

Abstract
Endobronchial chondromas are rare benign tumors. They may be part of the Carney triad; however, isolated endobronchial chondromas can occur in the larynx, trachea, and bronchi. We report a case of an endobronchial chondroma in a 61-y-old man with an incidental 5-mm endobronchial polypoid lesion at the proximal left main bronchus that was later found to be an endobronchial chondroma. Flexible bronchoscopy demonstrated a pedunculated, vascularized, pink mass. An excisional biopsy revealed a well-circumscribed lesion with nodular areas of mature cartilage and myxoid tissue confirmatory of an endobronchial chondroma. We reviewed a total of 23 cases of isolated endobronchial chondromas reported in the medical literature. Despite their rarity, endobronchial chondromas should be considered in the differential diagnosis of endobronchial tumors. Prompt recognition and resection of endobronchial chondromas is important to prevent airway obstruction and its associated complications.
Introduction
Chondromas are considered rare benign tumors. However, the true incidence of chondromas is unknown, as they have been historically misclassified as hamartomas.1,2 Endobronchial chondromas may be part of the Carney triad. The Carney triad is a rare non-hereditary condition affecting young women that also includes gastrointestinal stromal tumors (gastric epithelioid leiomyosarcoma) and extra-adrenal paragangliomas.3 Isolated endobronchial chondromas not associated with the Carney triad are extremely rare.
We present a case of an incidentally detected endobronchial chondroma on a chest computed tomography (CT) scan that was histologically confirmed by a bronchoscopic biopsy. A search of the literature using MEDLINE and the LILACS Database for the key words “chondroma” alone and in conjunction with various terms such as “bronchi” and “lung” was carried out. After excluding chondromas associated with the Carney triad, a total of 23 cases were identified for this review.
Case Report
A 61-y-old Hispanic man was seen in a smoking cessation clinic. He had 35 pack-year history of smoking as well as hypertension, obesity, obstructive sleep apnea, and hyperlipidemia and had recently undergone repair of an abdominal aneurysm. He reported mild dyspnea on exertion, with no other respiratory symptoms. On physical examination, he appeared in no acute distress, with normal vital signs. Chest auscultation revealed bilaterally decreased breath sounds with no wheezing or crackles. A complete blood count and serum chemistry were within normal limits.
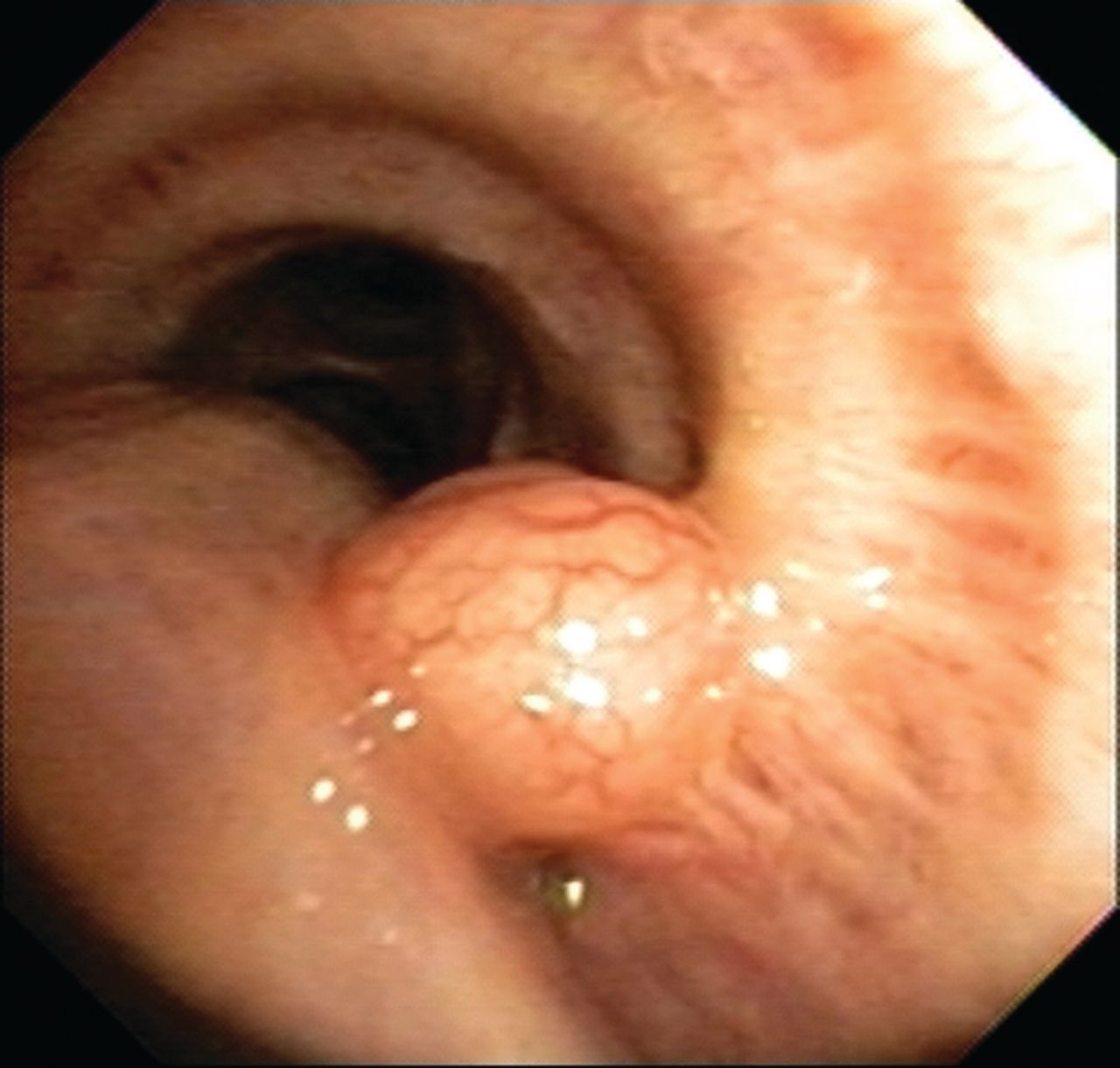
A chest x-ray showed hyperinflation of the lungs. A follow-up chest and abdominal CT scan done after abdominal aortic aneurysm repair showed a 5-mm endobronchial polypoid lesion at the proximal portion of left main bronchus (Fig. 1). Flexible bronchoscopy (BF-Q180 video bronchoscope, Olympus, Miami, Florida) confirmed a pedunculated, vascularized, pink mass at the medial aspect of the proximal left main bronchus. Subsequently, an excisional biopsy of the lesion was performed using an electrocautery snare for removal of the lesion. Thereafter, the patient had an uneventful recovery (Fig. 2).
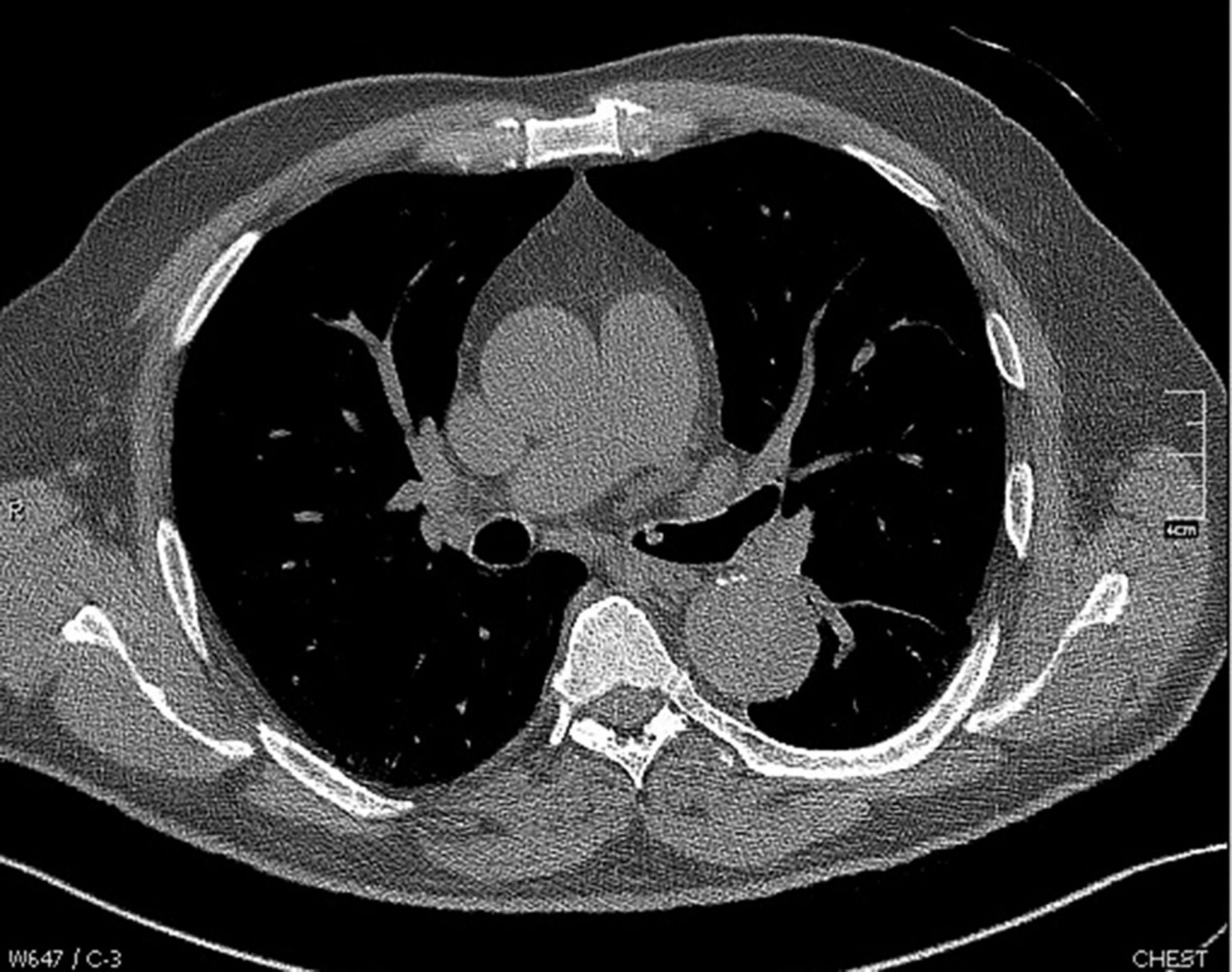
Chest computed tomogram demonstrates an endobronchial lesion in the proximal left main bronchus.

Bronchoscopic image demonstrating a polypoid, vascularized, pink tumor growing on the medial wall of the left main bronchus.
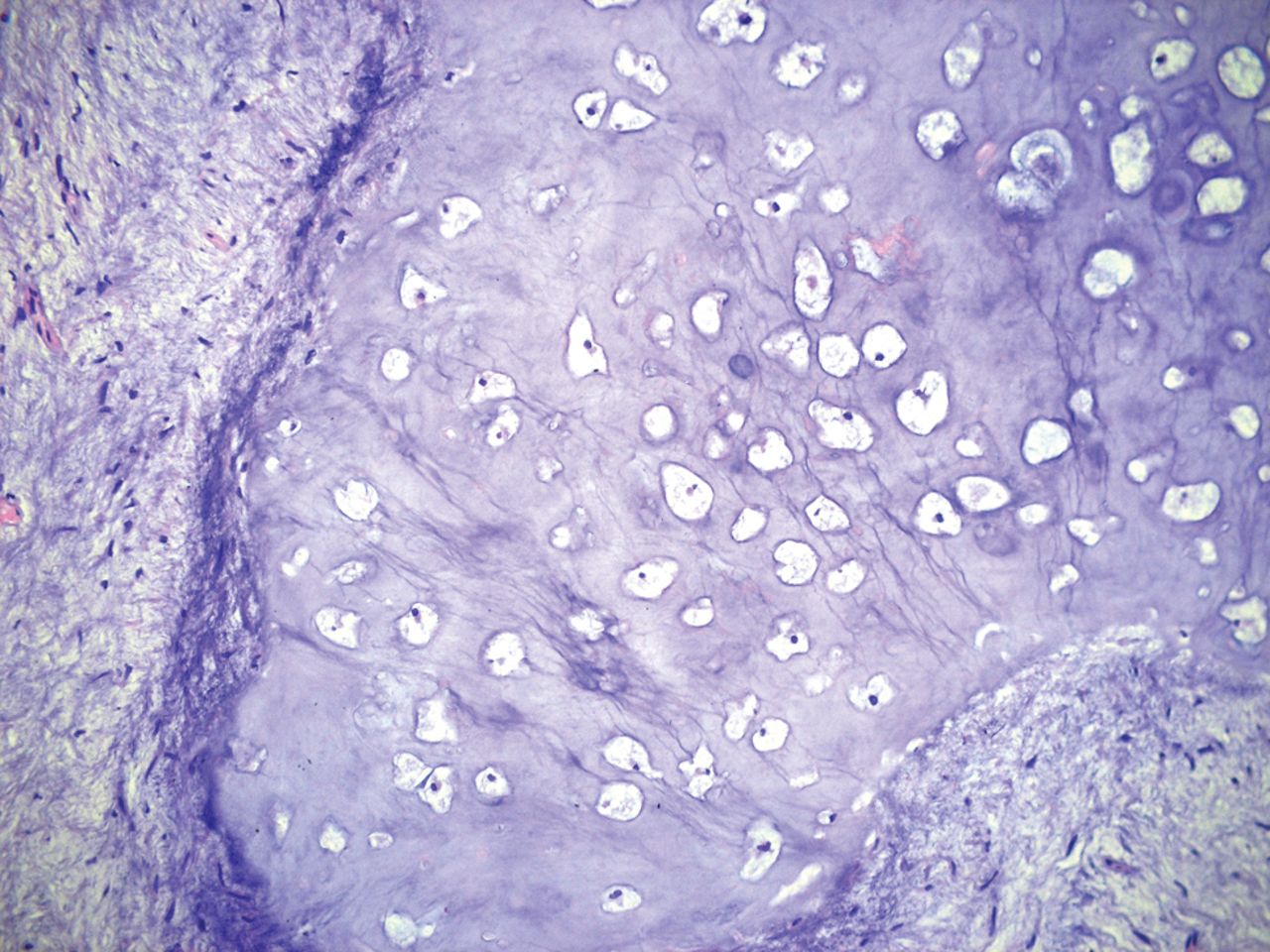
Histological samples revealed a well-circumscribed lesion consisting of nodular areas of mature cartilage and myxoid tissue, without evidence of epithelial lined clefts. At higher magnification, the myxoid and hyaline cartilage demonstrated low cellularity and bland nuclei (Fig. 3). Given the association of endobronchial chondromas with gastrointestinal tumors and extra-adrenal paragangliomas, an upper gastrointestinal endoscopy and abdominal CT were performed and found to be normal, thereby excluding the Carney triad. After 24 months of follow-up, a chest CT showed no evidence of recurrence.

Myxoid and hyaline cartilage components with low cellularity and bland nuclei.
Discussion
Benign tumors of the tracheobronchial tree are rare. Gaissert et al2 reported that benign tumors constitute 0.2% of all lung tumors in adults in the United States. Histologically, the most frequent benign tumors are papillomas and hamartomas; chondromas are uncommon.2
Chondromas are made entirely of benign mature hyaline cartilage and characteristically lack internal clefts lined by alveolar epithelium. The related mesenchymal tumors and hamartomas may have adipose tissue, muscle, or bone. Chondromas grow in bones and more frequently in the axial skeleton, synovial sheaths of tendons, or soft tissue adjacent to tendons in hands and feet. Endobronchial chondromas can appear in the larynx, trachea, or major bronchi,2 although they are more frequently observed in the trachea than in the bronchi.3–26
The differential diagnosis for the radiologic image of a chondroma includes hamartomas, tracheal amyloidosis, mucus plugs, and lung cancer. A hamartoma can be distinguished by the presence of bone and fat tissue on a chest CT. However, histologic confirmation is frequently advised in other conditions. A well differentiated chondrosarcoma can sometimes mimic a chondroma.2,4,5 The presence of tissue invasion, metastatic lesions, or mitosis should be further investigated, given the risk of chondrosarcoma or other metastasis.
Treatment consists of complete excision through bronchoscopy or surgery. Given the small number of cases reported, there is no consensus regarding the best approach.4–26
Review of the medical literature through MEDLINE and the LILACS Database identified a total of 23 cases of endobronchial chondromas. The male/female ratio was ∼3:2, with an average age of 46.3 ± 17.83 y. These findings differ from those for chondromas found as part of the Carney triad, where female predominance is observed. Notably, only 2 cases were asymptomatic. In 11 cases (45.8%), cough and dyspnea were associated with bronchial hyper-reactivity or asthma, and 2 presented with isolated chest pain. No significant association between comorbidities and bronchial chondromas were found, and only 5 subjects were active smokers. A summary of the published cases with demographics, clinical presentation, diagnosis, treatment, and outcomes is provided in Table 1.1–26
Summary of the Published Cases of Isolated Endobronchial Chondromas
In most cases, chest x-ray revealed lobar consolidation or atelectasis. Among those who had a chest CT, the main finding was an endobronchial lesion measuring < 3 cm, generally occluding a bronchus. Eleven cases (45.8%) involved the right bronchus. The most common bronchoscopic findings were pedunculated, vascularized, pink tumors. Histologic analysis of the biopsies showed characteristic chondromatous tissue, although there were exceptions that presented with myxoid stroma mixed with chondromatous tissue.
The reported treatments varied widely and included resection of the tumor through different techniques (bronchoscopy, video-assisted thoracoscopic surgery, or thoracotomy). In 7 cases, treatment consisted of endoscopic resection, and surgical treatment was reported in 17 cases, mostly between 1945 and 1980. None of the individuals died or had serious complications.
The most common reported clinical outcomes were symptom relief and radiographic resolution. The follow-up data were frequently insufficient, but 22 of the 23 cases (95.6%) that were reported showed no recurrence of the tumor. Only one case presented 2 episodes of recurrence.
In conclusion, isolated endobronchial chondromas not associated with the Carney triad are extremely rare. Bronchoscopy is a safe and useful tool to diagnose and treat chondromas. Resection of endobronchial lesions is important to prevent progression of respiratory symptoms. Further studies with detailed descriptions of treatments and long-term outcomes are needed to guide therapeutic recommendations.
Footnotes
- Correspondence: Sebastian Fernández-Bussy MD, Division of Interventional Pulmonology, Clínica Alemana, Universidad del Desarrollo, Manquehue Norte 1410, Santiago, Chile 7650567. E-mail: sfernandezbussy{at}alemana.cl.
The authors have declared no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}