator (Posey, Arcadia, California).
Ventilator Circuit Set-Up
The mouth-throat model was intubated with a 7.0 mm ETT and connected to a Nellcor Puritan Bennett 800 series ventilator (Covidien, Mansfield, Massachusetts) with 100% saturated air heated to 37 ± 0.6°C (ConchaTherm Neptune heated humidifier, Teleflex, Research Triangle Park, North Carolina). The distal bifurcating end of the trachea model was connected to 2 L anesthesia bags fully inflated to 2 L volume to represent a low compliant lung (Fig. 1) and maintained for 1 h for equilibration of the heated, humidified circuit before beginning the ETT cuff performance assessments. Ventilator settings selected for testing consisted of a flow of 40 L/min, tidal volume (VT) 500 mL, inspiratory time 1.0 s, and frequency 12 cycles/min. The ventilated mouth-throat model was elevated to 30° above the horizontal plane to reflect the practice of semi-recumbent positioning of intubated patients.

Intubated compliant trachea model set-up.
Mucus Simulant
Polyox water-soluble resin N-750 solution (Dow Chemicals, Woodbury, New Jersey) was used as the simulant for leak detection at a 0.25% concentration. A 0.5% Polyox solution, found previously to display characteristics similar to salivary secretions, was used in suction testing.21 The 0.25% simulant was made by heating 200 mL of deionized water to 95–97°C and adding 0.5 g of Polyox. The solution was removed from heat and mixed for 1–2 h until homogenous. Simulant secretions were dyed blue for visualization purposes. The rheology of the simulant (Table 1) was measured each day to ensure consistency throughout testing.
Rheology of Mucus Simulant
ETT Performance
Cuff performance of 3 7.0 mm internal diameter ETT designs (KimVent Microcuff, Kimberly-Clark, Roswell, Georgia; Mallinckrodt Hi-Lo, Covidien; and Sheridan/HVT, Teleflex) were evaluated within the trachea-ventilator circuit. These ETT designs displayed cuff material and geometry differences: polyurethane and cylindrical, polyvinylchloride and cylindrical, and polyvinylchloride and tapered, respectively. Testing occurred over cuff pressure of 5–25 cm H2O and PEEP of 0–15 cm H2O (Table 2). Triplicate testing of each ETT design was assessed for a period of 20 min under each test condition, with manometer (EndoTest; Rusch, Research Triangle Park, North Carolina) monitoring of cuff insufflation pressures. Five mL of simulant was added into the mouth of the model when testing 3 ETTs of each design for cuff seal performance, as measured by percentage of simulant leak past the cuff and VTe.
PEEP and Cuff/VTe Test Conditions
Two Humid-Vent Mini-filters (Teleflex) were placed at the bifurcation before the connection to the anesthesia bags to capture the colored simulant. The filters were removed after each test and submerged in 40 mL of saline. After 2 h of diffusion, the 40 mL saline-simulant solution was measured by an absorbance microplate reader (Biotek, Winooski, Vermont) to determine optical density. Leak percentage was determined by comparing the optical density of the sample with an optical density curve of known volumes of simulant diluted to 40 mL of saline. Test conditions with no visible cuff leak and a leak percentage less than 1% were considered to have zero cuff leakage.
ETT Subglottic Suction
ETTs with suction capability (TaperGuard Evac and ISIS HVT) were evaluated at 15 and 20 mm Hg continuous pressure and at 100 and 120 mm Hg intermittent suction pressure, using the bench ventilator-trachea circuit with constant cuff pressure and PEEP of 25 and 5 cm H2O, respectively. The ETT suction port was attached to a suction trap connected to a pressure regulator (Boehringer, Phoenixville, Pennsylvania). Suction efficiency was assessed as time required to aspirate 7 mL of 0.5% Polyox simulant and was tested in triplicate for each ETT design in both supine and lateral position. If mucus simulant was not completely cleared by 4 min, the test was stopped and deemed incomplete clearance. Occlusion of the suction channel was assessed visually by inward deviation of the posterior tracheal wall during suctioning, graded as complete (total obstruction with cessation of suctioning) or mild (disturbance of the posterior wall without impact on suction clearance).
Statistical Analysis
Data analysis was performed using the JMP Pro 10 statistics package (SAS Institute, Cary, North Carolina). Cuff seal and suction efficiency were analyzed by one-way analysis of variance and post hoc Tukey test. By convention, P < .05 was considered significant. A separate analysis of variance under each test condition was done to diminish heterogeneity caused by mixing results over all test conditions. We have displayed the results as box plots to show the range of data. Because the assessment of membrane occlusion was observational, no statistical test was applied.
This study was a laboratory investigation and employed no animal or subject participation, and therefore was exempt from the need for institutional review board approval.
Results
Simulant Leak Below the ETT Cuff
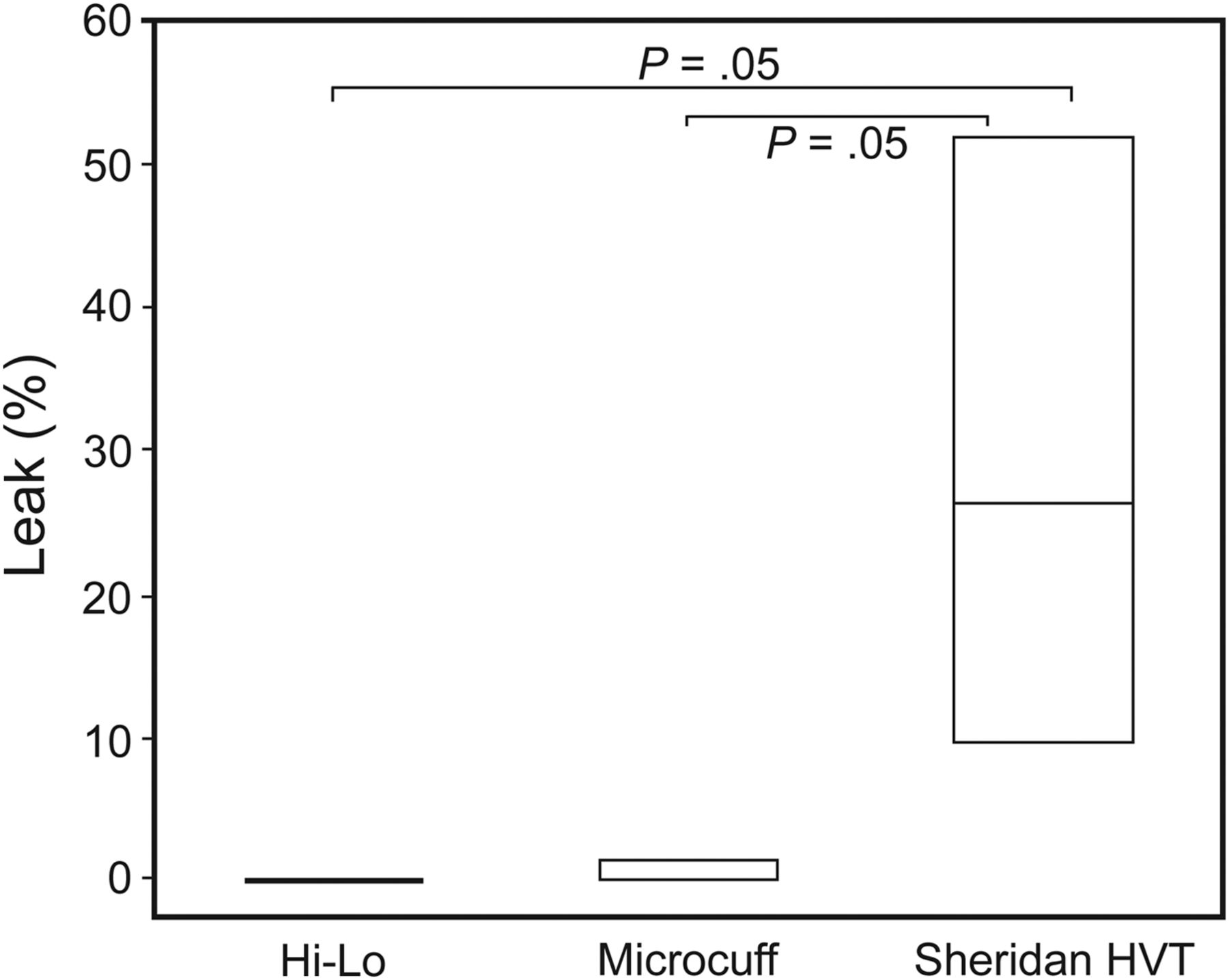
All ETT designs performed well with no simulant leak at cuff pressures of 10, 15, and 25 cm H2O, regardless of PEEP. Simulant leakage occurred only when no PEEP was present and at the low cuff pressure of 5 cm H2O. A significant difference in leak percentage was observed between the Sheridan/HVT and both Microcuff and Mallinckrodt Hi-Lo (P = .05), with a range of 0–29.3 ± 21.2% (Fig. 2).

Simulant leak percentage at PEEP of 0 cm H2O, endotracheal tube cuff pressure of 5 cm H2O. Box denotes full range of 3 data points.
Return Tidal Volume
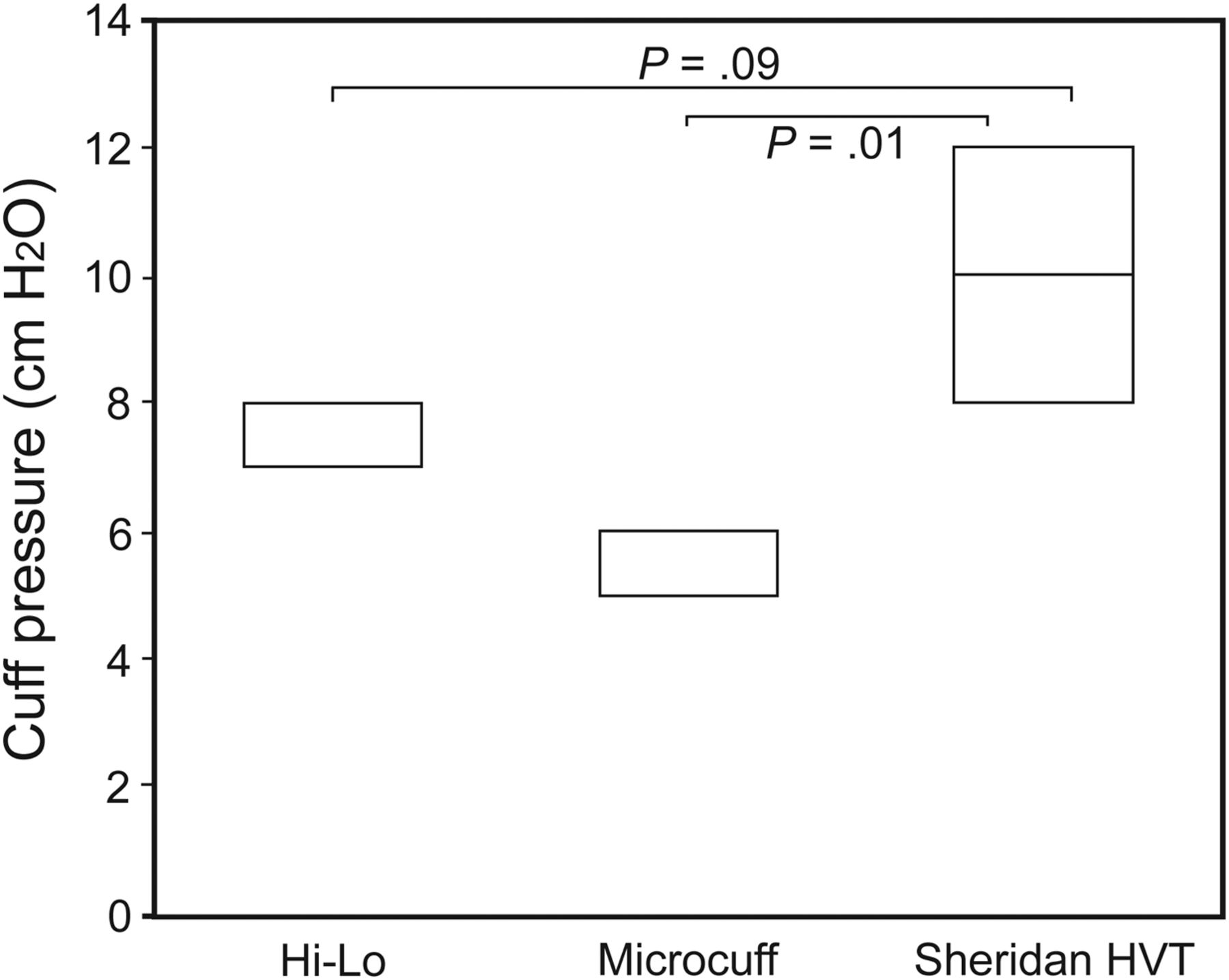
Increasing PEEP decreased the VTe in all tested ETTs. The lowest cuff pressure that maintained a VTe of 400 mL (>80% delivered, common clinical practice to minimize reinstrumentation by the vocal cords and yet be accommodated through leak compensation mechanics on current ventilators) varied with ETT design. When PEEP was 15 cm H2O (Fig. 3), the cuff pressure needed for the Microcuff ETT to maintain VTe > 400 mL was 16 ± 0.5 cm H2O, which is significantly less than the Sheridan/HVT cuff pressure of 21 ± 1 cm H2O (P < .01). During ventilation with PEEP of 5 cm H2O, all ETT designs maintained VTe > 80% delivered at a cuff inflation pressure of 12 cm H2O (Fig. 4). The Microcuff ETT sealed at the lowest insufflation pressure of 6 cm H2O, while the Sheridan/HVT cuff sealed at 12 cm H2O (P = .01).

Lowest endotracheal tube cuff pressure to maintain return tidal volume (VTe) ≥ 400 mL at PEEP of 15 cm H2O. Box denotes full range of 3 data points.

Lowest endotracheal tube cuff pressure to maintain return tidal volume (VTe) ≥ 400 mL at PEEP 5 cm H2O. Box denotes full range of 3 data points.
Subglottic Suction Channel
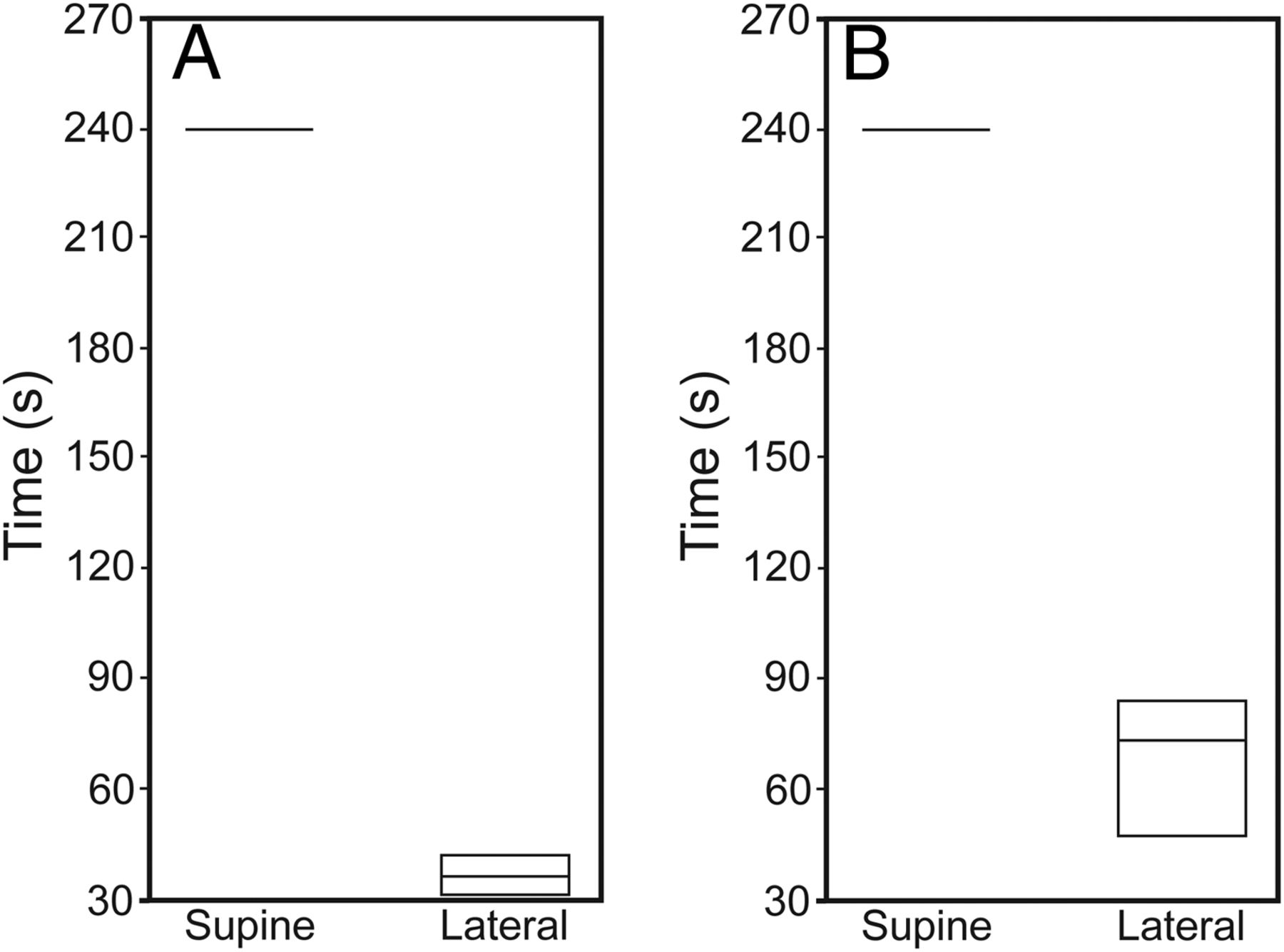
ETT suction channels cleared secretions in less than 3 s when using intermittent suction at pressures of 100 or 120 mm Hg regardless of the trachea position, supine or lateral. Neither suction channel design performed well in the supine position with continuous suction pressure of 15 mm Hg, failing to completely evacuate 7 mL of simulant by 4 min. However, at a slightly higher continuous suction pressure of 20 mm Hg, there was complete simulant clearance (Fig. 5). Rotating the trachea into a lateral position further improved the performance for both designs, with complete secretion clearance at the lowest suction pressure (15 mm Hg) tested (Fig. 6). There was no tracheal membrane displacement using low, continuous suction pressures. There was displacement of the posterior tracheal wall in both ETT designs using high intermittent suction pressures regardless of model position, although complete obstruction did not occur.

Suction channel efficiency (time) for complete simulant removal, at 15 mm Hg versus 20 mm Hg continuous suction pressure using A: ISIS HVT and B: TaperGuard Evac. Boxes denote full range of 3 data points. P < .01 between 15 and 20 mm Hg in both scenarios.
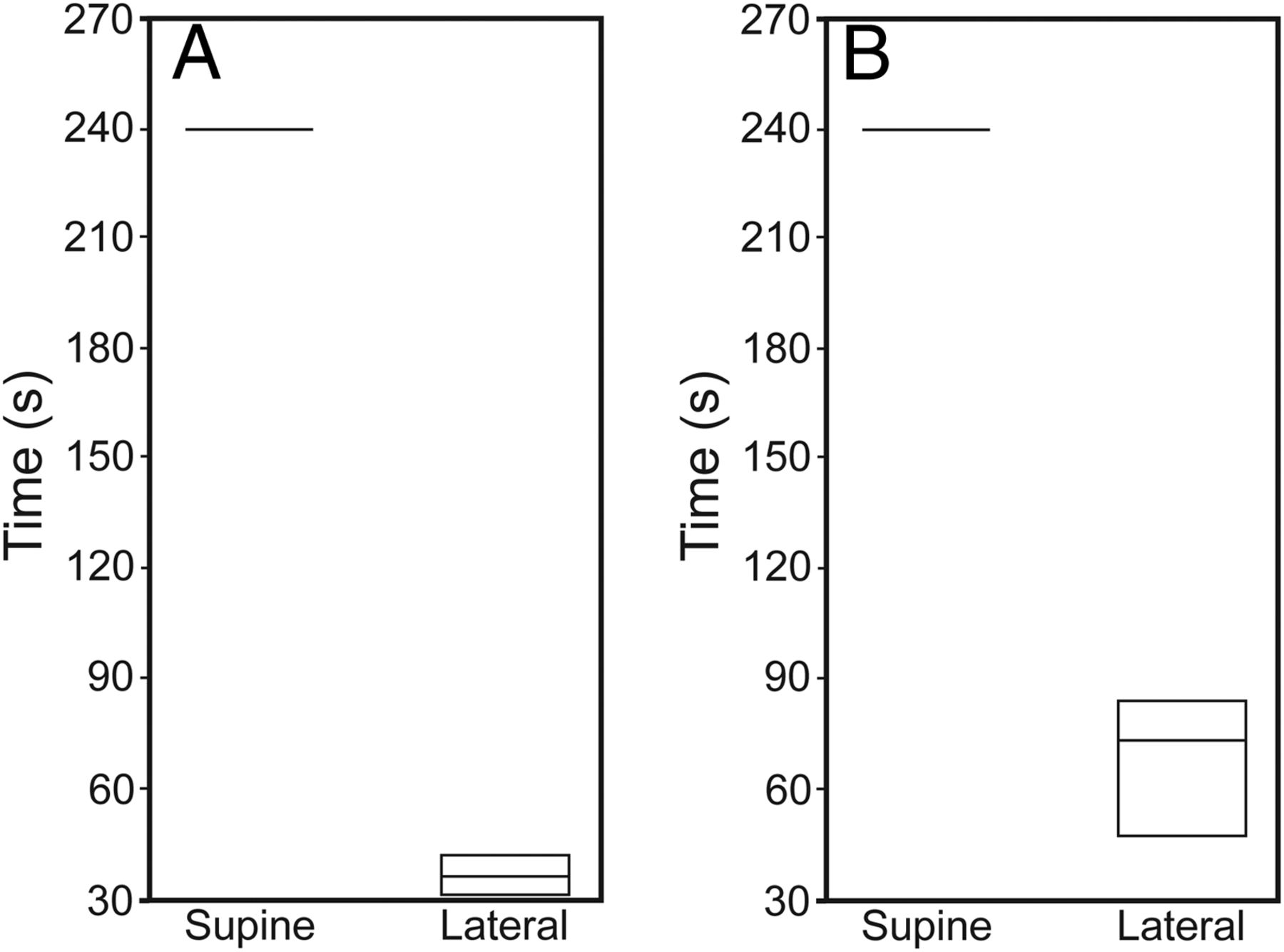
Suction channel efficiency (time) for complete simulant removal in supine versus lateral trachea position, under 15 mm Hg continuous suction pressure using A: ISIS HVT and B: TaperGuard Evac. Boxes denote full range of 3 data points. P < .01 between supine and lateral positions in both scenarios.
Discussion
Our objectives were to evaluate cuff seal effectiveness and the performance of the subglottic suction channel of different ETT designs using a novel, biorealistic tracheal model. To our knowledge, this is the first bench study of ETT performance using an airway model that matches the dynamic properties of the trachea. Young et al22 performed a combined bench and in vivo study of ETT performance using excised pig tracheas of approximately the same diameter as an adult human; however, the tracheae used were up to 1 day old, at which point tracheal compliance was lost due to cellular calcium leak into the tissue, causing muscle to rigor. In their model, leakage occurred in 44% of the endotracheal tubes tested, at the cuff pressure of 30 cm H2O, which is more consistent with leakage found in rigid trachea models than found in our study, where simulant leakage did not occur at cuff inflation pressures ≥ 10 cm H2O.
A significant limitation of our study may have been the use of fully inflated anesthesia bags to represent a low compliant lung. This may in itself have exaggerated the air leakage around the inflated cuffs (as measured by VTe) during testing. Nonetheless, within all ETTs tested, a cuff inflation pressure of 12 cm H2O or greater prevented secretion leakage and maintained VTe ≥ 80% delivered when PEEP was 5 cm H2O or less. This is lower than published recommendations that cuff pressure be maintained at 20–30 cm H2O.12,23,24 It is likely that compliance of the trachea diminishes the effect of cuff folding on leakage, possibly through the posterior membranous portion conforming around the cuff. In studies using a rigid airway model, only one ETT design, Microcuff, prevented air or secretion leak around the cuff at a similar lower inflation pressure of 15 cm H2O.7,8 This rigid model was not heated or humidified. Studies have suggested that moisture improves cuff seal by partially filling folds and cuff channels.23,25 Our study employed a humidified, heated circuit within the compliant trachea model.
The ETTs used in our study were those readily available to our institution and represent different cuff designs (cylindrical or tapered) and materials (polyvinyl chloride or polyurethane). Studies have demonstrated that cuff geometry and material affects performance, with improved sealing noted in polyurethane or silicone cuffs and tapered shape.6,8,9,22 Although we found performance differences between ETT designs, all ETTs tested provided an effective seal at cuff pressures lower than reported in studies using rigid tracheal models.
If compliance of the trachea plays a role in cuff sealing, then, at a higher airway pressure where there is decreased compliance, cuff sealing should be more difficult, requiring increased inflation to maintain effective seal. This has been demonstrated in vivo,26 and our study confirmed this effect of airway pressure on sealing. We found that, to maintain an effective VTe of ≥ 80% delivered at a PEEP of 15 cm H2O, an ETT cuff pressure up to 22 cm H2O was needed, considerably higher than the cuff pressure needed at low PEEP.
Our study design differed from many of the reported bench studies in regards to trachea positioning. We aimed to replicate patient care in a semi-recumbent position. This position decreases the gravity effects on secretions above the cuff and represents usual patient care practice. A study comparing different ETTs for fluid sealing and transmitted tracheal wall pressure similarly used the semi-recumbent position.6 The authors found a heterogeneous pressure distribution to the tracheal wall and proposed that increased folding of cuffs with larger outer diameter may play a role in this uneven pressure distribution. This study used a rigid trachea model, however, so the effect of tracheal compliance on the distribution of ETT cuff pressure or sealing was not assessed.
We evaluated suction channel performance in the supine and lateral positions. Better secretion clearance was found in the lateral position under low, continuous 15 mm Hg suction. Additionally, deviation of the posterior tracheal wall was observed at ≥ 100 mm Hg suction pressure, but complete occlusion of the orifice was not observed. This is likely due to using less than 3 s of high suction to clear the secretions. In clinical practice, suctioning intervals can vary. Tracheal trauma has been described primarily with continuous subglottic suction.27,28 Our finding of improved suction aspiration in the lateral position, allowing complete clearance of the secretions during continuous low 15 mm Hg suction pressure, may have clinical importance. Many institutions use a rotary bed or frequent repositioning of critically ill, intubated patients for prevention of skin breakdown, replicating this lateral position intermittently. Studies evaluating subglottic suction aspiration have not evaluated positional effect on secretion clearance or whether rotation may decrease mucosal injury during continuous suction techniques.
Aspects of ETT performance we did not address in this initial study of the compliant trachea model include replicating our findings of cuff seal performance with multiple sizes of ETTs. Only one size of ETT was tested due to cost constraints. We also chose to observe for leakage over 20-min intervals; this may not be the optimal interval for assessment of ETT performance within a compliant tracheal model, and clearly does not represent a protracted intubated patient experience. Cuff pressures were continuously monitored and maintained, whereas, in clinical practice, there is drift in cuff pressures over time.29 Movement or suctioning of ETTs with under-inflated cuffs has also resulted in higher rates of micro-aspiration.22,30 We did not manipulate our trachea model by suctioning or movement during the study. Further testing with multiple sizes of ETTs and under the movement conditions similar to patient care within this new, biorealistic tracheal model are needed.
Statistical analysis in this pilot study of a new compliant trachea model is limited due to the small number of ETTs tested. Extended work within the compliant trachea model, replicating and expanding these preliminary findings of a lower cuff pressure providing adequate sealing properties that prevent secretion leakage is needed before considering a change from current recommended cuff inflation pressures.
Conclusions
Using a novel in vitro tracheal model with dynamic characteristics matching that of an adult human airway, we demonstrated that tracheal compliance has an effect on ETT cuff performance. We found lower cuff pressures than currently recommended provided an effective seal against secretion leakage when PEEP was ≤ 5 cm H2O with a cuff threshold pressure of 12 cm H2O for sealing. At higher airway pressures where tracheal compliance is diminished, higher cuff pressure was required to maintain effective VT. We further found suction channel performance at low (15 mm Hg) continuous suction pressure to improve with rotation to a lateral position. Additional studies to expand this appreciation of the innate tracheal compliance effect on cuff performance are needed.
Acknowledgments
We thank Drs Walenga and Longest for the design and development of the compliant tracheal model we used in this study.
Footnotes
- Correspondence: Norma J Maxvold MD, Children's Hospital of Richmond, Virginia Commonwealth University, Box 980530, Richmond, VA 23298. E-mail: nmaxvold{at}mcvh-vcu.edu.
Ms Rozycki presented a version of this paper at the American Association for Respiratory Care Congress, held November 16–19, 2013, in Anaheim, California.
This study was supported by a research grant from Teleflex Medical, Research Triangle Park, North Carolina. Ms Rozycki received travel expense support for the abstract presentation at the American Association for Respiratory Care Congress from Teleflex Medical. Mr Dixon is employed by Teleflex Medical. Dr Rubin's laboratory received research funding for this study from Teleflex Medical. All other authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}